










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.55 n.3 San José Jul./Sep. 2013
Original
Mental
health panel 2011, conclusions and future steps
Javier
Contreras-Rojas1 y Henriette Raventós1,2
Authors ‘affiliations:
Background:
Health is a social process that seeks
physical and mental wellbeing through every stage of the individual’s
life. In spite of great efforts, in
Methods: Adiscussion
forum
on mental health with participation of health providers, researchers,
policy
makers and users of health services.
Results:
Representatives from 148 organizations and
institutions participated. There is a lack of salutogenic
indicators and minimal assessment of the impact of prevention and
promotion of mental
health. Only one program for psychosocial rehabilitation was
identified.
Conclusion:
The discussion process included users,
who, along with other actors identified needs and priority action
areas. The
difficulties related to the implementation of a specific action plan
are the
main barrier to achieve effective mental health promotion, treatment
and
rehabilitation.
There are
specific programs, but in the majority of
cases, their effectiveness is unknown. It is necessary to establish a
leading
institution and strengthen its role to ensure the success of a national
mental
health program.
Keywords:
National Mental Health Program, Caja Costarricense
It can be
said that health, as a state of complete
well-being through the stages of life, is not possible without a
healthy,
economic, cultural and social environment that includes coverage of
basic needs
(employment, housing, food, education, recreation).1 There
is
consensus that the healing model is inefficient, expensive, and
produces less
wellness than the promotion of prevention.2 The traditional
model of
medical care (physician-centered) has proven to be inefficient; the
patient
assumes a passive and irresponsible attitude of his condition, which
makes
difficult the prevention and control of mental illness. The alternative
model
includes the addition of three strategies: prevention and health
promotion,
care and rehabilitation.
1.
Prevention and promotion: the
individual is the main actor,
a subject with rights, but also duties on their own health. Education
empowers
a person to acquire the compromise on his health.3 The
State, in
turn, is responsible for ensuring the rights of a job, housing,
education,
food, health services and a social and work environment free of
violence and
environmental pollutants. In childhood it is especially important to
have a
healthy environment, protective factors such as immunization, hygiene
and
adequate food, and guidance from parents and other adults in charge of
the care
and formal education.
2.
Attention: the user
must participate in the process of diagnosis
and treatment; he must have full information about his disease,
treatment
options, the natural history of the disease and indicators that allow
early
recognition of a decompensation. All
people should
have access to prompt diagnosis, modern pharmacological and
non-pharmacological
treatments, evidence-based care and non-institutionalized attention,
that is
less restrictive of their liberties.4 Ideally,
these resources should be available at the community level.
3.
Rehabilitation: chronic mental illness (organic
psychoses, schizophrenia and bipolar disorder), with an onset in
adolescence or
early adulthood, usually leads to some level of impairment or
disability. The
deterioration is less if a proper and prompt treatment is established
since the
first outbreak, that further may decrease
the intensity
and frequency of decompensations. Long
periods of
hospitalization and confinement also increase the deterioration.5 Rehabilitation
includes strategies that ensure family involvement and that allow an
adequate
social reintegration.
Some
mentioned are: 1. the National Mental Health Plan
has no funding; 2. poor awareness and empowerment of health teams; 3.
attention
mainly based on a pharmacological approach; 4. insufficient human
resource
trained in mental health; 5. 3% of national health expenditures
designated for
mental health in the CCSS, 67% is for the two psychiatric hospitals and
the
remaining 33% for other health services and prevention activities; 6.
lack of
updated prescription drug protocols 7. poor
mental
health training in primary care; and 8. lack
of
planning and research in mental health, so there is a big gap in
knowledge
about the epidemiological profile of mental disorders in the country.
The final
report of the specialty in psychiatry,
conducted by the CCSS Internal Audit in 2010, identifies specific
mental health
needs.7 It recommends the following to the medical
management: 1. to
perform a situational diagnosis of the major mental illnesses
nationwide; 2. to
adjust the Institutional Plan on Mental Health to what is established
by the
Ministry of Health in the National Health Plan; 3. to create a
strategic
timetable for the implementation of this action plan; 4. to develop
guidelines
of the procedures for psychiatric care at all three levels, 5. to make
a
disclosure schedule and training plan for the three levels based on
these guidelines,
6. according to the Executive Decree No. 20665 -S (October 29th, 1991
), in
which psychiatry is declared as the fifth clinical specialty, to
prepare a
technical study to assess the availability of human, technological and
economic
resources for mental health; 7. to assess
the
appropriateness of removing the hierarchical dependence of psychiatry
from the
Chief of the Medicine Department, 8. to
develop a strategy
to strengthen regional mental health services in order to comply with
the
Declaration of Caracas.8 9. to
update the
projections defined in the document “Needs of Medical Specialists for
the
Costa Rican Social Security” (CENDEISSS ). 10. through
the participation of the Direction in Development of Health Services,
to
perform a technical study of the feasibility of extending the time in
each psychiatric
consultation, 11. to coordinate the
country.
