










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.63 n.2 San José Apr./Jun. 2021
Original
Prevalence of sarcopenia in the elderly adult population in Costa Rica
1Hospital Nacional de Geriatría y Gerontología, Departamento de Geriatría y Soporte Nutricional y Unidad de Investigación. San José, Costa Rica.
2Hospital Nacional de Geriatría y Gerontología, Departamento de Atención Comunitaria y Unidad de Investigación. San José, Costa Rica
In 1989, Irwin Rosenberg used the term “sarcopenia” (from the Greek sarx: flesh and penia or loss), to describe the decline in muscle mass related to aging. 1 His definition has been expanded in the last 20 years, referring to sarcopenia as the decrease in muscle mass and strength, with repercussions on functional performance, resulting in adverse consequences such as functional impairment, falls, hospitalizations, and poor quality of life and increased mortality.2-5
Its prevalence varies in the different reviews carried out, due to the different measurement methods.6-10 The European Working Group for the Study of Sarcopenia (EWGSOP)11 established the diagnostic criteria for defining sarcopenia, which has made it possible to homogenize the findings of its prevalence.
Cooker and Wolf (2012)3 noted the presence of sarcopenia among people aged 60-70 years in the community at 5-13% and up to 68% in the institutionalized population. In the Health Aging and Body Composition Study, the prevalence of sarcopenia in the community was 14% to 18%,10 while other authors in the same setting have documented it in up to 29% of the population.11
In Mexico, with the EWGSOP criteria, elderly adults with sarcopenia were identified in 33.6%, being more prevalent in those over 80 years of age (50.4%),12 this prevalence has been reported to be lower when standardized measures are used for the Mexican population, being 11.07%.13
Sarcopenia is a multifactorial process, among its main etiologies are the chronic low-grade inflammatory state that characterizes aging, low dietary protein intake, sedentary lifestyle, hormonal changes such as testosterone depletion, vitamin D deficiency, and insulin resistance, and chronic decompensated diseases. 7,14
Due to the adverse effects of sarcopenia and the variability of data regarding its prevalence, information from Costa Rica: Study of Longevity and Healthy Aging (CRELES) was used to determine the prevalence of sarcopenia using the EWGSOP2 criteria, as well as the associated factors in the Costa Rican elderly adult population.
Methods
Design
Based on the CRELES study (Costa Rica: Study of Longevity and Healthy Aging), and using the public databases available on the web page of the Central American Population Center of the University of Costa Rica, the analysis were carried out using the cohort of elderly adults aged 60 years or more.
The development objective of CRELES is explained in other publications. 15,16 CRELES is a longitudinal study with three rounds of study, the first in 2005, then in 2007, and finally in 2009.
For this study, we used data from the first round of interviews, conducted from November 2004 to September 2006, based on a representative sample of about 3000 adults born in 1945 or earlier and residing in Costa Rica in the year 2000.
Population
For this analysis, and after eliminating subjects with missing data on the variables to be studied, the final sample was 2516 people aged 60 and over.
Variables
Sociodemographic variables such as age, sex, economic income, level of education, cohabitation, self-perception of health, reported physical activity, reported comorbidities, anthropometric variables, muscle strength and physical performance tests such as the 5 times timed stand-up and sit-down test and walking speed were included, this was measured over a distance of 3 meters.
To define sarcopenia, the criteria of the European Working Group for the Study of Sarcopenia 2 (EWGSOP) were used together with the cut-off points of the Sarcopenia Project of the Foundation for the National Institutes of Health (FNIH):
Low muscle mass. In the absence of body composition methods, calf circumference (WC) was used. A value of less than 31 cm was considered as low muscle mass for both sexes.
Low Muscle strength. Muscle strength was obtained through grip strength, with a Jamar hydraulic dynamometer ©. The maximum measurement in kg obtained with the dominant limb was used. For this study, the cut-off points were adjusted according to gender.
Therefore, sarcopenic were defined as persons with a PC below 31 cm with muscle strength of <27 kg in men and <16 kg in women; those who did not meet this condition were classified as non-sarcopenic.
