











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
The temporomandibular joint includes the articular disc, the rounded end of the mandible (mandibular condyle) and the edge of the temporal bone (glenoid fossa). The articular disc is located amid the condyle and fossa. The ligament of the temporomandibular region facilitates lateral stability by overlying the joint. The TMJ is surrounded by a capsule filled with synovial fluid, which provides lateral stability. Lubrication and essential nutrients for the joint are provided by synovial fluid. In the absence of synovial fluid, there is increased shear stress and friction that leads to disc degeneration (1).
TMJ
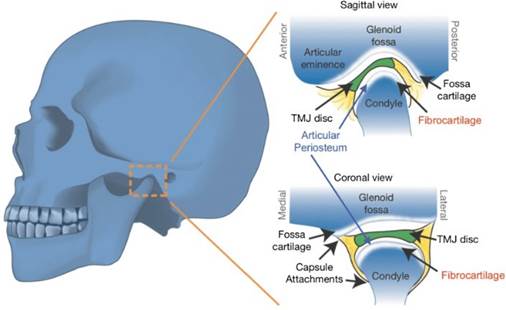
The meniscus or articular disc is situated in the donut-shaped joint capsule. The joint capsule is thicker at the edges and thinner in the middle. The articular disc consists of fibrocartilage, which is different from other joints that consist of hyaline cartilage. This disc has an important role in absorbing shock, distributing loads and accommodating joint movements. The disc is connected to the condyle of the mandible in either direction via ligaments. Blood supply to the TMJ and the associated muscles is facilitated through the branches of maxillary arteries and external carotids. There is no blood supply to the central region of the disc. The anterior and posterior regions of the disc are flexibly associated with the condyle. This association acts as a hinge during condyle movements. This inconsistent association may sometimes lead to instability of the disc. The sagittal and coronal views of the TMJ are shown in Figure 1.
The disc divides the joint into two different fluid-filled sections. These compartments have specific purposes. The lower part is included in rotational movement. The lower part includes the mandibular condyle, associated ligaments, articular disc and other structural forms. The mandible moves from the closed condition to an open condition through this rotational movement. The upper part is included in the gliding or translational movement of the joint. In this movement, the disc moves against the temporal bone, and the movement of the disc with the temporal bone as well as the condyle with the joint slope will lead to mouth opening (1).
In the developmental stages, the growth center of the mandible is present below the lining of fibrocartilage, making the mandible vulnerable to damage caused by pathological factors. The articular disc and mandibular condyle can undergo adaptive remodeling throughout their lifetime according to the masticatory system’s functional requirements. When the adaptation demands exceed individuals’ biological capacity, atypical joint mechanics and mechanical stress can lead to osteoarthritis or joint degenerative disease (3).
Anatomy and physiology of the TMJ
The TMJ is a joint that can move freely and can be termed the ginglymoarthrodial joint. It is composed of articular cartilage, a capsule and synovial cartilage. The capsule covers the TMJ. This joint connects the mandibular condyle to the temporal bone cavity (4).
Basic anatomy
The cranial surface of the TMJ is known as the glenoid fossa. It is composed of the temporal bone’s squamous area; it joins with the jaw’s condyle region. The fossa’s posterior region is called the posterior articular ridge. The postglenoid process is located sideways to it. The postglenoid process region aids in the formation of the upper wall of the external acoustic meatus.
The anterior edge of the temporal bone’s glenoid fossa includes the articular eminence that makes the medial bone prominent at the zygomatic bone’s posterior border. The preglenoid level slightly ascends and proceeds into the articular eminence; it is anterior to the cavity and is present at the base of the skull. This region permits the movement of the articular disk as well as the condyle. The articular tubercle is a bone edge adjacent to the origin of the zygomatic process.
In comparison to the antero-posterior region, the glenoid fossa is broader in the mediolateral region. The lower articular surface of the glenoid process denotes the upper region of the mandible. It comprises the condyle region of the mandible in the anteroposterior direction.
The articular disc has an oval or biconcave shape, intervenes beneath the glenoid fossa and surrounds the condyle. The cartilaginous disc has a posterior part of 3mm and an anterior part of 2mm and has a thinner middle diameter. The front portion of the articular disc has a fibroelastic fascia sheet anteriorly and a fibrous sheet posteriorly. The anterior part is associated with the postglenoid process. It has the function of preventing disc slippage at the time of mouth opening. The lower side of the articular disc avoids increased rotational disk movement in association with the mandibular condyle.
