











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkBackground
In recent months, humanity has faced a new challenge: COVID-19 - "Coronavirus Disease - 2019", caused by SARS-CoV-2, a new type of coronavirus. The disease spread and received pandemic status in March 2020, with a significant impact on public health and the economy (1). Coronaviruses belong to a large viral family and for decades have been known to cause respiratory infections in humans and animals. In December 2019, a new coronavirus was identified as causing a flu type syndrome and severe pulmonary complications, the illness caused was named COVID-19 (2). The origin, which is still uncertain, of SARS-CoV-2 dates to Wuhan, China, where the first cases were identified. The contamination took place in geometric progression to nearby provinces, and later expanding to countries on several continents (1,2,3).
In cities and large centers, moderate to severe social isolation was one of the strategies adopted to face the pandemic. While some classify this strategy as a fundamental priority for disease control (1,4), others question its applicability and results in practice (5,6,7).
In any case, in health units allocated for those affected by COVID-19, the challenge faced by professionals and university students in the health area has been great. Most intensive care units (ICU) or care centers needed to organize and expand patient care; adopt new personal protective equipment (masks and aprons); deal with uncertainties and stresses of care demands; and, frequently, face a lack of appropriate training and/or logistical and structural negligence of all kinds. In addition, health professionals make up the group most vulnerable to contamination and, consequently, the possibility of being subjected to social isolation as a protective measure, which has a great impact on the emotional health of this professional (8,9).
The WHO statement was followed by individual and research center statements about projections of hospitalizations and deaths, as well as potential coping strategies against COVID-19(10,11). Heated debates about the use of personal protective equipment such as masks and face shields; mandatory social isolation or "lockdowns" to contain the peak of contamination; viable medications for treatment, whether early or late; among other related topics, have engrossed the international scientific debate (5,6,7). In the health sector, the partially unknown behavior of the virus; risk of contamination; need to reallocate resources to the front line of the new disease; inefficiency and ineffectiveness of the Health System; and corruption and inefficiency in the use of resources available, have brought serious consequences (7).
In this unfavorable and unhealthy scenario, health professionals have been under immense pressure, facing safety challenges, the need to limit the spread of the coronavirus, reduce morbidity and mortality, and combat the delay in diagnosis and treatment of patients with other diseases (12,13). Thus, in some locations, the emergence of COVID-19 seems to have caused elective surgeries and surgical procedures to be canceled indefinitely, as well as numerous complementary exams of a preventive nature. The cancellation of these procedures, associated with the fear of contamination and illness when seeking medical care at health facilities, may be responsible for the increase in diagnoses of advanced neoplastic diseases (14), as well as complicated inflammatory diseases, due to postponement of the search for adequate medical care. Some surveys carried out in European countries corroborate the impression shared by doctors, who are living this reality (15,16,17,18).
In this context, obtaining information about social behavior, such as the use of violence in relationships, as well as the occurrence of car trauma and falls, becomes strategic to direct efforts to dealing with the consequences arising from trauma, providing adequate means and treatment strategies, in addition to making teams more aware and empowered to manage their patients. Death rates from violent causes in the main Brazilian urban centers are among the highest on the American continent, expressing a growing trend, which since the 1980s has been increasing (19). Violence indicates strength and refers to the notions of constraint and the use of physical superiority over another.
The health sector's vision on the topic of violence includes explanatory and operational aspects. Among national and international institutions, there seems to be a consensus around the following issue: violence represents a risk for the realization of the human vital process; life-threatening; alters health; produces illness; and causes death as a reality or near possibility (19). The third aspect advocates the conception of the social sphere as the dominant environment in the production of violence. However, in different sociological and health texts, criticisms are made of the excessive emphasis on the conception of biological determination of violent behavior (20).