Statistical analysis
After the sarcopenia variable was constructed, descriptive statistics were performed. For these descriptive analyses, two-dimensional tables were elaborated in which the percentage of sarcopenic and non-sarcopenic were calculated. The different sociodemographics and other health variables
were determined according to the category, as judged by the expert. Then, logistic regression was conducted, considering in this case sarcopenia as the dependent variable, which has two possible categories, sarcopenic and non-sarcopenic. As independent variables of the model, a large number of previously described variables were used, because the objective, in this case, the nature of the analysis was exploratory. For this case, only variables that provide problems to the model were excluded, for example, the case of multicollinearity, missing data and others that caused the estimated odds ratios not to converge adequately. Once all the problems presented by the model were fixed and given adequate revision, odds ratios for the sarcopenic category were obtained as results, because the non-sarcopenic category was taken as a reference since it is considered to be the healthy one. Now, to contrast, the relevance and possible error in the estimation of the odds ratio, a 95% confidence interval was estimated. All the analysis was carried out using the SPSS v16 program.
Results
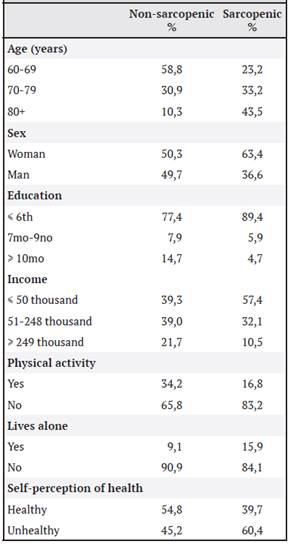
A total of 2516 persons aged 60 years and elderly were included. When the sarcopenia criterion was applied, a prevalence of sarcopenia was identified in 10.26% of the persons studied. As age increased, the cases of sarcopenia were higher, being 33.2% in the age range 70-79 years and 43.5% in those over 80 years of age. In the sex variable, women had more sarcopenia than men with 63.4% and 36.6% respectively.
People with sarcopenia had lower economic income (57.4% with an income of fewer than 50 thousand colones per month), and 90% had a level of schooling lower than the sixth year of primary school. Only 16% lived alone. The self-perception of health was evaluated, documenting that 60.4% of the people with sarcopenia perceived themselves as unhealthy. Of those studied, 83.2% denied doing any type of physical activity, as can be seen in Table 1.
Among the antecedents reported by people with sarcopenia, history of falls (59%), pulmonary iseases (23%), arthritis (20.7%), osteoporosis (11.8%), cerebrovascular disease (CVD) (8.3%), cancer (7.6%) and myocardial infarction (5.6%) were frequently found. Smoking was similar between sarcopenic and non-sarcopenic 40.8% and 44.1% respectively.
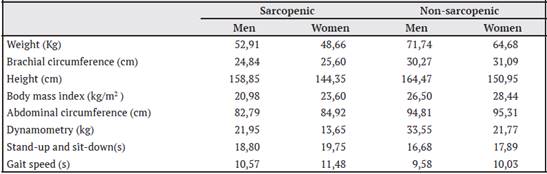
Anthropometric and functional variables were analyzed by sex and sarcopenic status (Table 2). Nonsarcopenic men had a higher average weight than sarcopenic men (71.7 kg vs 52.91 kg), the same was true for women (64.68 kg vs 48.66 kg respectively). This phenomenon was also observed with brachial circumference and abdominal circumference. On average, body mass index was lower in both men and women with sarcopenia (20.98 kg/m2 and 23.60 kg/m2 respectively), while the average CP was 28.4 cm for people with sarcopenia and 34.9 cm in the group without sarcopenia.
Grip strength was greater in people without sarcopenia than in sarcopenic people; in the latter, men had an average dynamometry of 21.95 kg and women of 13.65 kg. In the gait speed and the standup and sit-down test, people with sarcopenia took longer for their execution (Table 2).
