










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.58 n.2 San José Apr./Jun. 2016 Epub June 01, 2016
Articles
Ovarian lesions in pediatrics age. Retrospective study of 10 years
1Área de Salud Alajuela Sur / CAIS “Dr. Marcial Fallas Díaz”.
2Servicio de Oncología, Hospital “Dr. Rafael Ángel Calderón Guardia”.
3Servicio Cirugía General-Cirugía Pediátrica, Hospital “Dr. Maximiliano Peralta Jiménez”.
The purpose of this article is to understand the behavior of ovarian lesions in pediatric patients in Costa Rica, to improve their management and compare the results with other countries.
Ovarian masses, whether cystic, solid, or both, are a pathology considered rare in pediatric age and although its actual incidence is unknown, it is estimated that it occurs in about 2.6 for every 100 000 girls per year.1 8.0% of abdominal tumors in children are due to ovarian tumors.2
Simple cysts and teratomas are the most common lesions, mostly benign.3
Ovarian masses can be divided into nonneoplastic lesions and neoplastic lesions.
The ovarian tumors of malignant nature are rare in pediatric age, accounting for 2.0 to 10.0% of ovarian masses that occur in this population.4
Of these lesions, tumors derived from germ cells are the most common, ranging between 47.3 and 87.7%.5
Clinically, benign and malignant lesions are indistinguishable, also they may be asymptomatic and, therefore, diagnosed in routine tests.6 These lesions can have multiple presentations.7
Symptoms are usually insidious, and the tumor has reached a large size when diagnosed. Sometimes the discovery of these is when the patient undergoes a surgical procedure for presenting symptoms consistent with appendicitis,7 or by an ultrasound performed for another reason.
The main clinical manifestation is, with or without abdominal pain, pelvic or abdominal mass, which can be acute or chronic, as ovarian torsion occurs or not.8
As a group, these lesions occur in a spectrum ranging from functional cysts (non-neoplastic) ovarian torsion,1 and from neoplasia with a range of pathology going from a high level of malignancy, to benign tumors and cysts.7
The course of action in the presence of an ovarian tumor depends on the type lesion and age of the child.
The infants with suspected ovarian tumor should be referred to a specialized oncologic center, for further study.6
Ovarian pathology can be approached in different ways: laparotomy, laparoscopy and vaginal route.9
The best operation for pediatric malignant ovarian tumors is still controversial. In general, a surgical operation with fertility preservation (unilateral salpingooophorectomy) is recommended.
Methods
A non-experimental study was conducted, a retrospective longitudinal type and descriptive subtype, with an observational range, comprising a quantitative approach. Records of the girls were studied that were treated for ovarian lesions at the Max Peralta Jiménez Hospital, in the period of 2003-2013.
For data analysis a MS Excel program was used in its latest available version. It met all the requirements and was approved by the Local Committee of Bioethics of the MPH.
According to the Statistics Department of the Hospital, it had 16 diagnosed cases with the disease under study; because of the informed consent for the review of records it was unobtainable in 2 cases, a total of 14 cases were reviewed, of which 13 were used in the investigation, since it did not meet the inclusion criteria.
The study was conducted with data from 17 ovarian lesions, because one of the girls had 3 different lesions in the same ovary and two girls presented with bilateral involvement.
Results
The diagnosis was made in 8 girls (61.5%) in the range of 10 to 12 years, 4 infants (30.7%) between 0 and 9 years old and only one patient (7.6%) was diagnosed in prenatal age. The average age of diagnosis was 9.15 years.
The most frequently observed clinical manifestation was abdominal pain in 7 girls (53.8%); in 3 patients (23.0%) diagnosis was made by ultrasound, and vomiting manifested in 2 patients (15.3%), as well as the presence of a palpable mass; the transvaginal bleeding (TVB) was found as the main diagnosis manifestation in only one patient (7.9%).
Regarding the laterality, the right ovary was the most affected, covering 61.5% (n=8), followed by the left side in 23.0% (n = 3) and the bilateral involvement in 15, 3% (n=2).
In the prenatal age, the only patient studied obtained diagnosis by ultrasonographic finding. Of the 4 cases between 0 and 9 years, 3 (75.0%) they were manifested by abdominal pain and 1 (25.0%) through a finding by US; in the age group between 10 and 12 years, the most frequent manifestation was the presence of abdominal pain in 4 (50.0%) girls, followed by vomiting 2 (25.0%) and palpable mass in the same number of patients; the presence of TVB was clear in one of the girls (12.5%), and the diagnosis was made by ultrasonographic study (12.5%).