Questioning the view that privileges the biological causality of violence, as well as the stance of a single-cause, macro or micro-social understanding, is based on the concept of violence as a complex, multi-causal phenomenon involved in the cause-effect dialectic. There is also the need to make the manifestations of violence and its articulation specific, and the indication that subjective processes must be, at the same time, included in the analysis and contextualized in the socio-historical context (20). Therefore, responding to the growing demand for care services for traumatic injuries caused by accidents and violence also requires new skills, equipment, and organization of the health system. The complexity of these challenges requires adequate reflections, decisions, and actions (18,20). Thus, the relationship between violence and urgent and emergency pre-hospital care is presented as a public health policy strategy. However, the approach of pre-hospital care for victims of violence or in violent areas, from the perspective of professionals who help them, is not a frequent approach in research (21).
Another important aspect in addition to violence in trauma is falls. A fall is an accidental event that results in a change in the individual's position to a lower level, in relation to their initial position, with an inability to correct it in a timely manner and coming to rest inadvertently on the ground (22). For a fall to occur, there must be a disturbance in balance and a failure of the postural control system to compensate for this disturbance, with 56% falling from a height, where the public road was the most frequent place of occurrence (23). The stability of the body depends on the adequate reception of information through sensory, cognitive, central nervous system, and musculoskeletal components in an integrated way (24). Falls are classified as accidental events, which, together with car collisions, interpersonal and self-inflicted violence, comprise a group of causes of mortality and morbidity (25).
Falls were the most frequent accidents among patients who participated in the 2009 Viva Survey, representing 37% of all accidental events that led people to seek care in urgent and emergency services(20). Males suffer most falls in the population up to 49 years of age, and females are the main victims in the over 50 age group (21). Given this context, the aim of this study was to assess the clinical and epidemiological characteristics of trauma related to violence, accidents, and falls among the years 2019, 2020, and 2021, considered before and during the COVID-19 pandemic. The hypothesis of this study was that the occurrence of trauma and health care increased during the COVID-19 pandemic period.
Methods
Design, setting, participants and ethics
The present research is an analytical study of the retrospective cohort type. First, the search was performed in the TABNET system, which establishes digital health indicators from the Municipal Health Department (SMS) of the State of São Paulo. Within this system, a search was carried out for the Information System for the Surveillance of Accidents - SIVA, of the Coordination of Health Surveillance - COVISA/SMS, in which situations of violence were notified and recorded by the National Information System for Diseases of Notification - SINAN Net. After that, the Information System for the Surveillance of Violence and Accidents (Tabnet SIVVA) was accessed, with a focus on notifications and recording of situations of falls and other accidents.
All searches for violence, falls, and other accidents were raised by the systems: SIVA and SINAN, in the periods from March to July, in 2019, considered pre-pandemic; and the years 2020 and 2021, considered during the COVID-19 pandemic. The standardized age group for the searches were adults aged 25-55 years who suffered urgent trauma from violence, falls, and other accidents.
Trauma Variables assessed in Violence, Falls, and Other Accidents
First, the topics researched related to violence were in relation to the types of violence (physical, torture, psychological/moral, and sexual); mechanism of violence (body strength/beating, hanging, blunt object, sharp object, and suspected alcohol use); cause of violence (father, mother, stepfather, spouse, boyfriend, son, siblings, friends/acquaintances, and strangers), and health care. In relation to falls and other accidents, the cases of notification for falls, drowning, electric shock, burns, accidents caused by weapons - melee weapon or firearm, heat or fire, suffocation, landslide, or flooding were raised as well as traffic accidents. Another point raised was in relation to health care in cases of falls and traffic accidents in hospitals, clinics, and emergency rooms.
Data collection was also related to the socio-demographic characteristics of adults, aged 25-55 years, who suffered trauma related to violence, falls, and other accidents, in the period before and during the COVID-19 pandemic, in the city of São Paulo.
Statistical analysis
Non-parametric tests were applied for statistical analysis, considering the nature of the studied variables. The Chi-Square Test was applied to compare the years 2019, 2020, and 2021, in relation to confirmed cases of violence, falls, and other accidents in the city of São Paulo. The same test was applied to compare the three years in relation to the frequencies of each of the types of trauma studied.
Results
Table 1 shows that trauma in adults was more prevalent in males, with complete primary education, and predominating ethnicity between white and brown.
