










Services on Demand
Journal
Article
 text in
text in  Portuguese (pdf)
Portuguese (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkEnfermería Actual de Costa Rica
On-line version ISSN 1409-4568Print version ISSN 1409-4568
Enfermería Actual de Costa Rica n.45 San José Jul./Dec. 2023
http://dx.doi.org/10.15517/enferm.actual.cr.i45.49923
Original Article
Flower therapy effect on the quality of professional life in nursing residents: pilot study

1 Bacharel em enfermagem. Escola de Enfermagem da Universidade de São Paulo. Departamento de Enfermagem Médico-Cirúrgica. São Paulo. Brazil. ORCID: 0000-0002-0878-9793
2 Enfermeira. Professor Doutor. Escola de Enfermagem da Universidade de São Paulo. Departamento de Enfermagem Médico-Cirúrgica. São Paulo. Brazil. ORCID: 0000-0001-8689-5762
3 Enfermeira. Professor Doutor Livre Docente. Escola de Enfermagem da Universidade de São Paulo. Departamento de Enfermagem Médico-Cirúrgica. São Paulo. Brazil. ORCID: 0000-0002-4910-7672
Introduction
One of the great challenges for nursing is dealing with the multiple stressors faced in its work environment. The factors that generate illness are the intense workload, unexpected situations that cause anguish, and the devaluation of the work, leading to frustration, and the physical and mental exhaustion of the worker.1
The quality of professional life is a term that illustrates the levels of occupational stress and is related to “the quality of someone's feeling in relation to their work as a helper”. For Stamm,2 it is influenced by three factors: compassion satisfaction, burnout and secondary traumatic stress, with the professional being more affected when they can no longer deal in a healthy way with the negative feelings that emerge from the suffering of the patients they assist.
Studies on this phenomenon in the work context of healthcare providers3 have become an important topic in recent years, considering that the work relationship in health is strongly marked by ambivalence in feelings of suffering and reward during the care.
The quality of professional life can also be affected by activities that include providing care, with this also happening with nursing residents. In Brazil, the Residency in Nursing is a latu sensu postgraduate course funded by the federal government that enables training and professional qualification of newly graduated nurses when they enter the field of work. This postgraduate course includes 5.760 hours, in which 80% of the total workload is practical activities and 20% theoretical-practical activities, so that a workload of 60 hours per week is performed over two years.4 This workload of extensive work and the alternation of shifts may imply a decrease in time for eating, leisure, rest, sleep and social and family contact.1
Studies on stress among residents show prevalences that tend to exceed 50%.5,6A study carried out in Brazil that assessed the stress of nursing residents using the Nursing Student Stress Assessment scale showed that the most prevalent domains of stress were Professional Training (68%) and Professional Communication (54%).7
With the recent COVID-19 pandemic, health services entered into a scenario of actions and health safety aimed at the various professionals involved in caring for the population.8 Chinese research9 found that nurses were at high risk of occupational exposure while caring for patients with COVID-19. Given the extensive workload, nurses were forced to use a complete set of personal protective equipment, which limited breathing.9 Physical and mental strain was greater as the weekly work time increased, exposing the body to a state of tension and fatigue, which when continuous and prolonged can lead to exhaustion. Exposure to anxiety, an important factor for nurses' stress burden, and burnout, related to physical and mental health, affect the quality and safety of the work of nurses,9a category that also includes nursing residents.
In this scenario, the Integrative and Complementary Health Practices (ICHP) transcend several issues and encompass not only the individual's life habits, but their relationship with social and family groups, their insertion at work and their entire sociocultural context. The analysis of the literature demonstrates that ICHP can help improve the quality of professional life by presenting effective results in reducing tension, anxiety and stress, providing well-being, relaxation and energy rebalancing of the body as a whole.10 In this sense, ICHP can be a tool to improve the quality of professional life, as this is influenced by the satisfaction and well-being of the care provider in the performance of their duties.11
In Brazil, since 2006, there has been a national public health policy that includes access to ICHP in the Brazilian public health system.12 Integrative and Complementary Health Practices involve approaches that seek natural mechanisms for preventing injuries and recovering health through effective and safe technologies , with an emphasis on empathic listening, the development of the therapeutic bond and the integration of the human being with the environment and society.12 One of the ICHP is flower therapy.