Currently,
various efforts are undertaken, that are
aimed at promoting and improving mental health. The draft of the Mental
Health
Policy is based on the following principles: intersectoral
and interagency coordination, allocation of institutional resources as
required; updating the legislation, extending coverage to different
levels of
participation, development of specific action plans; rights approach,
risk,
gender and diversity, permanent learning team of mental health
awareness
campaigns to combat stigmatization, increasing the number of mental
health
professionals, research and impact assessment.
This
article aims to present the discussions on mental
health issues, taking into account the feedback provided by other
equally
important stakeholders. In addition to the participation of the State
authorities and service providers, it has the participation of patients
and
families. It briefly describes the methodology of the Forum and the
conclusions
are discussed, as exposed by the participants.
Methods
A forum
for consultation and discussion on mental
health was organized with the participation of different actors among
which
are: 1. providers of care, support and rehabilitation 2. researchers
3. persons who define the policies at
governmental
level, and 4. users and their families
through several
non-governmental organizations (NGOs). This discussion was held at the
headquarters of the Inter-American Institute of Human Rights (IIHR)
located in
Los Yoses, Montes de Oca,
on October 10, 2011, moderated by Dr. Henriette
Raventos Vorst, a researcher at the
The goal
was to identify gaps in knowledge about the
situation and mental health interventions in
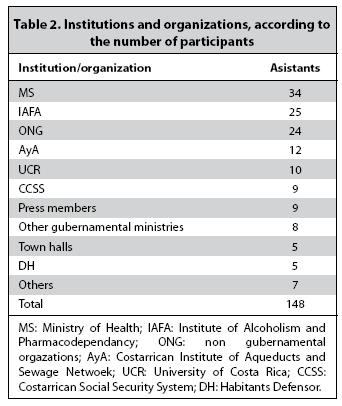
Results
The forum
was attended by 148 representatives of
various institutions and organizations. Table 2 summarizes
the institutions and
organizations represented in the activity.
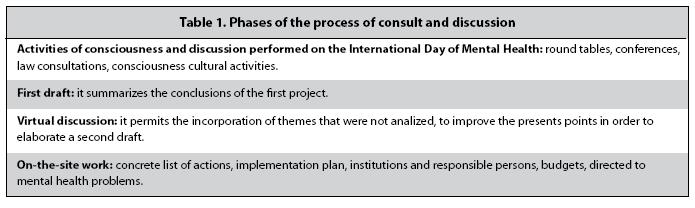
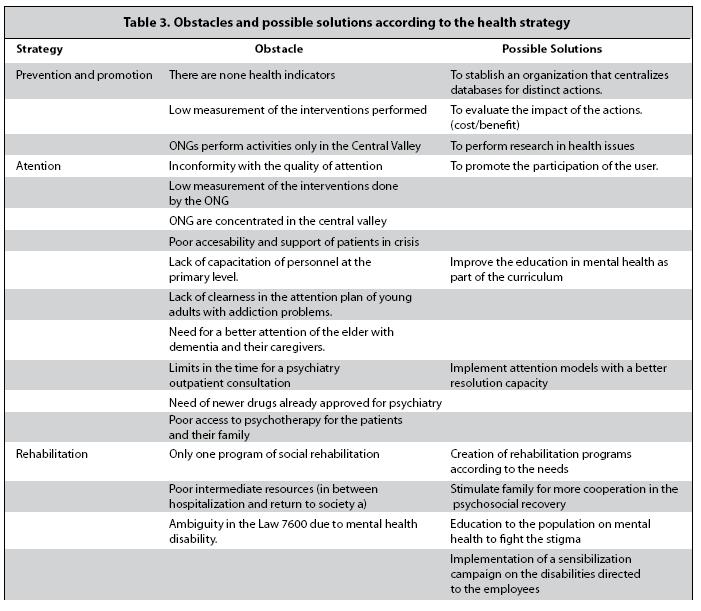
This
document is the second draft mentioned in point
2, which is the working tool for the development of a preliminary
action plan. Table
3 summarizes the barriers identified and the possible solutions
raised by
attendees. Following the recommendations of various international
organizations, the findings are grouped according to the health
strategy to
follow.