Table 1 Socio-demographic characteristics of adults aged 25-55 years who suffered trauma-related violence in the period. before and during the COVID-19 pandemic. in São Paulo.
| Sociodemographic Variables | 2019 number (%) | 2020 number (%) | 2021 number (%) | Total |
|---|---|---|---|---|
| Complete primary education | 1.737 (42.7) | 1.658 (40.7) | 666 (16.4) | 4.061 |
| Complete high school | 5.052 (44.3) | 4.482 (39.3) | 1.856 (16.3) | 11.390 |
| Complete higher education | 760 (45.8) | 640 (38.6) | 257 (15.5) | 1.657 |
| Illiterate | 162 (45.6) | 128 (36.0) | 65 (18.3) | 355 |
| Female sex | 16.873 (46.9) | 13.424 (37.3) | 5.656 (15.7) | 35.953 |
| Male sex | 13.477 (46.8) | 10.922 (37.9) | 4.384 (15.2) | 28.783 |
| White | 11.568 (48.2) | 8.797 (36.6) | 3.617 (15.0) | 23.982 |
| Black | 2.948 (43.0) | 2.735 (39.9) | 1.162 (16.9) | 6.845 |
| Yellow | 167 (40.9) | 180 (44.1) | 61 (14.9) | 408 |
| Brown | 10.802 (42.9) | 10.091 (40.1) | 4.249 (16.9) | 25.142 |
| Indigenous | 127 (44.5) | 114 (40.0) | 44 (15.4) | 285 |
In table 2 it can be observed that adults who suffered different types of violence: physical, torture, and sexual had a higher percentage prevalence in the year 2019, the pre-pandemic period of COVID-19, when compared to the years 2020 and 2021, considered pandemic years, except for psychological/moral violence, which was higher in 2021 when compared to 2019 and 2020. The observed findings reflect that the pandemic period possibly resulted in the masking of surveillance records on violence, given the social isolation guidelines advocated between 2020 and 2021, a fact that may have led participants not to register notifications of violence with the same frequency as in the year 2019.
Table 2 Types of violence in confirmed cases of adults. aged 25-55 years. who suffered trauma from March to July. before and during the COVID-19 pandemic in São Paulo.
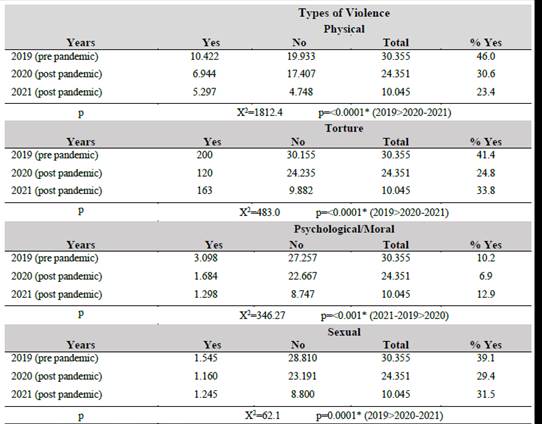
* Chi-square test. considering statistical differences p<0.05
Table 3 shows that the prevalence of different mechanisms of violence was significantly higher in the year 2019, the pre-pandemic period of COVID-19, when compared to the years 2020 and 2021, considered years of experience of the pandemic.
Table 3 Mechanisms of Violence in confirmed cases of adults. aged 25-55 years. who suffered trauma from March to July, considered before and during the COVID-19 pandemic in the city of São Paulo.