Flower therapy is considered a vibrational therapeutic practice that uses plants and flowers that act on the most subtle level of the person, helping in emotional and mental harmonization, thus favoring relief and recovery.13 The theory of quantum fields has allowed the generation of hypotheses yet to be tested on the action mechanism of flower therapy. Aqueous systems can modulate biological function by processing, storing and retrieving information mediated by electromagnetic signals (information) that mimic the effects of a given matter,14 in this case, the flower of Bach's system of flower essences when the flower remains immersed in natural water under sunlight. This information becomes resonant with the coherence domain of the water and when administered it favors quantum coherence and the assimilation of virtues by the individual. “This transmission takes place through a frequency of wave energy that carries 'information' into action, and activates cell membranes, provoking specific biochemical responses capable of altering the biological response that coordinates neurotransmitters, neuropeptides and hormones, modulating the way of thinking, feeling and acting.”15
Benefits are observed in the use of five associated florals that make up the so-called Rescue Remedy®, indicated for emergency situations, crisis, and stress, among others, as observed in the reduction of high levels of situational anxiety in nursing students.16 The Rescue Remedy® is composed of five flower essences: Rock Rose (Heliantnemum vulgare), used in cases of great urgency, intense fear, extreme needs, and situations that seem hopeless; Impatiens (Impatiens glandulifera), used in very severe pain, lack of patience, anxiety to get back to normal or get well quickly, and intolerance of those around; Cherry Plum (Prunus cerasifera), applied for lucidity in difficult moments; Star of Bethlehem (Ornitholagum umbrellatum), which helps to heal shocks and physical or emotional traumas, and Clematis (Clematis vitalba), used to help focus and recovery in cases of tiredness and apathy.13
In the present study, the Rescue Remedy® was used with the addition of the Walnut (Juglans regia) flower, which was called FiveW in this study. The association of Walnut with the Rescue Remedy is justified because it is a recommended essence for adapting to new situations that involve transitions with no perspective of the future result and with repercussions on the physical and mental state, as occurred during the pandemic, requiring psycho-spiritual protection faced with suffering in the care of affected patients.17
Given the importance of caring for those who provide care, and considering the lack of studies focused on the quality of professional life in nursing residents, the present study aimed to verify the effect of Bach flower therapy on the components of quality of professional life (Compassion Fatigue - Burnout and Secondary Traumatic Stress - and Compassion Satisfaction) in nursing residents in the context of the COVID-19 pandemic. The hypothesis was that flower essence therapy could positively impact the quality of professional life.
Methodology
Study design and participants
This was a quasi-experimental pilot study, of the before and after follow-up type, carried out from May/2020 to January/2021. The sample was a group of resident nurses specializing in the areas of Obstetric Nursing, Pediatrics (Child and Adolescent Health) and Adult and Older Adult Health; Cardiology/Pulmonology and Clinical Care Specialized in Neonatology, from public hospitals; and Clinical Surgical, from a private hospital, all being teaching hospitals in southeastern Brazil. Participants were volunteer residents who met the following inclusion criteria: a) being a nursing resident in the first (R1) or second (R2) year of any specialty and b) achieving a score > 21 in the Burnout subscale of the Professional Quality of Life Scale 4 (ProQOL-4), to include residents with moderate to severe scores and to be able to identify any improvements in the score. This subscale was applied via e-mail, two weeks before starting the study with the included participants. Exclusion criteria were: a) use of any other complementary health therapy; b) initiation of treatment with anxiolytics and/or antidepressants during the study; and c) being pregnant or lactating, for ethical safety reasons. Interruption of treatment or withdrawal during the intervention period were considered as losses. A non-probabilistic convenience sample was established, in which all nursing residents of the aforementioned hospitals were invited to participate. A total of 24 residents were recruited to achieve the outcome of professional quality of life measured by the Professional Quality of Life Scale - ProQOL-4.18
Intervention
A bottle of FiveW was delivered to each participant by the teaching researchers of the present study. The intervention consisted of administering the flower essence orally, at a dose of four drops, four times a day (upon waking up, after lunch, at the end of the day and before going to bed), for 21 days. Participants received a video via email, produced by two undergraduate students, with instructions on how to use the flower formula. The flower formula bottles used were donated by a supplier. The researchers themselves paid for the other costs of the study.