Discussion
As stated
by the executive director of IIHR in
Sisy
Castillo Ramírez, MD (Viceminister
of Health) and Mary Rose Madden Arias (IIDH), mentioned that there are
still
legal gaps, for example, the Law against Workplace Bullying. Other laws
also
necessary are those that ensure equal rights for all citizens (for
example,
laws for corporate cohabitation of same-sex couples, for the regulation
of
biomedical research, monitoring of tabaco
advertising, and in vitro fertilization). In some cases, the existing
laws lack
additional legal instruments (for example: regulations) to ensure its
implementation.
Examples
of interventions in prevention and promotion
Among the
interventions discussed are: 1. Prevention
of drug use (IAFA), 2. Protocols for the
prevention of
violence in schools (Ministry of Education), 3. Community
care of the elderly (National Hospital of Geriatrics and Gerontology
Dr. Raúl Blanco Cervantes), 4. Management
of moral and workplace bullying (MS), 5. networks
for preventing minors in psychosocial risk (Saint- Exupéry
Foundation), 6. other interventions such as
yoga, art
and dance. The only programs that mentioned measurements to determine
the
impact of the intervention are the drug use prevention programs of IAFA
and the
networks for preventing minors in psychosocial risk of the Saint- Exupéry Foundation. But only Saint- Exupéry Foundation showed the results. The IAFA
still has no data since the first evaluation will be until 2012.
Members of the
Prevention
and promotion strategies
To set the
priority promotion strategies that can be
scaled for prevention and promotion, we recommend: to make a list of
all
interventions being undertaken by different organizations, including
but not
limited to CCSS, ministries, IAFA, National Children´s
Board (PANI), UCR and NGOs; to document the results of such research in
order
to measure the impact and compare their effectiveness according to
cost/benefit
issues, and to create/designate an entity with leadership to centralize
information from different sectors/ organizations. To have an inventory
of the
current actions is essential to avoid duplication of efforts and to
make more efficient
the use of the resources. A specific example, such as school dropout
prevention, is also vital to ensure proper growth and access to
opportunities. A
healthy environment, free from violence, harassment, insults (for
example
drugs, smoking and other environmental pollutants), is
extended from the home, community, school and workplace.
Examples
of interventions in care
The
approaches of the Costa Rican Foundation of
Bipolar Disorder (FUCOTBI) and the Costa Rican Association of Recurrent
Affective Disorders (REFINE) were presented. Both NGOs provide care for
people
with mood disorders (for example psychoeducation
for
patients and family members, individual and group psychotherapy). They
also
conduct education campaigns through formal and informal means, whose
goal is to
reduce stigma. Concrete actions were presented, but no instruments are
designed
to measure its impact. It was also mentioned that care activities
undertaken by
NGOs are limited to the
The public
manifested the following complaints about public
services in mental health care: difficulty in getting transportation
for a decompensated patient from home to
the medical center; the
general practitioner has insufficient training or sensitivity for the
detection, diagnosis and treatment of such diseases, treatment for
adolescents
that onset on drug abuse is poor, there is little support for
caregivers of the
elderly with dementia, the outpatient psychiatrist consultation at the
CCSS
lasts only 15 minutes, the access to new psychotropic drugs is limited,
and
these drugs often must be purchased privately, and the availability of
psychotherapy in most centers is very limited.
Intervention
strategies in attention
To set the
priority strategies in the axis of care for
people with neuropsychiatric illness, it is essential to have the
opinion of
the user and family.9 These can
provide
vital information regarding their needs and expectations of attention
at the
social security level. Training of primary care level in the diagnosis
of
mental and behavioral disorders should also be improved. More training
at the
primary level will allow earlier and better timed diagnosis,
that will reduce the risk of complications. Increased efficiency
in the
management of these patients at primary and community level would
decrease the
burden of dating in psychiatric services, which is a practical measure
to
address the current lack of specialists.10These actions
should
follow international recommendations and algorithms for priority
treatment of
mental illness. An implementation plan that includes impact measurement
is
required. Finally, it should be analyzed in a reasonable time, the
effectiveness of the proposed changes, and an effective promotion
intervention
to increase coverage. A possible solution is that impact studies are
carried
out on a pilot basis by NGOs and then that the CCSS assumes the
obligation to
implement them if they prove to be successful.