The front part of the articular disc is associated with the articular eminence, the joint capsule and the pterygoid muscle’s upper area. The inferior part of the articular disc is associated with the glenoid fossa, temporal bone, and bilateral tissue of the disc and condyle. The lateral and medial parts of the cartilaginous disc are connected to the condylar foundation of the mandible. The disc edge is partially fused with the joint’s surrounding fibrous capsule (5).
Muscles
Four muscles -the masseter, temporal, and two pterygoids- directly engage the TMJ.
The perimysium of the masseter muscle makes direct contact with the front edge of the articular disc. It has multiple muscle layers and inserts on the coronoid process and the branch of the mandible (lateral surfaces) after it emerges from the zygomatic arch.
Its main function is to raise the jaw. The masseteric branch of the trigeminal cranial nerve provides the muscle with its innervation. The medial face of the zygomatic process and the temporal fossa of the skull serve as the origin of the temporalis muscle, which inserts on the coronoid mandibular process. Similar to the previous muscle, the temporalis can occasionally create anterior contact with the articular disc. As a result, the mandible rises. It is innervated by the deep temporal nerves, which are branches of the trigeminal nerve.
The lower head and the upper head make up the lateral or external pterygoid muscle. The extra- cranial face of the large sphenoid wing and/or the anteromedial face of the condyle neck in the upper part of the pterygoid fovea are the sources of the upper bundle, which is inserted anteriorly to the joint capsule. At the anteromedial aspect, it makes contact with the disc. The inferior head inserts on the pterygoid fovea and arises from the lateral side of the lateral lamina of the pterygoid process of the sphenoid. The jaw protrudes when the external pterygoid is activated bilaterally; however, the mandibular bone deviates to the side when it is activated unilaterally.
In the opening phase of the mouth, the external pterygoid muscle pulls the condyle forward; in the closure phase, it draws the disc anteriorly. When the mouth is first opened and when it is first closed, the two upper and lower bundles are active. The pterygoid fossa, the pyramidal process of the palatine, the maxillary tuberosity, and the internal or medial pterygoid muscle are the origins of this muscle. It ends on the medial face of the angle and the mandibular branch. The mandibular branch of the trigeminal nerve innervates the internal pterygoid, much like it does the external pterygoid. The mandible is raised and protrudes due to the internal pterygoid muscle (6).
Ligaments
Several ligaments, which also send out a multitude of proprioceptive afferents, govern TMJ forces. The proprioception of the joint is influenced by a number of different structures, including the capsule, the periodontal ligaments, the masticatory muscles and the skin. The extent to which the TMJ functions depends on how tightly the articular ligaments feel (7).
Sphenomandibular ligament (SML). A remnant of the Meckel cartilage is the SML. The pterygospinous ligament likewise has its origins in the sphenoid spine. It enters the TMJ through the medial wall on its way to the jaw. It involves the malleus through the petrotympanic fissure and creates some of the fibers of the anterior ligament of the malleus. It proceeds to descend until it reaches the mandibular lingula (sphenoid, middle ear, mouth). Numerous veins, including the mylohyoid nerve, pass through the ligament and contact the pterygomandibular fascia. With the inferior alveolar nerve, the medial meningeal artery, the internal maxillary artery, the auriculotemporal nerve, and the lateral pterygoid muscle, it forms a superior and lateral association. After opening to the mouth at approximately 10 degrees, the TMJ is protected from increased condyle translation.
Stylomandibular ligament (STML). The STML extends from the styloid process of the temporal bone to the posterior edge or angle of the jaw. It is generally characterized by thickening of the parotid fascia and deep cervical fascia. It controls the excessive protrusion of the jaw. The middle ear stapes (via the Reichert cartilage) develop from the first and second branchial arch, which is where it derives embryologically. It passes through the medial pterygoid muscle's inner region along its course.
The pterygomandibular ligament (PTML). The buccopharyngeal fascia thickens to become the PTML, often known as the raphe. It starts from the internal pterygoid plane of the skull's hamulus and extends to the back of the retromolar trigone of the mandibular bone. The pharyngeal constrictor muscle (posterior) and the buccinator muscle (anterior) are two muscles that contact the PTML. According to embryology, the ligament develops from the mesenchymal union of the first and second branchial arches. PTML restricts uncontrolled jaw motions.