Monitoring of adherence to treatment was carried out weekly, via telephone, by the two undergraduate students. All participants started the intervention simultaneously.
Data collection instruments
A questionnaire was prepared for sociodemographic characterization (age, gender, specialty, use of continuous medication, allergy, use of ICHP, participant's or family's COVID-19 history).
The ProQOL-4 scale is an instrument translated, adapted, and validated for Brazil by Lago and Codo,18 which assesses the quality of professional life through three subscales that assess two phenomena: Compassion Satisfaction and Compassion Fatigue, the latter being composed of Burnout and Secondary Traumatic Stress subscales. The lower the Compassion Satisfaction score and the higher the Burnout and Secondary Traumatic Stress scores, the more overwhelmed and distressed the person is in the work environment.2 Consisting of 28 items scored on a Likert-type scale (1 to 5), the validated scale has two items less than the original version, which were removed during validation to improve the instrument's psychometric properties. The scale is divided into three subscales that assess three distinct phenomena: Compassion Satisfaction, Burnout and Secondary Traumatic Stress and its score varies from 28 to 140. In addition to the 28 items, the initial part of the scale also contains four questions, called ProQOL-A, ProQOL-B, ProQOL-C, ProQOL-D with Likert-type responses. These questions are intended to characterize the profile of patients who are assisted by the professionals that respond to the scale.
Recruitment and data collection procedure
The dissemination of the study to the residents was carried out in a class of the residency course, by a teaching researcher and by the two undergraduate students. Interested parties were contacted by the two undergraduate students via email, in order to present the research objectives. Residents who consented to participate, electronically signed the consent form authorized by the institution. Due to the pandemic, the only face-to-face contact with the residents was for the delivery of the flower formula bottle.
The two undergraduate students carried out a virtual interview to apply the data collection instruments. The ProQOL-4 scale was applied at three times: 1) before the beginning of the intervention (one day before the participants started the first dose), 2) after three weeks of using the flower essence therapy and 3) three weeks after the end of the intervention (follow up).
Data analysis
Data were entered into a Microsoft Excel® spreadsheet and analyzed by a statistician using the R 4.1.1 software (R Core Team, 2021). The ProQOL-4 scale was analyzed as recommended for the original scale (excluding items removed in the Portuguese validation): Compassion Satisfaction (items 3,6,12,16,18,20,22,24,27,30), Burnout (1r,4r,8,10,15r,17r,19,21,26) and secondary traumatic stress (2,5,7,9,11,13,14,23,25). Items with the letter 'r' refer to items that are reversed for the scoring analysis. Data analysis used measures of central tendency and variability, Kendall's Tau correlation for the items ProQOL-A, ProQOL-B, ProQOL-C and ProQOL-D with the subscales, Student's paired t-test with the mixed effects model to compare pre- and post-treatment, and Cohen’s d for the effect size, with the variables 'having been ill with COVID-19', 'close person having been ill with COVID-19', and the 'year' and 'specialty' of residency used in the interaction analysis. Effect size was assessed through Cohen’s d. The level of significance considered was 5%.