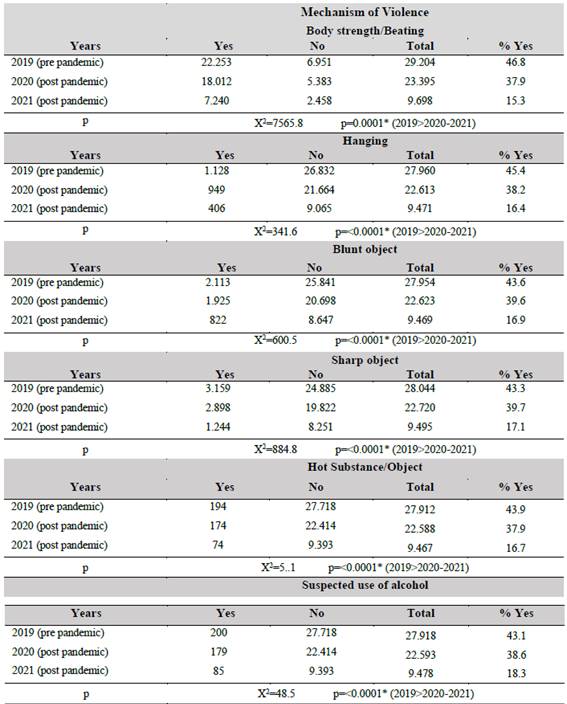
* Chi-square test. considering statistical differences p<0.05
Table 4 shows that the prevalence of the different causes of violence were significantly higher in the year 2019, the pre-pandemic period of COVID-19, when compared to the years 2020 and 2021, considered years of experience of the pandemic.
Table 4 Cause of Violence in confirmed cases of adults, aged 25-55 years, who suffered trauma from March to July, before and during the COVID-19 pandemic, in São Paulo.
| Causer of Violence | Years before and during the COVID-19 pandemic | |||||
|---|---|---|---|---|---|---|
| 2019 N % | 2020 N % | 2021 N % | X2 | p* | Differences | |
| Father | 1643 60.3 | 755 27.7 | 327 12.0 | 992.1 | <0.0001 | 2019>2020/2021 |
| Mother | 1427 57.1 | 734 29.4 | 338 13.5 | 729.5 | <0.0001 | 2019>2020/2021 |
| Stepfather | 394 46.6 | 301 35.6 | 150 17.8 | 107.7 | <0.0001 | 2019>2020/2021 |
| Spouse | 4738 44.3 | 4287 40.1 | 1665 15.6 | 1545.5 | <0.0001 | 2019>2020/2021 |
| Boyfriend | 818 41.9 | 808 41.4 | 327 16.7 | 242.0 | <0.0001 | 2019>2020/2021 |
| Son | 843 42.3 | 774 38.9 | 375 18.8 | 192.3 | <0.0001 | 2019>2020/2021 |
| Brother | 1254 45.5 | 1050 38.1 | 454 16.5 | 375.9 | <0.0001 | 2019>2020/2021 |
| Friend/Acquaintance | 3591 49.6 | 2629 36.3 | 1027 14.2 | 1389.0 | <0.0001 | 2019>2020/2021 |
| Stranger | 6688 46.2 | 5585 38.6 | 2209 15.3 | 4484.6 | <0.0001 | 2019>2020/2021 |
* Chi-square test, considering statistical differences p<0.05
Table 5 shows that the prevalence of health care in cases of violence was significantly higher during the pandemic period between 2020 and 2021 when compared to 2019, considered pre-pandemic of COVID-19.
Table 5 Health care for confirmed cases of violence in adults, aged 25-55 years, who suffered trauma from March to July, before and during the COVID-19 pandemic, in the city of São Paulo.
| Health Care in Cases of Violence (Health Network) | ||||
|---|---|---|---|---|
| Years | Yes No | Total | % Yes | |
| 2019 (pre pandemic) 2020 (post pandemic) 2021 (post pandemic) | 16.395 15.378 6.559 | 11.566 7.543 2.996 | 27.961 22.921 9.555 | 58.6 67.1 68.6 |
| p | X2=520.95 p=<0.0001 (2020-2021>2019) | |||
* Chi-square test, considering statistical differences p<0.05
Table 6 shows that the prevalence of traffic accident trauma to pedestrians, occupants, drivers, and passengers were significantly higher in the pre-pandemic year 2019 and the year during the pandemic 2020 when compared to the year 2021.