Pinto or discomalleolar ligament; malleolomandibular ligament. According to embryology, it originates from the tympanic part. There are two parts to the ligament. The extratympanic area, or the portion of the TMJ joint capsule that is posterosuperior and in contact with the retrodiscal tissues (passing through the petro-tympanic fissure), is concerned with the middle ear in the first case and involves the malleus relative to the anterior ligament of the malleus. There are two distinct purposes. Because of the tensions of nearby structures, the TMJ shields the synovial membrane. It would appear to control or manage the appropriate pressure for the middle ear (8).
The medial and lateral poles of the mandibular condyle are the sites of insertion for two bundles of symmetrical fibers that make up the collateral ligament. These fibers begin at the level of the intermediate fascia of the articular disc. The disc was held firmly against the condyle.
There is a connection between the TMJ and other muscles that move and support the joint. The temporal, masseter, external or lateral pterygoid muscles are responsible for closing the jaw. The internal or medial pterygoid, geniohyoideus, digastric and mylohyoideus muscles are responsible for opening the jaw (9).
The rotation of the discomandibular space occurs before translation when the mouth opens, together with movement of the translational disco- temporal space. The condyle is capable of sliding anteriorly, rotating anteriorly in the medial direction of the opposing condyle, and rotating anteriorly in the same condylar structure. While the condyle on the other side glides forward, the condyle itself can travel backward. With anterior sliding, bilateral or ipsilateral TMJ protrusion can develop.
The intricate movements of the TMJ enable a variety of functions, such as sucking, chewing, swallowing, facial expression, phonation, breathing and mouth opening. These movements also enable retrusion, lateralization, and protrusion of the jaw nd help to maintain the proper level of middle ear pressure (10).
Nerves
A number of proprioceptive receptors, including Golgi-Mazzoni and Ruffini and myelinated and nonmyelinated nerve fibers, are present in the TMJ, especially in the parenchyma of the articular disc. The masseteric nerve, a branch of the second branch of the trigeminal nerve, innervates the articular capsule in the anterolateral section. At the same time, the auriculotemporal nerve of the third branch of cranial nerve V innervates the lateral region of the capsule (11).
Lymphatics and blood supply
The masseteric artery, maxillary artery, superficial temporal artery and other arteries all contribute to the arterial blood supply of the TMJ. Other arterial branches include those from the ascending palatine artery, the rising pharyngeal artery, the exterior carotid artery and the inferior auricular artery. The pterygoid plexus, which communicates with the internal maxillary vein, medial meningeal veins, masseterine veins, deep temporal veins, inferior alveolar vein and sphenopalatine vein, is where venous drainage occurs in the retrodiscal region (12). Because the number of lymph nodes might increase with TMJ illness, lymphatic drainage is not always easy to explain. The lymphatic system that typically affects the TMJ originates in the submandibular triangle region (10).
Etiology of tmj dysfunction
TMDs occur due to complicated and multiple causes. This disorder may be instigated by a wide range of variables, which are divided into 3 categories. Predisposing variables increase the possibility of developing TMD, instigating factors that start the illness, and maintaining factors that impede healing progression or hasten disease progression. One element might occasionally realize one or more such functions. Identification and management of the related components are essential for effective TMD management.
Occlusal anomalies, bruxism, orthodontic therapy, macro- and microtrauma, orthopedic instability, exogenous estrogen and joint laxity are some of the causative variables. TMDs may be triggered by psychological elements, including mental tension, stress, anxiety, and depression.
Occlusal issues
The first and most contentious etiologic cause of TMD is occlusal issues. Costen has conclusively proven that occlusal issues play a part in TMD emergence. Currently, deliberate occlusion is one of the main causes of TMD, as it may contribute to both vulnerability and the development or maintenance of the condition. The research claims that it is now impossible to pinpoint the precise contribution of occlusal variables to temporomandibular joint diseases. On the other hand, Koh et al.'s meta-analysis (13) revealed a lack of evidence for the use of occlusal rebalancing in the prophylaxis or treatment of TMD.
Despite being pathological conditions of the temporomandibular complex, incorrect occlusions caused by dental malocclusions and inadequately treated or untreated edentulism are not thought to be the primary causes of TMD (14). A low occurrence of certain malocclusional characteristics (negative overjet, one-sided open bite, one-sided cross bite of men, and edge-to-edge bite of women) with TMD symptoms or signs has been noted by Badel et al. (15). In the same study, it was discovered that asymptomatic patients had considerably more hyperbalance and interference contacts than did TMD patients. There was no distinction between Angle's classifications in TMD patients and asymptomatic people.