Results
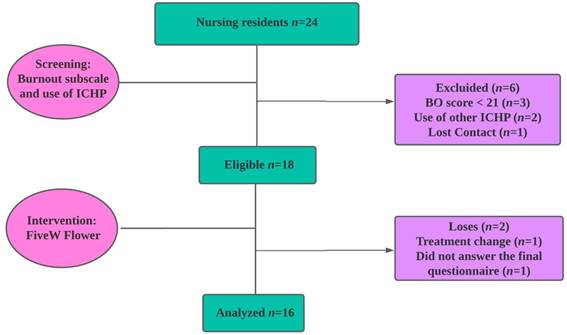
Of the 24 residents recruited, five were excluded because they used other ICHP (2) or did not achieve the minimum score for the Burnout subscale (3), since these conditions were considered to be confounding variables. Accordingly, 19 residents were eligible, however, contact was lost with one participant and, therefore, 18 residents started the study. There were two losses throughout the study: one resident did not answer one of the questionnaires and the other started treatment with psychotropic drugs, fulfilling the exclusion criterion, as this was considered to be a confounding variable (Figure 1).
Screening with the Burnout subscale showed a mean score of 26.1 (SD ± 4.2), corresponding to a moderate level of Burnout.
Participants were all female, with a mean age of 24.5 (SD ± 3.0; median = 24) years. Half were in the first year of the residency and the rest in the second year, with nine (56.3%) working in the Adult Health area, six (37.5%) in Obstetrics and one (6.2%) in Pediatrics (Child and Adolescent Health). All professionals had less than two years of experience as nurses and the daily workload was 12 hours. Regarding the history of COVID-19, nine (56.3%) residents had already contracted the infection, 12 (75.0%) had someone close to them who fell ill with the coronavirus, and four (33.3%) of these close people needed hospitalization.
Regarding work, there was a predominance of the responses “very often or often” in the ProQOL-A item (Do you care for people who are suffering?) (n = 10; 62.5%) and in the ProQOL-B item (Do you care for people at risk of death?) (n = 8; 50.0%). For item ProQOL-C (Do you care for people who have gone through a traumatic event such as sexual abuse, assault, aggression?) the responses “sometimes or rarely” predominated (n = 12; 75.0%). In the ProQOL-D item (Do some of the cases that you care for affect you?) most responses were “often or sometimes” (n = 12; 62.5%) (Figure 2).
There was a positive correlation between the ProQOL-A item and Burnout (p = .039; 95%CI -0.09; 0.76, between the ProQOL-D item and Secondary Traumatic Stress (p = .026; 95%CI (-0.05; 0.78) and with Compassion Satisfaction (p = .047; 95%CI (-0.11; 0.75), however the confidence intervals showed wide amplitude with the possibility of a negative coefficient.
The comparative analysis before and after the intervention showed that the Bach flower therapy helped to reduce the Secondary Traumatic Stress score (p = .017) with a residual effect at follow-up. The effect could not be verified in Compassion Fatigue as it also included the Burnout subscale, which did not change with the use of the Bach flower therapy (Table 1).
Table 1: Measures of central tendency, variability and Student's t-test (p value) of the ProQOL-4 scale scores in nursing residents, according to the study phase. Brazil, 2021.
| ProQOL / Phase | Before | After | Follow-up | p (Before - After) | p After - Follow up |
|---|---|---|---|---|---|
| Compassion Satisfaction | |||||
| Mean (SD) | 37.5 (3.6) | 35.7 (4.9) | 35.8 (4.0) | 1.000 | .973 |
| 95%CI | (35.6; 39.1) | (33.2; 37.8) | (33.6; 37.4) | ||
| Burnout | |||||
| Mean (SD) | 25.6 (5.2) | 24.6 (4.9) | 25.9 (4.3) | ||
| 95%CI | (23.2; 28.1) | (22.5; 27.2) | (23.8; 27.9) | ||
| Secondary Traumatic Stress | |||||
| Mean (SD) | 21.4 (5.8) | 17.6 (4.7) | 18.4 (5.8) | .017 | .752 |
| 95%CI | (15.8; 21.2) | (15.6; 20.0) | (15.8; 21.2) | ||
| Compassion Fatigue | |||||
| Mean (SD) | 47.0 (10.2) | 42.2 (9.8) | 44.2 (9.8) | .059 | .717 |
| 95%CI | (42.2; 51.9) | (38.3; 46.9) | (39.8; 49.1) | ||
For Compassion Fatigue and its subscales (Burnout and Secondary Traumatic Stress) there was an interaction with the specialty of the residency program (Figure 3). The residents of the Adult and Older Adult Health specialization area presented a reduction in the Compassion Fatigue score at the end of the intervention (p = .026), unlike the residents of other areas. In the Burnout subscale, the one resident in the Pediatrics area had a lower score than the participants in the other areas (p = .008).