Table 2 Average anthropometric and functional variables of the individuals in the CRELES study, cohort 2005
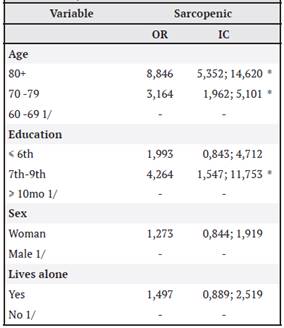
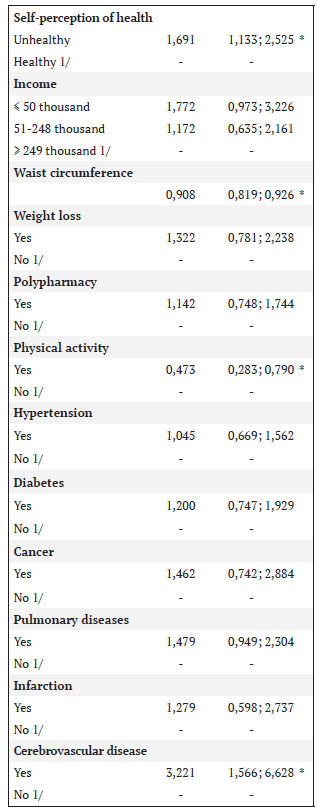
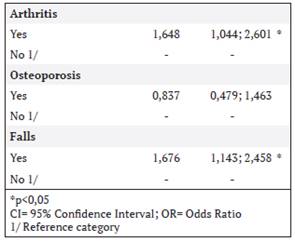
In the risk ratio (OR), taking sarcopenia as the dependent variable, the variables that showed the greatest association were age, with the risk increasing after 70 years of age (OR 3.164; CI 1.962-5.101), being even greater after 80 years of age (OR 8.846; CI 5.352-14.620), level of education (OR 4.264; CI 1.547-11.753), and perceiving oneself as unhealthy (OR 1.691; CI 1.133-2.525). Of the comorbidities, having a history of CVD (OR 3.221; CI 1.566-6.628), arthritis (OR 1.648; CI 1.044-2.601), falls (OR 1.676; CI 1.143-2.458) and being physically active (OR 0.473; CI 0.283-0.790). Among the anthropometric variables, waist circumference was the only one with an association (OR 0.908; CI 0.819-0.926) (Table 3).
Discussion
To our knowledge, this is the first study to show national data on the prevalence of sarcopenia in people in the community. The EWGSOP developed a clinical definition and diagnostic criteria with cut-off points that make it easy to apply6 and to analyze the prevalence of this geriatric syndrome in our country.
In CRELES, calf circumference was used as an indirect measure of muscle mass, which has studies correlating it with skeletal muscle mass index, disability, and self-reported physical perception.20,21 Calf circumference is currently considered a sensitive, inexpensive, non-invasive, and easy-tomeasure anthropometric measure.22,23 The cut-off point of 31 cm has been suggested as an indicator of decreased muscle mass. 20,22
In Mexico, applying the EWGSOP criteria (with PC as a measure of muscle mass), the prevalence of sarcopenia was higher (33.6%)12 than in our study (10.26%). In a more recent study in that same country, Perez et al (2016) had a prevalence of sarcopenia at 11.07%, similar to that documented in Colombia with 11.5%,17 values close to that documented in Costa Rica. As described by Arango et al (2012), in Costa Rica it was more prevalent in women and in those over 80 years, which exposes age as a conditioning factor for the appearance of primary sarcopenia.
On the other hand, in Chile, the prevalence of sarcopenia with EWGSOP was 19.1%,18 however by age, Costa Ricans in their eighties with sarcopenia have a higher prevalence than Chileans (Costa Ricans 43.5% vs 38.5%). In Brazil19 the reported prevalence was 16.1% in women and 14.4% in men.
Concerning muscle strength, which reflects muscle quality, it is considered a predictor of adverse outcomes.20,21 Cut-off points for weakness are useful for identifying populations that may benefit from interventions to improve muscle strength and function. Costa Rican women were on average weaker (13.65 kg) than Chilean women with sarcopenia (18.7 kg), which raises the question of whether all Latin American countries have the same cut-off point for describing normal muscle strength, as changes in their cut-off point may affect the magnitude of sarcopenia prevalence. 23,24
Another measure that reflects a decrease in strength is the stand-up and sit-down test five times. In the study population, this test was also longer to execute in the nationals than in other Latin American countries; however, it is noteworthy that even in those classified as non-sarcopenic in the CRELES study, the duration was longer than 15 seconds, a cut-off point that reflects an alteration in muscle strength.2 This finding motivates further studies of this variable and its behavior in the national population.
Commonly used measures of physical performance in geriatrics include the short performance battery, gait speed, and the 6-minute walk test; these represent quick, inexpensive, and reliable measures of physical function that can be easily implemented in clinical settings. 25 Currently, those defined in the FNIH are used as cut-off points because of their strong longitudinal associations with disability, mortality25 and because their use has been recommended by other experts.2,11
Regarding the analysis, gait speed was longer in Costa Ricans with and without sarcopenia, compared to the Chilean population. 18 A gait speed value < 0.8 m/sec classifies sarcopenia as severe, which generates greater adverse outcomes such as frailty, falls, low quality of life, disability, and mortality.2 Similar to what was documented by Lera et al.,18,23, an association was found between sarcopenia and falls, physical inactivity, and comorbidities such as CVD and arthritis, which may be related to the decrease in mobility associated with these conditions, which could influence the development of secondary sarcopenia in the Costa Rican population.