Depending on the etiopathogenesis of TMD, occlusal interferences are seen differently in terms of relevance. Le Bell et al. (16) discovered that healthy people successfully adjust to artificial interference without developing dysfunction symptoms. Artificial interference exacerbates clinical symptoms in individuals with TMD past medical conditions. The existence of an anterior open bite might be seen as the result rather than the cause of articular remodeling (17).
The etiopathogenesis of TMJ problems may also be significantly influenced by condylar posture (18). The associations between centric occlusal- centric association disparity, condylar position, and the presence of TMD symptoms and indicators were assessed in a recent study (19). According to the study's findings, patients with TMD may have condylar transpositions of significant scale and large interarch dental differences if their centric relation-centric occlusion discrepancy is recorded and evaluated. Similar findings were obtained by Weffort et al. (20), who showed that extreme inter- cuspation and statistically substantial differences in centric association could be measured at the condylar stage in both asymptomatic and sympto- matic patients. Recent investigations have stressed the complex disease etiology and diminished the role of occlusion as a primary causative element of TMD (21). Discussions of occlusal features have affected and limited therapeutic options for TMD.
Psychological stress
Occlusal disharmony, contracture, degenerative arthritis and internal disturbances are the results of muscle hyperactivity and weariness caused by anxiety, stress and other associated psychological factors. These factors may alter the occlusal pattern of the chewing cycle, causing modifications more indicative of TMD rather than a cause. According to numerous studies, people who have myofascial pain or arthralgia linked to myofascial pain, osteoarthritis or arthritis have more advanced phases of somatization and depression than people who have disc dislocation (22).
Hormonal reasons
Women are 4 times more likely than men to be affected by TMD symptoms. Although the cause of the low occurrence of TMD among men is still unknown, increased testosterone levels could be a likely reason (33, 23). Hormonal alterations cause unpleasant sensations among TMD patients during the menstrual cycle and pregnancy (24, 25). Myofascial pain may become more severe in women of childbearing age because of fluctuations in estrogen levels. TMJ degradation, osteoporosis and alveolar bone resorption are all due to the decreased amounts of estrogen that are present after menopause (25). A total of 92.3% of female patients with menstrual problems had TMD, according to a recent study by Jedynak et al. (26).
Joint hypermobility and hyperlaxity
TMDs and hypermobility have also been linked in research. Others have reported a favorable correlation between TMD and generalized joint hypermobility (27). Some authors have reported no association between systemic hyperlaxity and TMD or between systemic hypermobility and TMJ mobility. The possibility of TMD in patients with TMJ and systemic hypermobility was evaluated by Kavuncu et al. They reported that patients with TMD experienced both general and local hypermobility more often than did patients in control groups and that the possibility of TMJ dysfunction increased with concurrent defects (28). These findings are similar to those of a study by Coster et al. (29), which included 31 people with Ehler-Danlos disease and found that all of them had TMD with recurring condylar subluxations.
Parafunctions
Changes and compromised TMJ functions are considered TMJ parafunctions. Among these factors, excessive gum chewins, tooth clenching and bruxism have all been thoroughly studied as potential risk factors for TMD. Miyake et al. (30) identified chewing gum unilaterally and bruxism as possible elements of TMD in a study involving 3,557 students. In these studies, 87.5% of patients with joint pain and disc displacement had bruxism. The frequent abuse of the TMJ clearly causes malfunction (31), and bruxism is connected with TMD symptoms.
According to reports, 20% of adults have bruxism, which is comparable to the prevalence of this disease in young people. Cheifetz et al. (32) reported a 38% occurrence of bruxism among children in a study carried out in Boston, and the study was based on reports from parents. Only 5% of them exhibited TMD symptoms. The age group aged 20 to 50 years had the highest incidence of bruxism, after which it gradually decreased. In a 20-year longitudinal study of 420 people, Magnus- son et al. (33) reported a statistically significant association between bruxism and TMD.
Genetic predisposition
ESR1 gene and ENPP1 gene polymorphisms: Thirteen SNP genes involved in the development of TMD and surgical results in dentofacial abnormali- ties were examined by Nicot et al. The TT genotype of the ENPP1 gene SNP rs858339 (ENPP1 gene) has been shown to be a protective factor against dysfunctional degeneration following orthognathic surgery, but the AA genotype of the SNP rs1643821 (ESR1 gene) has been described as a possible element. However, patients with TMD are also at risk for those with the heterozygous genotype AT. These factors will be important in developing future screening tests, techniques, and therapies (34).