Figure 3: Effects of Bach flower essence use on the ProQOL-4 subscales throughout the evaluation phases, according to specialty and year. Brazil, 2021.
For Secondary Traumatic Stress and Compassion Fatigue, there was interaction with the specialty of the residency program. In the analysis of Secondary Traumatic Stress, there was evidence of a main effect of the specialty (p = .044), in which residents of Obstetrics, and Adult and Older Adult Health presented lower scores in Secondary Traumatic Stress at the end of the intervention, which was very different in relation to the Pediatrics resident. A similar effect was observed in Compassion Fatigue, which sums the Burnout and Secondary Traumatic Stress subscales (p = .012).
Regarding the year of the residency program, in Compassion Satisfaction, there was a reduction in the score of first-year residents (p < .001) compared to the second-year residents (Figure 4). In Burnout, although the interaction between the phase and the year showed that the second-year residents benefited from the use of the Bach flower essence (Figure 4A), there was no statistically significant difference (p = .058).
Residents who had a close person infected with COVID-19 had different scores throughout the study (Figure 4) in Burnout (p = .004), Secondary Traumatic Stress (p = .027) and Compassion Fatigue (p = .008).
Figure 4: Effects of the Bach flower therapy on the ProQOL-4 subscales throughout the evaluation phases, comparing those with and without a close person affected by COVID-19. Brazil, 2021
Effect size analysis showed a relative reduction of 18% (d = .74) in Secondary Traumatic Stress after 21 days of intervention and 14% (d = .53) at the follow-up compared to baseline, considered a medium effect size. The effect sizes for Compassion Satisfaction and Compassion Fatigue at the end of the intervention were also medium, 5% and 10% respectively.
Discussion
The majority of participants in this study were nursing residents who experienced work-related suffering while caring for patients in life-threatening situations. This creates an environment that fosters feelings of dissatisfaction, exhaustion, and stress. These negative emotions are associated with a range of cognitive, emotional, and physical demands encountered in daily patient care, ultimately leading to a decreased quality of professional life. A study on stress in multidisciplinary residents of a public hospital evaluated through the Stress Symptoms Inventory for adults demonstrated a prevalence of stress of 78.9%, with 64.3% in the resistance phase.6
A systematic review on Compassion Fatigue involving 28,509 nurses from 11 countries observed a mean score of 33.1 for Compassion Satisfaction, 26.6 for Burnout, and 25.2 for Secondary Traumatic Stress.19 The present study in residents showed a higher mean for Compassion Satisfaction and lower for Secondary Traumatic Stress. The higher mean was similar to the Chinese study with newly graduated nurses, which showed a Compassion Satisfaction score of 37.9 and its association with greater resilience.20
An electronic survey conducted with Korean nurses during the pandemic showed a mean Secondary Traumatic Stress score of 31.2, considered moderate. The factors that influenced Secondary Traumatic Stress were caring for patients with COVID-19 for more than 30 days and working in a hospital not structured to care for these patients, while the support of a friend as social support was a significant factor in dealing with Secondary Traumatic Stress.21
The ICHP have been adopted to support new graduates in their transition to the workplace. An intervention with the Stress Management and Resiliency Training (SMART) program in nursing residents, which aims to improve individual attention skills and interpretation refinement, showed a significant improvement in stress, mindfulness and resilience, despite limited adherence to the stress protocol of the intervention.22
Flower essence therapy seeks to develop these skills, based on a greater self-perception, in a process of observing and transforming reaction patterns faced with situations that can disharmonize the individual. The present study, when verifying evidence of a significant reduction, mainly in Secondary Traumatic Stress, after the use of the FiveW flower formula, reinforces literature findings16 on the effect of the Rescue Remedy® essences in traumatic experiences experienced at work, such as witnessing the pain and suffering of sick people. The inclusion of Walnut essence in the composition of the Rescue Remedy® is related to the fact that this flower offers protection for the increased sensitivity to external influences,23in this case the suffering of others, so as not to lose focus.