Of the lesions, 58.8% (n = 10) included nonneoplastic lesions, and 41.1% (n = 7), neoplastic lesions.
The most common condition was of benign origin, with 6 reported cases (87.7%), while its malignant counterpart was documented only in one case (14.2%).
Of the 10 non-neoplastic ovarian lesions, simple cyst was the most common type, comprising 70.0% (n = 7), whereas the presence of hemorrhagic cyst, of inclusion and of corpus luteum, was reported only one case each (10.0%).

Figure 1: A. Mature cystic teratoma 12 cm long, extracted from a 9 year old girl, who presented abdominal pain in the left iliac fossa, of a month of evolution. B-C. Pure dysgerminoma, of 30 x 20cm, weighing 2kg, present in a 12 year old girl, identified as a palpable abdominal mass on physical examination
The simple cyst was the most frequent benign histology in 43.7% of benign lesions (n = 7), followed by the mature cystic teratoma in 37.5% (n = 6); hemorrhagic cysts, inclusion and corpus luteum, were reported in one case (6.2%) each. The only malignant lesion was a dysgerminoma (Figure 1).
Clinical manifestations in non-neoplastic lesions were distributed as follows: abdominal pain in 5 patients (50.0%) patients, vomiting in 2 (20.0%), as well as the ultrasonographic finding and the transvaginal bleeding manifested in one of the patients (10.0%).
In benign tumors, the most common clinical manifestation was abdominal pain in 50.0% (n = 3), the other symptoms and ultrasonographic finding in one case each, with 16.6%.
The only malignant lesion was diagnosed by the presence of a palpable mass.
The surgical method that was performed for the management of ovarian pathology in the girls was a laparotomy, in 76.9% (n = 10) of the interventions; the laparoscopic approach was used twice (15.3%), and for one of the girls (9.6%) both approaches were made.
Despite these results, in recent years in a hospital it has been implemented the laparoscopic surgical method of choice for these patients.
The most commonly used surgical technique was salpingo-oophorectomy in 41.1% (n=7), followed by the total oophorectomy in 29.4% (n = 5), partial oophorectomy with 17.6% (n = 3) and finally, the fenestration and cyst aspiration, performed in two lesions, with 11.7%.
Discussion
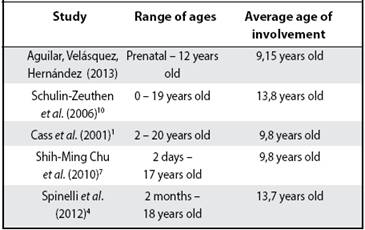
In all studies, the mean age of involvement is very similar, ranging between 9 and 13 years (Table 1).
Abdominal pain is the manifestation most frequently found in all studies, appearing between 48.6% and 86.0% of lesions,4-10 followed by the identification of a palpable mass in the 8.3 to 27.0% of cases.4-10 It is worth mentioning the relationship between clinical manifestation and the result of the histopathological finding of the lesions, in terms of its characteristics of benignity or malignancy, where the abdominal pain was found widely associated with benign lesions, while the presence of a palpable mass was the clinical finding in the only patient with a lesion of malignant histopathologic characteristics.
Non-neoplastic ovarian lesions show a slight predominance over neoplastic lesions.1-4-11
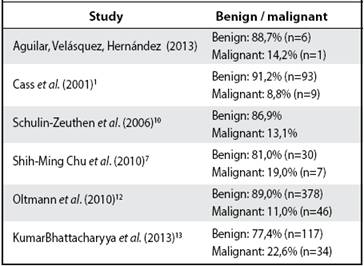
There is a significant prevalence of benign ovarian lesions compared with those that manifest a histology compatible with malignancy (Table 2).
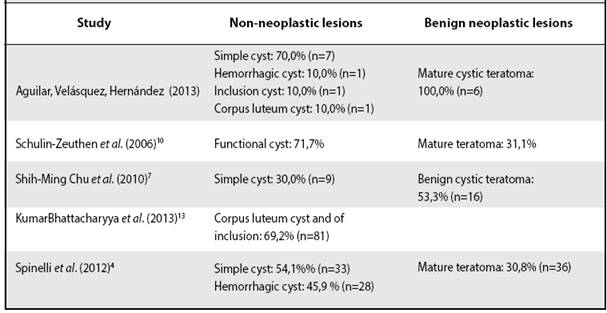
Regarding non-neoplastic lesions, a predominance of simple cysts was observed, and the superiority of teratoma in neoplastic lesions with benign character (Table 3).