Classification of TMJ disorders and their associated diagnostic modalities
Internal derangement (ID)
ID, which denotes articular disc displacement, is the most prevalent TMD. ID has a 3:1 female-to-male ratio, increases in the 40 s to 80 s of life, and most frequently manifests as jaw pain, clicking, or locking (35, 36). Articular disc displacement is the most frequent cause of ID. The preferred imaging technique for determining ID in the TMJ is MRI (11). The situation and structure of the disc, the mandibular condyle’s signal and structure, condylar translation and the existence of joint effusion with active imaging are a few important aspects that should be assessed when interpreting MRI images of TMJ derangement.
The disc shows a typical biconcave form in the initial internal derangement, although it is displaced to the front in the closed position of the mouth. However, as the condyle moves anteriorly during mouth opening, the disc recaptures or returns to its natural anatomical location. The disc still has a normal morphology in the intermediate stage, is dislocated in the closed-mouth position, and does not recapture when the mouth opens. The articular disc is persistently displaced and develops aberrant structures in the later stages, such as perforation or broken posterior attachments to the bilaminar zone.
In more advanced stages, imaging signs of degenerative joint disease can also be visible, such as osteophytes, condyle flattening, joint effusion, or aberrant T1 and T2 signals of the condyle (37, 38,39). A different method for evaluating ID is ultrasound, specifically for detecting joint effusion and disc displacement. However, this method is thought to be less effective at identifying condyle- specific bone defects (40, 41).
Avascular necrosis
The condyle experiences avascular necrosis as a result of poor blood supply. It can be understood in relation to a variety of etiologies, including trauma, systemic lupus erythematosus and sickle cell disease. Along with severe subchondral sclerosis, the condyle of the mandible appears distorted on a CT scan. The marrow on MR exhibits a mixed signal on T2WI (T2-weighted image) and is dark on T1WI (T1-weighted image) (42).
osteoarthritis (OA)
The underlying subchondral bone and joint cartilage are both affected by OA. In older people, primary OA is more prevalent. On the other hand, younger individuals with past trauma, ID or other associated TMJ arthropathies may exhibit secondary OA (43). According to Ahmad et al. (2009), typical imaging abnormalities on MRI or CT include condyle flattening, bone erosion, osteophytes, joint space constriction, aberrant marrow signals and subchondral sclerosis (44). Pain, restricted movement, and crepitus are all indications of TMJ OA.
Rheumatoid arthritis (RA)
The most common inflammatory arthritis that can harm the TMJ in adults is RA (45). Approximately 50% of RA patients experience TMJ problems. TMJ involvement is not a typical RA finding (46). The diagnosis of RA is made in the majority of patients prior to the onset of TMJ indications. The most typical symptoms include joint swelling, pain and restricted jaw motion (47). More severe involvement may result in persistent functional loss, facial deformities, and trismus (48). Inflammatory arthritis conditions such as RA of the TMJ are frequently assessed using contrast-enhanced MRI and CT scans.
Common imaging findings associated with RA include joint space reduction, synovial proliferation, articular erosion, reduced condylar height, flattening of the condyle, abnormal condylar movement and disc deformity (45, 49, 50). In contrast to that in OA, articular disc displacement in RA occurs later in disease progression, and the disc can remain in its normal location despite significant alterations to the underlying condylar bone. The absence of bony support provided by the underlying osseous structures, rather than morphologic alterations to the disc itself, is the primary cause of disc displacement in RA patients with a lengthy history of the disease (51).
Juvenile idiopathic arthritis (JIA)
The most prevalent rheumatic condition in children and adolescents is JIA. According to the subtypes, the percentage of TMJ involvement in JIA varies, ranging from 40% to 70% (52). Because a delayed diagnosis can harm the mandibular growth plate and impair normal facial growth, early-stage diagnosis and clinical management of the TMJ in JIA-affected individuals are crucial. As patients may not exhibit symptoms until rather advanced disease stages, clinical diagnosis might be challenging (51).
The optimum imaging technique for both acute signs and subsequent degenerative arthritis is contrast-enhanced MRI. Early in the illness phase, joint effusion, synovial thickening and synovial enhancement are the prevalent typical signs. Chronic secondary arthritis alterations, such as bone erosion, pannus development, and disc degeneration, are more common when inflammation and joint damage persist (53). These changes eventually cause condylar flattening and deformity.