The concepts of Burnout and Secondary Traumatic Stress presented by Stamm2 allow us to identify that the flower essences that make up the FiveW are closer to the signs and symptoms verified in Secondary Traumatic Stress than in Burnout.
Considering the psychological symptoms observed in a study with multidisciplinary residents in the stress resistance phase, such as thinking focused on one subject (52.8%), self-doubt (50.0%), irritability and excessive sensitivity (47.2%), and in the exhaustion phase, excessive tiredness (69.4%), desire to escape (58.3%) and anxiety (44.4%),6 it was observed that the FiveW formula can act positively on these states.
The study highlights the significant interaction between the variable having a close person infected with COVID-19 and the effects of the intervention observed in the scores of Burnout and Secondary Traumatic Stress. This suggests that the FiveW formula has the potential to alleviate the negative impact caused by catastrophic situations such as the pandemic.
The reduction in the Compassion Satisfaction scores was surprising, as positive feelings were expected to improve after the Bach flower essence therapy. The observed opposite effect could be attributed to the inherent mode of action of the remedy, which brought unconscious emotional issues to the surface. This process increased the residents' self-perception of reality, including the recognition of biopsychic exhaustion experienced in their profession, which was expected to provide satisfaction due to helping other people. This effect may be associated with one of the flowers, Clematis, which safely brings the individual back to the present reality, focusing on the situation so that decisions can be made.23
Compassion and satisfaction, as a source of strength, motivate work, despite the high levels of stress.24 Feelings of hope and optimism are therefore generated, which encourage nurses to continue in their role as caregivers and to face the negative aspects of their professional lives. However, empathetic care can lead to internalization of tensions and exhaustion of caring.25
Some variables affected the scores of some ProQOL-4 subscales, such as year and specialty of the residency, and having a close person infected with COVID-19. The better effect of the Bach flower therapy in first-year residents observed in Compassion Satisfaction and Burnout could be attributed to more time spent by second-year residents exposed to the strain of caring and the intense workload of the residency program. Empirically, it is recognized that the presence of residents in care practice supports the downsizing of nursing care providers, which has become even more compromised by the death, absenteeism or departure of professionals infected by COVID-19.
A literature review on the factors associated with Compassion Fatigue in healthcare providers revealed that dissatisfaction with the work sector, chosen profession, and specific job functions was more commonly observed in providers affected by Compassion Fatigue. This dissatisfaction was particularly high among those directly involved in patient care. Additionally, there was a positive correlation between the number of years worked in a hospital setting and the prevalence of Compassion Fatigue.26
Considering the differences in Compassion Satisfaction and Burnout among the specialties, it is assumed that the diversity of specialties in adult health exposes residents of this program to more stressful situations. A North American cross-sectional study found that nursing professionals who worked in mixed care units (intensive care patients and patients receiving surgical and cardiovascular care) presented lower Compassion Satisfaction than those who worked in only one care unit.27 There is a tendency for nurses who work in pediatric and obstetrics units to present greater job satisfaction.28
The Burnout subscale showed a difference in the scores obtained at the screening and at the beginning of the study, suggesting that its items are influenced by unforeseen elements that are difficult to measure, above all, because they are subjective and non-constant experiences. There was a residual effect of the intervention on Secondary Traumatic Stress and consequently on Compassionate Fatigue at the follow up.
Study limitations include the small sample of residents, which makes it impossible to generalize the findings and weakens the power of the test, and the difference in the number of residents by specialization program. The very context of a pandemic, which is unstable, causes particular emotional strain on healthcare providers and is incomparable to other socio-historical moments.