Table 6 Confirmed cases of trauma from traffic accidents in adults, aged 25-55 years, from March to July, before and during the COVID-19 pandemic, in the city of São Paulo.
| Traffic Accident Trauma | ||||
| Years | Pedestrian | Occupant | Driver | Passenger |
| N (%) | N (%) | N (%) | N (%) | |
| 2019 (pre pandemic) | 2.341 (42.8) 1.903 (40.1) 820 (17.1) | 7.671 (52.3) 8.767 (34.1) 3.597 (13.6) | 3.718 (46.3) 5.196 (37.9) 2.051 (15.8) | 904 (42.1) 884 (41.2) 358 (16.7) |
| 2020 (post pandemic) | ||||
| 2021 (post pandemic) | ||||
| P | X2=4579.9 | X2=4990.0 | X2=8981.8 | X2=286.0 |
| (2019 and 2020 > 2021) | p<0.0001* | p<0.0001* | p<0.0001* | p<0.0001* |
* Chi-square test, considering statistical differences p<0.05.
The figures showed that the prevalence of the cases of trauma from fall, drowning electric chock and burn (figure 1), as well as white gun, fire arm, suffocation, landslide/ flood (Figure 2), were significantly higher in the pre-pandemic year 2019 when compared to 2020 and 2021. The figure 3 and 4 showed the prevalence health care (hospital/emergency room or ambulatory) for confirmed cases of traffic accidents and cases of falls and other accidents, in which majority remained high in the year 2021 when compared to the years 2019 and 2020.
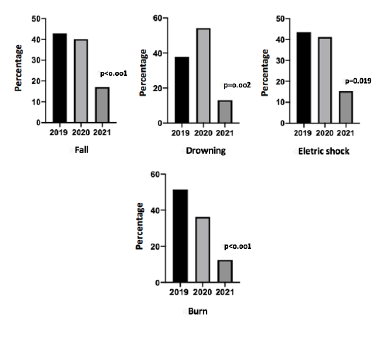
Figure 1 Prevalence of confirmed cases of trauma from falls and other accidents in adults, aged 25-55 years, between March and July, before and during the COVID-19 pandemic, in the city of São Paulo.
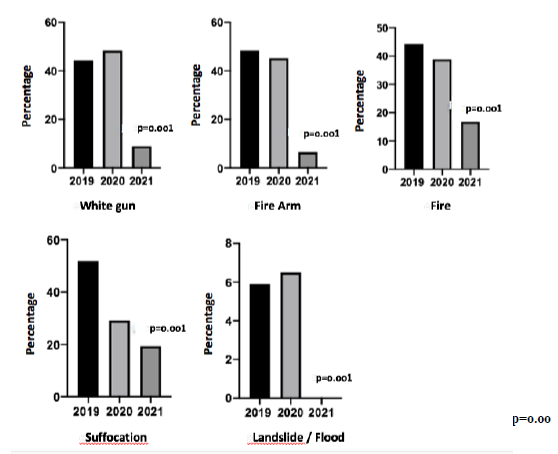
Figure 2 Prevalence of confirmed cases of trauma from other accidents in adults, aged 25-55 years, from March to July, before and during the COVID-19 pandemic, in the city of São Paulo.
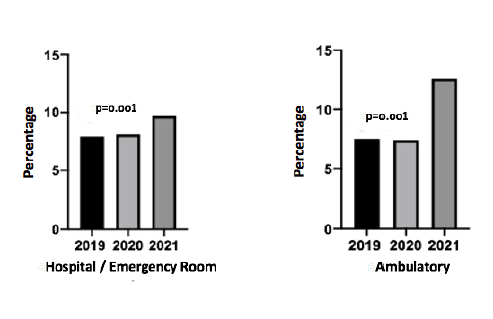
Figure 3: Health care for confirmed cases of traffic accidents in adults, aged 25-55 years, who suffered emergency trauma from March to July, before and during the COVID-19 pandemic, in the city of São Paulo.

Discussion
The present study aimed to verify the clinical and epidemiological characteristics of trauma related to violence, accidents, and falls among the years 2019, 2020, and 2021, considering before and during the COVID-19 pandemic. The main results showed that trauma, in the period before and during the pandemic, was more prevalent in males with elementary school education and white and/or brown ethnicities among the adults evaluated. When analyzing the different types of violence: physical, torture, and sexual, there were higher percentage prevalence during 2019, the pre-pandemic period of COVID-19, except for psychological/moral violence, which was higher in 2021. It was also observed that the different mechanisms of violence were significantly more prevalent in 2019, as well as the different causes of violence, falls, and car trauma involving pedestrians, occupants, drivers, and passengers. Outpatient care confirmed the trend of superiority in the pre-pandemic period, however emergency hospital care showed a greater number of requests in 2020 and 2021.