Laparotomy surgery represents the largest number of interventions, occurring in 67.0% to 79.9% of interventions,4-7 however, now the use of laparoscopy is taking dominion in regards to the management of the ovarian lesions in pediatric patients.
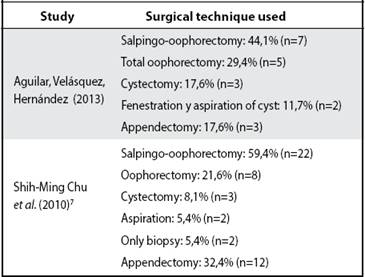
The salpingo-oophorectomy is the most widely surgical technique used for the management of ovarian lesions in this population (Table 4).
Work performed in the “Dr. Maximiliano Peralta Jiménez” Hospital.
Affiliation of authors: 1South Alajuela Health Area/ “Dr. Marcial Fallas Diaz” CAIS. 2Department of Oncology, “Dr. Rafael Angel Calderon Guardia” Hospital. 3General-Pediatric Surgery Department, “Dr. Maximiliano Peralta Jiménez” Hospital. Abbreviations: MPH, “Dr. Maximiliano Peralta Jimenez“; TVB, transvaginal bleeding; US, ultrasound. iseaghe91@gmail.com
Referencias
1. Cass DL, Hawkins E, Brandt ML, Chintagumpala M, Bloss RL, Milewicz AL, et al. Surgery for ovarian masses in infants, children, and adolescents: 102 Consecutive Patients Treated in a 15-Year Period. J Pediatr Surg. 2001;36:693- 699. [ Links ]
2. Kumar BN, De A BP, Mongal S, Chakraborty S, Bandopadhyah R. Ovarian tumors in pediatric age group - A clinicopathologic study of 10 years cases in West Bengal India. Indian J Med Paediatr Oncol. 2010;31:54-57. [ Links ]
3. Karpelowsky JS, La Hei ER, Matthews K. Laparoscopic resection of benign ovarian tummours in children with gonadal preservation. Pediatr Surg Int. 2009;25:251-254 [ Links ]
4. Spinelli C, Pucci V, Buti I, Liserre J, Messineo A, Bianco F, Ugolini C. The role of tumor markers in the surgical approach of ovarian masses in pediatric Age: A 10-year study and a literature review. Ann Surg Oncol. 2012;19:1766-1773. [ Links ]
5. Vaysse C, Delsol M, Carfagna L, Bouali O, Combelles S, Lemasson F, et al. Ovarian germ cell tumors in children. Management survival and ovarian prognosis. A report of 75 cases. J Pediatr Surg. 2010;45:1484-1490. [ Links ]
6. Carvalho M, Sucesso MB, Ferreira AM, Norton L, Estevinho N. Patologia ovárica num centro oncológico pediátrico. Nascer e Crescer. 2011;20:69-72. [ Links ]
7. Shih-Ming C, Yung-Ching M, Hsun-Chin C, Jin-Yao L, Jeng-Chang C, Chao- Ping Y, et al. Ovarian Tumors in the Pediatric Age Group: 37 Cases Treated over An 8-year Period. Chang Gung Med J. 2010;33:152-156. [ Links ]
8. Quero A, Estrada R, Tenorio H, Álvarez RM. Tumor de células germinales de ovario: Características clínicas y resultados del tratamiento. Red de Revistas Científicas de América Latina y el Caribe, España y Portugal. 2007; 75:81-85. [ Links ]
9. Dietrich SC, Gehrich A, Bakaya S. Surgical exposure and anatomy. Surg Clin North Am 2008; 88:223-243. [ Links ]
10. Schulin-Zeuthen CP. Tumores anexiales en niñas y adolescentes: experiencia del Hospital Clínico de la Universidad Católica de Chile 1991-2003. Rev Chil Obstet Ginecol. 2006;71:174-183. [ Links ]
11. Morowitz M, Huff D, Von Allmen D. Epithelial ovarian tumors in children: a retrospective analysis. J Pediatr Surg. 2003;38:331-335. [ Links ]
12. Oltman SC, García N, Barber R, Huang R, Hicks B, Fischer A. Can we preoperatively risk stratify ovarian masses for malignancy?. J Pediatr Surg. 2010;45:130-134. [ Links ]
13. Kumar N, De A BP, Mongal S, Chakraborty S, Bandopadhyah R. Ovarian tumors in pediatric age group - A clinicopathologic study of 10 years cases in West Bengal India. Indian J Med Paediatr Oncol. 2010;31:54-57. [ Links ]
Received: August 24, 2015; Accepted: February 04, 2016
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