Septic arthritis
Despite its rarity, severe long-term disability frequently occurs in patients with TMJ septic arthritis (54). Staphylococcus aureus is the most frequently observed bacterium, and it can infect a joint through hematogenous dissemination or direct inoculation (55).
Imaging outcomes in TMJ septic arthritis patients include joint effusion, synovial enhancement, adjacent bone marrow and soft tissue edema, which are related to other joint infections. The easiest way to see these results is via MRI. The clinical appearance and severity of the indications serve as the primary criteria for differentiating septic arthritis from other inflammatory disorders. Septic arthritis is characterized by sudden onset of acute pain, excessive tenderness upon palpation, and other general symptoms, including fever, malaise, or nausea/vomiting (55).
Calcium pyrophosphate deposition disease (CPPD)
Noninfectious inflammatory arthropathy, known as CPPD, is characterized by crystal deposition in periarticular and articular soft tissues (56). Only a few case reports of CPPD of the TMJ have been published in the literature (57, 58).
Joint aspirations and fluid investigations demonstrating calcium pyrophosphate crystal deposition provide a definitive diagnosis of CPPD, but radiological assessment is crucial for determining the level of underlying osseous damage, the incidence of joint fluid, and secondary osteoarthritis to rule out other etiologies. A suitable imaging method for this illness is CT, which typically reveals a calcified form in the joint along with subsequent destructive and degenerative alterations (59). As a result, if CPPD is suspected, MRI is rarely employed as the initial imaging modality. However, as typical TMJ CPPD symptoms such as joint swelling, a reduced range of movement and pain also occur in other TMDs for which MRI is recommended as standard practice, MRI is still frequently carried out. Periarticular T2 hypointense signals with heterogeneous enhancement are notable MRI findings that can mimic more serious conditions, such as chondrosarcoma (59). Medical care and surgical joint debridement, with or without potential condyle resection, are also options for treatment (60).
Trauma
Glenoid fossa fracture, TMJ dislocation or condylar fracture can all result from trauma to the jaw. Condylar fractures make up 25-50% of mandibular fractures and are categorized as neck or condylar head (extra or intra-articular) fractures (45).
Condylar fracture patients typically experience anteromedial and inferior dislocation of the condylar head as well as telescoping and lateral displacement of the ramus due to the unrestrained force of the lateral pterygoid muscle. The preferred modality for assessing mandibular and facial fractures in acute situations is multidetector CT.
After closed reduction, the majority of condylar fractures exhibit functionally favorable results. Joint ankylosis, a fatal consequence, can arise from acute disc dislocation or damage to the retrodiscal soft tissue. Studies have revealed a connection between the likelihood of soft tissue injuries and the pattern and severity of condylar fracture on CT. However, MRI is the preferred modality for assessing disc dislocation and retrodiscal tissue injury (61, 62).
Management strategies for tmj disorders
Nonsurgical methods
Self-care methods
A TMD self-care plan might include recognizing, keeping an eye on, and avoiding oral parafunctions (such as daytime clenching, gum chewing and nail biting), tips on good sleep hygiene, pain-free eating, limiting caffeine intake, thermal therapy, self-massage, and relaxation methods such as diaphragmatic breathing and therapeutic exercises. Currently, there are not enough statistics available to state whether certain TMD diagnoses call for changes to the self-management protocol (63). These self-care techniques are crucial in addition to initial management to provide patients with some power over symptoms during recurring TMD flare-ups or bouts.
Occlusal splints
When used at night on the lower or upper teeth, stabilization splints (i.e., soft polyethylene or hard acrylic mouthguards providing full coverage of the occlusal surfaces) provide short-term relief in comparison with no treatment, but there is differing evidence compared to nonoccluding palatal splints (placebo) (64). Additionally, compared to behavioral medicine, acupuncture, physical therapy and stabilizer splints caused a similar reduction in TMD-related discomfort. Unwanted occlusal alterations have been linked to partial covering equipment such as over-the-counter mouth guards and nociceptive trigeminal inhibition (NTI) (64, 65).
Pharmacotherapy
There have been reports of the off-label use of lidocaine patches as well as neuromodulatory medications such as serotonin-norepinephrine reuptake inhibitors, tricyclic antidepressants, gabapentin, benzodiazepines, and pregabalin, particularly for managing more complex conditions, central sensitization and persistent pain (66, 67). However, the majority of the information that is currently available is focused on their use in treating other chronic pain diseases, and it is unclear how they could work specifically to treat TMD (67, 68).