The literature demonstrates that the predominance of males is common in traumatic injuries (26), however, with a wide range and diversity of municipalities, regions, and places of health care, a fact that hinders any possible comparisons between the scientific findings. Although trauma is seen and recognized as a global health problem, which has almost unrestricted economic consequences, many trauma control and response centers are still not centralized. By not having enough broad and comprehensive information that can guide government interventions and programs focused on reducing mortality, in addition to the situation perpetuating itself and the effectiveness of combating trauma remaining low (27), drawing parallels between socio-epidemiological profiles becomes challenging and sometimes unfeasible.
Another important point is the increased level of violence: physical, torture, and sexual, during 2019, the pre-pandemic period of COVID-19, when compared to the period during the pandemic (2020 and 2021), except for psychological/moral violence, which was higher in 2021. According to Praça et al., (2017)26, quality and adequate trauma care is essential, providing in-depth knowledge of the clinical profile of the assisted population, as well as the alignment between these characteristics and local public policies for better availability of clinical care for violence: physical, torture, and sexual. Among the possibilities for the occurrence of sexual violence, there is Intimate Partner Violence (IPV), in which young people are associated with a greater risk of suffering aggression, while older individuals are more associated with promoting aggression against partners. Some of the explanations for IPV are: unemployment, low levels of education, and low socioeconomic status, as well as feelings and emotions (anxiety, depression, post-traumatic stress, and personality disorders), and alcohol abuse (28). In the current study, notifications of violence, physical, torture, and sexual, were reduced during the pandemic compared to the previous year. Although COVID-19 brings new strategies and changes to daily routines, which can result in interpersonal conflicts of physical and sexual violence, this fact may have been underreported by victims during the pandemic. In line with the data found in the current study, a survey carried out in a rural area showed that the number of visits to emergency care units also decreased during the period analyzed under the influence of COVID-19, demonstrating increased notifications of penetrating injuries, affecting men and other members of their closest social support group (29).
Among the different mechanisms of violence observed in this study, the main causes were falls, car trauma involving pedestrians, occupants, drivers, and passengers, with greater significance for 2019 compared to 2020 and 2021. Scientific evidence reveals that an analysis of data referring to trauma and its causes in different systems and regions, without integration, will not lead to a global description compatible with the reality of the facts. Specifically, in the country of China, there was an increase in the number of traumas related to car accidents, explained by the intensification of industrialization and expansion of the road network; another example was South Africa, which reported an increased frequency of trauma caused by accidents and collisions involving public transport vehicles, which resulted in the loss of many lives, simultaneously (26). The differential of this study was to understand these etiological mechanisms of trauma in Brazil, and in a sample of young adults, which is little explored in scientific evidence, a point that makes comparisons with other studies difficult for a better causal approach to traumas. A study revealed that traffic accidents or car collisions are among the sixth leading cause of death in 195 countries (27), with traumatic injuries being the most frequent, followed by homicides and attempted homicides (26).
When analyzing the mechanisms of violence used for the genesis of traumatic injuries, among which we consider: (1) use of physical force and/or beating, (2) hanging, (3) use of a blunt object, (4) use of a sharp object, (5) use of a substance and/or hot object, and, finally, (6) use of concomitant alcoholic beverages; we found a higher prevalence of all mechanisms studied in the period analyzed in 2019. This same trend was found when we analyzed the numbers considering trauma related to falls. We found a higher prevalence in the period 2019, compared to the analyzed intervals in 2020 and 2021. This trend was also followed by data related to electric shocks and burns, except for the numbers related to drowning, which had the highest record in the 2020 period.