Limitations
One limitation is that it is a cross-sectional analysis, as only one round of the CRELES study was included, and therefore causality factors were not analyzed. Another limitation is the absence of body composition parameters to establish correlations with calf circumference. As this was a retrospective study, we worked with existing information.
Local cut-off points are required to identify sarcopenia; however, using the EWGSOP criteria and cut-off points allowed us to compare results with other prevalence studies conducted in other Latin American countries.
Conclusion
In conclusion, the prevalence of sarcopenia was similar to that documented in other Latin American countries (10.26% in our country). It is more prevalent in women, and the older the age, the higher the risk of developing it.
Identifying sarcopenia in elderly adults in Costa Rica will allow us to intervene and prevent functional deterioration, falls, hospitalizations, and death, all of which are events related to sarcopenia.
Abbreviations: CP, calf circumference; CRELES, Costa Rica longevity and healthy aging study; EWGSOP, European Working Group on Sarcopenia in Elderly People; CVD, cerebrovascular disease; FNIH, Foundation for the National Institutes of Health Sarcopenia Project; OR, odds ratio. Conflicts of interest: The authors declare no conflicts of interest in the preparation of this article. Envejecimientocr@gmail.com
Referencias
1. Studenski SA, Peters KW, Alley DE, Cawthon PM, McLean RR, Harris TB et al. The FNIH sarcopenia project: rationale, study description, conference recommendations, and final estimates. J Gerontol A Biol Sci Med Sci. 2014; 69:547-58. doi:10.1093/gerona/glu010 [ Links ]
2. Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T et al. Revised European consensus on definition and diagnosis. Age Ageing. 2019; 48:16-31. doi: 10.1093/ageing/ afy169. [ Links ]
3. Coker R, Wolfe R. Bedrest and sarcopenia. Curr Opin Clin Nutr Metab Care. 2012; 15:7-11. doi: 10.1097/MCO.0b013e32834da629 [ Links ]
4. Legrand D, Vaes B, Matheï C, Swine Ch, Degryse J. The prevalence of sarcopenia in very old individuals according to the European consensus definition: insights from the BELFRAIL study. Age and Ageing. 2013; 42: 727-734. doi.org/10.1093/ageing/aft128 [ Links ]
5. Zhang T, Cao L, Cao T, Yang J, Gong J, Zhu W et al. Prevalence of Sarcopenia and Its Impact on Postoperative Outcome in Patients With Crohn’s Disease Undergoing Bowel Resection. J Parenter Enteral Nutr. 2017;41:592-600. doi: 10.1177/0148607115612054. [ Links ]
6. Bahat G, Tufan F, Killic C, Akpinar TS, Kose M, Erten N et al. Cut-off points to identify sarcopenia according to European Working Group on Sarcopenia in Older People (EWGSOP) definition. Clin Nutr. 2016; 35:1557-1563. doi: 10.1016/j.clnu.2016.02.002 [ Links ]
7. Volpato S, Lara B, Cherubini A, Landi F, Maggio M, Savino E et al. Prevalence and Clinical Correlates of Sarcopenia in Community- Dwelling Older People: Application of the EWGSOP Definition and Diagnostic Algorithm. J Gerontol A Biol Sci Med Sci. 2014;69:438-446. doi: 10.1093/gerona/glt149 [ Links ]
8. Beaudart C, Reginster JY, Slomian J, Buckinx F, Locquet M, Bruyère O. Prevalence of sarcopenia: the impact of different diagnostic cut-off limits. J Musculoskelet Neuronal Interact. 2014 Dec;14:425-31 [ Links ]
9. Buckinx F, Landi F, Cesari M, Fielding R, Visser M, Engelke K et al. Pitfalls in the measurement of muscle mass: a need for a reference standard. J Cachexia Sarcopenia Muscle. 2018; 9: 269- 278. 10.1002/jcsm.12268 [ Links ]
10. Newman AB, Kupelian V, Visser M, Simonsick E, Goodpaster B, Nevitt M et al. Health ABC Study Investigators. Sarcopenia: alternative definitions and associations with lower extremity function. J Am Geriatr Soc. 2003; 51:1602- 1609 [ Links ]