Despite this, this study contributes to broaden the reflection on how the quality of professional life of nursing residents can be affected by Compassion Satisfaction and Compassion Fatigue. Considering these reflections, it would be important to investigate a larger sample of residents outside the pandemic context, and to include non-resident nurses, to see whether the same phenomenon is reproduced.
Conclusión
The FiveW flower formula produced a significant reduction in Secondary Traumatic Stress scores, which is one of the components of professional quality of life scale. Accordingly, Bach flower essence therapy with FiveW contributes as a complementary strategy in managing the quality of professional life, alleviating the symptoms of stress related to trauma among nursing residents.
Conflict of interest declaration
The authors declare that there are no conflicts of interest of a personal, economic, inter-institutional or other nature
Referências blibliográficas
1 Alvim CCE, Souza MMT, Gama LN, Passos JP. Relationship between the work process and mental illness nursing staff. Rev Flu Exten Univ. 2017;7(1):12-16. Portuguese. Available from: http://editorauss.uss.br/index.php/RFEU/article/view/918 [ Links ]
2 Stamm BH. The Concise ProQOL Manual. 2nd ed. Pocatello, ID: ProQOL.org. 2010 Available from: https://www.proqol.org/uploads/ProQOL_Concise_2ndEd_12-2010.pdf [ Links ]
3 Jilou V, Duarte JMG, Gonçalves RHA, Vieira EE, Simões ALA. Fatigue due to compassion in health professionals and coping strategies: a scoping review. Rev Bras Enferm. 2021;74(5):e20190628. doi: /10.1590/0034-7167-2019-0628. [ Links ]
4 Brasil. Ministério da Educação. Resolução CNRMS n. 5, 7 novembro de 2014. Dispõe sobre a duração e a carga horária dos programas de Residência Multiprofissional em Saúde e de Residência em Área Profissional da Saúde e sobre a avaliação e a frequência dos profissionais da saúde residentes. Diário Oficial da União. Brasília; 10 nov 2014, n. 217, Seção I, p. 34. [ Links ]
5 Silva RMB, Moreira SNT. Stress and multiprofessional residence in health: understanding meanings in the training process. Rev Bras Educ Med. 2019;43(4):157-166. Portuguese. doi: 10.1590/1981-52712015v43n4RB20190031. [ Links ]
6 Rocha JS, Casarotto RA, Schmidtt ACB. Health and work of the multiprofissional residence. Rev Cienc Salud. 2018;16(3):447-62. doi: 10.12804/revistas.urosario.edu.co/revsalud/a.7265. [ Links ]
7 Menegatti MS, Rossaneis MA, Schneider P, Silva LGC, Costa RG, Haddad MCFL. Stress and coping strategies used by nursing interns. Rev Min Enferm. 2020; 24:e-1329. Portuguese. doi: 10.5935/1415-2762.20200066. [ Links ]
8 Gallasch C, Cunha M, Pereira L, Silva-Junior JS. Prevention related to the occupational expousore of the health professional workers in the COVID-19 scenario. Rev Enferm UERJ. 2020;28:e-49596. Portuguese. doi: 10.12957/reuerj.2020.49596. [ Links ]
9 Mo Y, Deng L, Zhang L, Lang Q, Liao C, Wang N, Qin M, Huang H. Work stress among Chinese nurses to support Wuhan for fighting against the COVID‐19 epidemic. J Nurs Manag. 2020;28(5):1002-1009. doi: 10.1111/jonm.13014. [ Links ]
10 Natividade PCS, Spagnol CA, Vieira A, Almeida GV, Pereira KD. Contributions of integrative and complementary and practices in health to the quality of life of workers. Braz J of Develop. 2021;7(8):78873-78889. Portuguese. doi: 10.34117/bjdv7n8-213. [ Links ]