Other noninvasive procedures
Physiotherapy, behavioral therapy, chiropractic care, botox injections, acupuncture, and osteopathic jaw manipulation are other noninvasive treatments for TMD (69).
Surgical procedures
Treatment of invasive closed TMJS
By simply lubricating the external joint space and enabling mobilization of the articular disc, TMJ arthrocentesis and arthroscopy have been proven to be the most efficient techniques for addressing "stuck" joints (70). TMJ arthrocentesis, however, is effective in treating acute cases of closed lock (71). Chronic (lasting more than three months) or difficult-to-treat cases of closed lock can be managed more successfully by TMJ arthroscopy. Early in the 1990s, TMJ arthrocentesis was developed as an easy and affordable method for lubricating the joint and injecting various medications directly into the superior joint area (72). Two 19-gauge needles, one acting as an entrance for irrigation fluid and medications and the other acting as an outlet to avoid fluid buildup in the joint, are used in this procedure. They are placed directly into the superior joint area. OM surgeons who would otherwise have little expertise in TMJ surgery frequently perform TMJ arthrocentesis (73).
Opening the TMJ for invasive treatment
Open TMJ surgery involves exposing the TMJ through an incision in front of the ear and is frequently referred to as arthrotomy. Arthrotomy enables a variety of surgical operations, including disc repositioning and repair (74) and discectomy, which involves removing the entire disc if it is beyond repair. Condylectomy is carried out when the condyle is also afflicted by disease, such as osteoarthritis, and if total prosthetic joint replacement is not carried out, it can result in extensive malocclusion (75).
Arthrotomy is performed when alternative treatments, including medicine and occlusal splint therapy, fail to treat a joint injury caused by trauma, degenerative disease, or inflammatory disease (76). Depending on the situation, the procedure can take anywhere from one to two hours, and tissue grafts might be needed to replace any irreparable joint parts. Patients typically spend the night in the hospital and take two weeks off to heal before returning to work. Similar to orthopedic surgery, TMJ surgery should frequently be followed by a physiotherapy and jaw exercise program (77).
Psychosocial factors and patient-centered care
Impact of psychosocial factors on tmj disorders
TMD disorders might also be hampered by anxiety. Its impact on TMD was examined, and the findings revealed that generalized anxiety disorder had a significant impact on the etiology of the condition, potentiating pain mostly due to an increase in muscular tension. An investigation into the frequency of anxiety, depression, and TMJ osseous changes in elderly Vietnamese people according to sex and place of residence, as well as the relationship between these conditions and the limitations of mandibular function, was conducted (78).
Therefore, psychological disturbance results in an increase in bodily tension, causing or exacerbating painful TMD symptomatology. This could explain why people who are always under strain, worry, and stress exhibit TMD symptoms and indicators. Teenage students have been the subject of numerous TMD studies because they are thought to be demographic and susceptible to psychological changes. According to a study by Saadet, bruxism, state anxiety, depression, and hysteria were linked to the symptoms and signs of TMD in adolescents (79).
A study by Adrian assessed the functional, physical, and psychosocial effects of TMJ degenerative joint disease (DJD) and revealed that TMJ discomfort appeared to worsen oral health- associated quality of life more than TMJ DJD severity did (80).
According to a recent study by Yadav et al., women made up 73.3% of TMD patients. Compared with male patients, female patients were more likely to exhibit bruxism. As a result, compared to male patients, female patients appeared to have a greater likelihood of TMDs. Women who had TMD indications and symptoms were shown to have higher anxiety and sadness scores. As a result, female patients with a propensity to grind their teeth and high anxiety and despair scores appeared to have more TMDs (81).
Incorporating patient preferences into treatment
Clinicians must determine whether the underlying problem is psychological or physical because this will affect the sequence of treatment (82). The group of temporomandibular diseases known as myofascial pain and dysfunction comprises the majority of psychogenic illnesses, which require the use of psychotherapy (83) and psychotropic medications (84). Treatment options that are more comfortable and appropriate for individual patients should be considered.
Cognitive-behavioral interventions for pain management
A designed regimen of cognitive behavioral therapy may be necessary if there are ingrained habits that maintain or exacerbate temporomandibular dysfunction and cannot be simply changed by increasing patient awareness. According to qualified psychologists, behavioral modification techniques may include lifestyle counseling, relaxation therapy, hypnosis, and biofeedback (85).