11. Cruz-Jentoft AJ, Landi F, Schneider SM, Zuñiga C, Arai H, Boirie Y et al. Prevalence of and interventions for sarcopenia in ageing adults: a systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing. 2014; 43:748-759. doi:10.1093/ ageing/afu115 [ Links ]
12. Arango-Lopera VE, Arroyo P, Gutiérrez-Robledo L, Pérez-Zepeda M. Prevalence of sarcopenia in Mexico City. Eur Geriatr Med. 2012; 3: 157-160. doi:10.1016/j.eurger.2011.12.001 [ Links ]
13. Pérez-Zepeda M, Sánchez-Garrido N, González- Lara M y Gutiérrez- Robledo LM. Sarcopenia prevalence using simple measurements and population-based cutoff values. J Lat Am Geriatr Med. 2016; 2: 8-13 [ Links ]
14. Woo J. Nutritional interventions in sarcopenia: where do we stand? Current Opinion in Clinical Nutrition & Metabolic Care. 2018; 21:19-23. doi:10.1097/MCO.0000000000000432 [ Links ]
15. Rosero-Bixby L, Fernández X, and Dow W. CRELES: Costa Rican Longevity and Healthy Aging Study, 2005 (Costa Rica Estudio de Longevidad y Envejecimiento Saludable). Disponible en: http://ccp.ucr.ac.cr/index.php/ creles-inicio.html [ Links ]
16. Rosero-Bixby L. CRELES- Costa Rica: Estudio de Longevidad y Envejecimiento Saludable. Poblac Salud Mesoam. 2007; 5. Disponible en: http://revistas.ucr.ac.cr [ Links ]
17. Samper-Ternent R, Reyes-Ortiz C y Cano C. Frailty and sarcopenia in Bogotá: results from the SABE Bogota ́ Study. Aging Clin Exp Res. 2017 Apr;29:265-272. doi: 0.1007/s40520-016-0561-2 [ Links ]
18. Lera L, Albala C, Sánchez H, Angel B, Hormazabal MJ, Márquez C, Arroyo P. Prevalence of Sarcopenia in Community- Dwelling Chilean Elders According to an Adapted Version of the European Working Group on Sarcopenia in Older People (EWGSOP) Criteria. J Frailty Aging. 2017; 6: 12- 17. doi: 10.14283/jfa.2016.117 [ Links ]
19. Alexandre T da S, Duarte YA de O, Santos JLF, Wong R, Lebrão ML. Prevalence and associated factors of sarcopenia among elderly in Brazil: findings from the SABE study. J Nutr Health Aging. 2014;18:284-90. doi:10.1007/s12603-013-0413-0 [ Links ]
20. Rolland Y, Lauwers-Cances V, Cournot M et al. Sarcopenia, calf circumference, and physical function of elderly women: a cross-sectional study. J Am Geriatr Soc. 2003; 51: 1120-1124 [ Links ]
21. Landi F, Onder G, Russo A et al. Calf circumference, frailty and physical performance among older adults living in the community. Clin Nutr. 2014; 33: 539-544. doi: 10.1016/j. clnu.2013.07.013 [ Links ]
22. Velázquez M, Irigoyen M, Lazarevich I, Delgadillo J, Acosta P, Zepeda M. Comparison of the prevalence of sarcopenia using skeletal muscle mass index and alf circumference applying the European consensus definition in elderly Mexican women. Geriatr Geront Int. 2017;17:161-170. doi: 10.1111/ggi.12652 [ Links ]
23. Lera L, Ángel B, Sánchez H, Picrin Y, Hormazabal M, Quiero A y Albala C. Estimación y validación de puntos de corte de índice de masa muscular esquelética para la identificación de sarcopenia en adultos mayores chilenos. Nutr Hosp. 2015;31:1187-1197. doi: 10.3305/ nh.2015.31.3.8054 [ Links ]
24. Masanés F, Rojano X, Salvá A, Serra-Resach JA, Artaza I, Formiga F et al. Cut-off Points for Muscle Mass - Not Grip Strength or Gait Speed - Determine Variations in Sarcopenia Prevalence. J NUTR Health Aging. 2017;21:825- 829. doi: 10.1007/s12603-016-0844-5. [ Links ]
25. Alley D, Shardell M, Peters K, McLean R, Dam T, Kenny A et al. Grip strength cutpoints for the identification of clinically relevant weakness. J Gerontol A Biol Sci Med Sci. 2014 May;69:559- 66. doi:10.1093/gerona/glu011. [ Links ]
26. Syddall H, Westbury L, Cooper C, Sayer A. Self- reported walking speed: a useful marker of physical performance among community-dwelling older people? J Am Med Dir Assoc. 2015; 16: 323-328. doi:10.1016/j. jamda.2014.11.004 [ Links ]
Received: March 02, 2021; Accepted: August 19, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