11 Pancieri AP, Fusco SB, Ramos BIA, Braga EM. Meanings of flower therapy for anxiety in people with overweight or obesity. Rev Bras Enferm . 2018;71(5):2310-15. doi: 10.1590/0034-7167-2018-0044. [ Links ]
12 Brasil. Ministério da Saúde. Portaria n.º 971 de 3 maio 2006. Aprova a Política Nacional de Práticas Integrativas e Complementares (PNPIC) no Sistema Único de Saúde. Brasília: Diário Oficial da União , n 84, seção I, p. 20- 24, 4 maio 2006. [ Links ]
13 Bear J, Bellucco W. Florais de Bach: o livro das fórmulas. São Paulo: Pensamento; 2019. [ Links ]
14 Foletti A, Ledda M, Piccirillo S, Grimaldi S, Lisi A. Electromagnetic information delivery as a new tool in translational medicine. Int J Clin Exp Med 2014;7(9):2550-2556. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4211758/pdf/ijcem0007-2550.pdf [ Links ]
15 Guerrini IA, DomeneTG. Como as conexões quânticas auxiliam na busca da saúde integral: as bases científicas da terapia floral e de outras terapias sutis. Curitiba: Appris; 2020. [ Links ]
16 Halberstein R, Sirkin A, Fajardo V P, Vaz MO. Healing With Bach® Flower Essences: testing a complementary therapy. Complement Health Pract Rev. 2007;12(1):3-14. doi: 10.1177/1533210107300705. [ Links ]
17 Krämer D. Nuove terapie com i Fiori di Bach. 3ªed. Roma: Ed. Mediterranee; 2008. p.99-100. [ Links ]
18 Lago K, Codo W. Compassion fatigue: evidence of internal consistency and factorial validity in ProQoL-BR. Estud Psicol. 2013;18(2):213-21. Portuguese. doi:10.1590/S1413-294X2013000200006. [ Links ]
19 Xie W, Chen L, Feng F, Okoli CTC, Tang P, Zeng L, Jin M, Zhang Y, Wang J. The prevalence of compassion satisfaction and compassion fatigue among nurses: a systematic review and meta-analysis. Int J Nurs Stud. 2021;120:103973. doi: 10.1016/j.ijnurstu. 2021.103973. [ Links ]
20 Cao X, Li J, Gong S. The relationships of both transition shock, empathy, resilience and coping strategies with professional quality of life in newly graduated nurses. BMC Nurs. 2021;20(1):65. doi: 10.1186/s12912-021-00589-0. [ Links ]
21 Lee MS, Shin S, Hong E. Factors affecting secondary traumatic stress of nurses caring for COVID-19 patients in South Korea. Environ Res Public Health. 2021;18(13):6843. doi: 10.3390/ijerph18136843. [ Links ]
22 Chesak SS, Horin KH, Cutshall SM, Jenkins SM, Sood A. Feasibility and efficacy of integrating resiliency training into a pilot nurse. Nurse Educ Pract. 2021; 50:102959. doi: 10.1016/j.nepr.2020.102959. [ Links ]
23 Barnard J. Forma e função. 1a ed. São Paulo. Editora Blossom; 2018. [ Links ]
24 Lee HJ, Lee M, Jang SJ. Compassion satisfaction, secondary traumatic stress, and burnout among nurses working in trauma centers: a cross-sectional study. Int JEnviron Res Public Health . 2021;18(14):7228. doi: 10.3390/ijerph18147228. [ Links ]
25 Pehlivan T, Güner P. Compassion fatigue: the known, unknown. J Psychiatric Nurs. 2018;9(2):129-34. doi: 10.14744/ phd.2017.25582. [ Links ]
26 [ Links ]
27 Sacco TL, Ciurzynski SM, Harvey ME, Ingersoll GL. Compassion satisfaction and compassion fatigue among critical care nurses. Crit Care Nurse. 2015;35(4):32-43. doi: 10.4037/ccn2015392. [ Links ]
28 Kagan I, Hendel T, Savitsky B. Personal initiative and work environment as predictors of job satisfaction among nurses: cross-sectional study. BMC Nurs . 2021;20(1):87. doi: 10.1186/s12912-021-00615-1. [ Links ]
Received: January 31, 2022; Accepted: March 13, 2023
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