TMDs can occasionally be the physiological manifestation of a psychiatric or psychological condition, such as conversion disorder or depression. Indications of this possibility include the reporting of strange symptoms, the patient acting strangely, or the patient appearing to be suffering more than one would anticipate given the nature of the ailment. A psychiatric referral is a necessary component of the overall management plan in these situations (86).
Emerging trends and future directions in tmj research
Future investigations on the etiology of TMD will undoubtedly examine life stresses in greater depth, as well as uncommon genetic variations and genome-wide association studies (GWASs) (87). The study of multidimensional social and environ- mental elements has lagged behind, despite significant advancements in our understanding of the medical and psychological causes of painful TMD (88). The onset of chronic musculoskeletal pain after a car accident and the onset of spiking pain in older adults are both linked to neighborhood disadvantage, according to suggestions from the wider pain literature (89, 90). Additionally, dental pain (91), musculoskeletal pain, depression and psychosomatic symptoms (92) are related to both individual and community social capital.
TMD is included in a newly developed classification scheme for all orofacial pain syndromes. The beta version of the International Classification of Orofacial Pain (ICOP) was made public (93). The majority of the examinations and criteria specified in the ICOP for TMD, despite being a new categorization, are the same as for the validated diagnostic criteria for TMD.
Furthermore, future taxonomy will probably start to contain a more mechanistic classification because there has been some progress in our knowledge of the pathophysiology underlying TMD and other pain syndromes. This means that in addition to identifying the type of pain disorder present based on symptoms and signs, such as myalgia, the classification will also specify the mechanism causing myalgia, such as central and/or peripheral sensitization, and the molecular targets, such as CGRP or nerve growth factor, that are responsible for this particular mechanism (94). These advancements in diagnosis could explain the significant variation in prognosis and treatment response within diagnostic categories that is now found in the system. Future research will likely assist in more accurate risk prediction, therapy formulation, and administration, enabling the examination of many causative pathways (95).
Limitations
Like any other study, this study has its own limitations. Despite efforts to encompass a wide range of topics, the field of TMJ research is vast and continually evolving. It is possible that some recent developments or niche areas may not have been adequately addressed in the review. There could be bias in the selection of studies and sources, favoring more readily available or well- known research. This could result in a potential omission of relevant studies, particularly those published in less accessible journals or those not published in the English language. TMJ research spans various disciplines, including dentistry, orthopedics, rheumatology, and psychology; this review may not cover all disciplines.
Conclusion
This contemporary review provides a comprehensive overview of the multifaceted realm of temporomandibular joint (TMJ) function and dysfunction. The intricate anatomy and physiology of the TMJ emphasize the remarkable biomechanical intricacies that govern its function during everyday activities. The diverse etiological factors contributing to TMJ dysfunction and the synergistic interplay between genetic predisposition, trauma, occlusal irregularities, and psychological stress have been explored. Classifying TMJ disorders allowed us to determine the myriad clinical presentations, diagnostic criteria, and differential diagnoses, thereby facilitating accurate identification and tailored management. This review also discusses modern diagnostic modalities, underscoring their pivotal role in ensuring precise assessment.
In the realm of treatment, an array of therapeutic approaches, from conservative measures to surgical interventions, have been developed to provide comprehensive guidance for clinicians. By acknowledging the critical influence of psychosocial factors, the importance of patient-centered care and the integration of cognitive-behavioral strategies in managing TMJ-related distress has been highlighted. Furthermore, emerging trends and potential future breakthroughs in TMJ research, hinting at regenerative therapies, minimally invasive techniques, and personalized medicine, are discussed as promising avenues.
Overall, this review not only highlights the complexity of TMJ function and dysfunction but also provides clinicians, researchers, and healthcare providers with a contemporary roadmap for understanding, diagnosing, and managing TMJ-related conditions, ultimately improving the quality of life for individuals experiencing these challenges. As knowledge evolves, continued research and interdisciplinary collaboration will undoubtedly unlock new horizons for this enigmatic joint and its intricate disorders.
Author contributions statement
Conceptualization and design: V.V., K.A.R. and J.C.
Literature review: V.V.
Methodology and validation: V.V.
Formal analysis: V.V.
Investigation and data collection: V.V.
Resources: V.V.
Data analysis and interpretation: V.V. Writing-original draft preparation: V.V.
Writing-review & editing: V.V. and K.A.R.
Supervision: J.C.
Project administration: K.A.R.
Funding acquisition: K.A.R.