We suggest two possible explanations for the results found. The first is the possibility of underreporting trauma-related data during the pandemic period, especially in the early months and months in which the number of cases presented records of the historical series registered to date. Due to the changes made to the structure of the health units and the health system to attend infected individuals, we believe that many of the cases may have been neglected by the system, and not adequately attended to or consequently, not notified. The second refers to behavioral changes generated by fear. This feeling is believed to have played an important role during the current pandemic. Its action and influence may have reached different spheres, influencing collective and individual behavior. Through its function of helping human beings to adapt, throughout history, fear acts on the nervous system in two different ways; either instinctively and subconsciously, almost automatically, through the action of the cerebral tonsils, or in a lucid and conscious way, using the neocortex (30). Fear, in view of the collective challenges faced with infections, hospitalizations, and deaths generated by SARS-CoV-2, may have generated the results found in the studied population.
The analysis of trauma caused by car collisions showed a higher prevalence in pedestrians and passengers during the period analyzed in 2019; while there was greater involvement of occupants and drivers in the 2020 period. Unlike other possibilities of natural disasters, pandemics affect the world's economy and population by modifying health and claiming lives. Even though it did not destroy the infrastructure of the affected areas, the pandemic generated government reactions aimed at preventing the dissemination of the coronavirus. In this line of thought, many government officials instituted quarantine periods, enacted decrees closing schools, commercial establishments, and public spaces, as well as establishing social distance. Despite the effectiveness of each of the established actions, these measures generated a decrease in the circulation of cars on lanes and highways, changing the dynamics of traffic, among which we can cite the reduction in congestion and traffic density during the pandemic. However, flow and speed are inversely proportional characteristics in the dynamics of car traffic (31). Therefore, changes in the prevalence of accidents involving cars, their drivers, occupants, and pedestrians may be related to these differences caused by the change in traffic.
When we consider "traumas from other accidents", which include traumas caused by firearms, melee weapons, heat, fire, suffocation, landslides, or floods, we identified a clear prevalence in the period analyzed in 2019. Once again, the hypothesis of underreporting is raised, considering that the described trend is an increase in the frequency and severity of domestic violence events. Concomitantly, due to difficulties in requesting help from third parties during the pandemic, it is also expected that the numbers related to aggression are higher than reported and the association with substance abuse may also increase and be associated with violent events during the pandemic (29,32).
Another important finding observed in this study was increased outpatient care in the pre-pandemic period, while the number of requests for emergency hospital care was shown to increase in the period between 2020 and 2021. Also in this rationale, it was found that for the use of health services - outpatient, hospital, and emergency room, there was a higher prevalence in the year 2020 when analyzing trauma from car collisions. As for traumas related to falls, drowning, electric shocks, and burns, the use of outpatient health services had a higher prevalence during the period in 2019, while hospital care and the use of emergency room care were higher in the period analyzed in 2021. Both results found for the types and characteristics of trauma described above are in line with the data found in the literature, which advocate for an immediate increase in consultations in emergency rooms and hospital units during outbreaks or explosions of cases related to the coronavirus, while a reduction in clinical and surgical outpatient services is expected during the pandemic (33). According to Praça et al., (2017), for hospital care in emergency rooms to provide effective and pragmatic assistance, a single integrated information system is needed so that, in fact, there are effective actions, programs, and services (26).
Conclusions
The prevalence of emergency trauma directed to violence, accidents, and falls remained higher in the period in 2019, considered pre-pandemic of COVID-19, compared to the years 2020 and 2021, considered during the pandemic, as well as the demand for health care in hospitals (emergency department) and outpatient clinics. These findings demonstrated a reduction in cases of notifications and demand for health care for adults affected by the trauma of violence, accidents, and falls during the COVID-19 pandemic.
DECLARATIONS
Consent for publication
Not Applicable
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author (apribeiro@alumni.usp.br) on reasonable request.
Competing interests
All Authors declare that they have no conflict of interest.
Funding
This study did not receive grants from funding agencies.
Authors’ contributions
All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors approved the final version to be published. Study conception, writing and design: PCRF and APR. Acquisition of data and Statistics: PCRF, EJL, APR, DFAG, CNF, LNN, LDMF, ISL, YJ and NFN. Analysis and interpretation of data: PCRF, EJL, YJ, APR and NFN.