Stigma is
the main reason why individuals do not seek
professional mental health care.11 Fear of being labeled as
“crazy”, makes people not receive early help, the diagnosis is
delayed, the disease takes a more torpid course, and there is an
increase in
management complications and a worse overall prognosis. In other
countries,
education (both patients and families, and the general population,
mental
health issues ) and exposure of disadvantaged groups (in this case
mental
patients) are the most effective measures to combat the stigma.12 In
Costa Rica an educational plan that involves mass media and that
reaches most
of the population is required. More empowered and better self-esteem
patients
have more chance to fight for their rights, ensuring a better quality
of life. Psychotherapy
in all its forms should accompany drug therapy. Other complementary
therapies
that may be incorporated in care include: zootherapy,
dance therapy, yoga therapy, art therapy (these are discussed in more
detail in
the next section).
Examples
of interventions in the rehabilitation axis
The day
hospital service at the
It is
noted that the only existing rehabilitation
program is confined to a hospital room in a single medical center. This
makes
access to remote areas and users can create resistance in patients with
negative experiences at the center. Also unveiled complementary
therapies based
on interaction with dogs, dance, art, yoga and voice in radio. These
are
relatively recent forms that do not yet have impact measurement in
between.
Intervention
strategies on the shaft rehabilitation
In
addition to the feedback provided by relatives and
patients, it is recommended that these programs are accessible to
people around
the country. It should important to use the existing community
facilities such
as educational or religious centers. Social reintegration with more or
less autonomy, that depends on each case,
must ensure the
possibility of obtaining work and haousing.13 It is
considered that
employability will enhance with information campaigns to reduce stigma
and
educate employers on the necessary adjustments to people with
disabilities or
mental illness. Education in general should seek to eradicate myths
about
people with mental illness, to change the view of the family, the
community the
media and the same health personnel. It is important to develop
training
programs to improve the skills of this group and to achieve greater
competitiveness in the labor market. In terms of housing, the
feasibility of
having families, supportive homes or intermediate shelters should be
explored.
Mental
health is inseparable from the health and
general welfare of the people. The most effective strategies are, in
general,
health promotion, which are collective obligations within an
ideological
framework of the country, where all citizens have access to a healthy
environment, education, housing, food, employment, recreation, so they
can
carry out their life plans. It is urgent to define an agenda of
interventions that
they are escalated in a short, intermediate and long period of time.
The goal
of this effort is to list specific actions prioritized by the
participants of
the discussion. It is pertinent to ensure respect for the rights and
confidentiality of information, the right to appropriate treatment, and
the
right to free will and informed consent.
Conflict
of interest: no conflict of interest.
Acknowledgments:
The authors thank all participants of
this forum.
References
1. WHO. Basic documents. 43rd ed.
2. WHO. Primary prevention of mental, neurological and psychosocial disorders.
3. Bowie CR, Twamley EW, Anderson H, Halpen B, Patterson TL, Harvey PD. Self-assessment of functional status in schizophrenia. J Psychiatric Res 2007;41:1012–1018. [ Links ]
4.
5. Landon BE, Gill JM, Antonelli RC, Rich EC. Prospects for rebuilding primary care using the patient-centered medical home. Health Aff 2010;29:827–834. [ Links ]
6. Informe de la Evaluación del Sistema de Salud Mental en Costa Rica utilizando el Instrumento de Evaluación para Sistemas de Salud Mental de la OMS (IESM-OMS) COSTA RICA 2008. [ Links ]
7. CCSS, Auditoría Interna. Área de Servicios de Salud. Informe en la especialidad de psiquiatría de la red de servicios de salud. Oficio: ASS-347-2010, 24 de noviembre de 2010 (documento impreso). [ Links ]
8. Iniciativa Regional de reestructuración de la Atención Psiquiátrica. Declaración de Caracas 1990. [ Links ]
9. Funk M, Minoletti A, Drew N, Taylor J, Saraceno B. Advocacy for mental health: roles for consumer and family organizations and governments. Health PromotInt, 2006, 21:70-75. [ Links ]
10. Daly R: Psychiatry could benefit from education, work force changes. Psychiatric News, May 7 2010, 4,28. [ Links ]
11. Eaton J, Agomoh AO. Developing mental health services in
12. Wahl OF. Media madness: public images of mental illness.
13. Chatterjee S, Pillai A, Jain S, Cohen A, Patel V. Outcomes of people with psychotic disorders in a community-based rehabilitation programme in rural


{kind=link}
{kind=link}
{kind=link}