











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
The knowledge of the morphology and growth of the craniofacial complex is essential to make a comprehensive orthodontic diagnosis and establish a treatment focused on the specific needs of individuals. The craniofacial complex is a set of highly differentiated anatomical components, whose development and growth occur in different ways and directions according to the individual, their genetics, and external environmental stimuli (1, 2).
The orthodontist is required to identify the direction of facial growth, as well as the facial biotype since these determine some dental, muscular, and skeletal conditions of individuals (3, 4). To obtain the diagnosis prior to the establishment of the ideal treatment plan for the care of morphological and functional malocclusions, it is required to identify the patient according to their growth direction and facial biotype, to achieve stable orthodontic results and avoid possible relapses (5).
The direction of facial growth is regulated genetically and environmentally, but there are other determining factors, so the growth of skeletal tissues is a secondary response, compensatory, and mechanically derived from the functional events that produce non-bony tissues, such as muscles or teeth (6, 7).
The direction of facial growth is related to the vertical behavior of the bony bases of the craniofacial complex, giving rise to mandibular rotation during facial growth (8, 9). Deriving in the growth of the mandible, which could suffer horizontal rotation, counterclockwise in relation to the face, forward and upward, enhancing the chin on the face, while in the vertical rotation occurs clockwise, downward, and backward providing less projection of the chin on the face, modifying the aesthetics of the patient (10, 11).
The facial biotype is a normal variation of the facial bones and muscle structures of the patients, therefore, to achieve favorable results, it is necessary to treat according to the pattern of the individual to be treated orthodontically (12). The facial biotype is classified as dolichofacial, mesofacial, and brachyfacial, these are closely related in the maxillary and mandibular morphology and, consequently, related to the shape of the dental arches and the position of the teeth (13).
The lateral cephalogram, in which cephalometric tracings are made, is a tool that provides information about the bony structures, from which the patient's craniofacial morphological characteristics are determined, including the direction of growth and facial biotype (14, 15).
Various cephalometric measurements are described in the literature to determine the direction of growth as well as the facial biotype (16, 17). Some of the authors who have proposed cephalometric analyses for the assessment of these characteristics and are routinely used by orthodontists all over the world are Ricketts and Björk-Jarabak (18). However, in some cases, the use of different cephalometric measurements to determine the same characteristic, for example, growth direction or facial biotype, could lead to an inconsistent diagnosis between the measurements applied (19, 20). It is important to distinguish the strength of agreement between the measurements of the cephalometric tracings of different authors popularly used.
The present study is aimed at studying the strength of agreement for determining the direction of growth and facial biotype in the same patient, comparing the results obtained according to two cephalometric measurement techniques widely used by orthodontists in clinical practice at a global level to distinguish the expected disagreement between each of these cephalometric measurements, and to be able to make an adequate treatment plan design based on the correct determination of the growth direction and the specific facial biotype of each patient.
Materials and methods
This observational, cross-sectional, and analytical study was approved by the institutional research committee, with registration code FODO-2017-004. A sample of lateral cephalograms of patients between 18 and 59 years of age was obtained from the radiology department of the Faculty of Dentistry. Lateral cephalograms of healthy patients, without dentofacial anomalies, with first permanent molars completely erupted, complete clinical history, and no prior orthodontic treatment were included. Cephalograms that were poorly projected or with over-impositions of anatomical structures that prevented the localization of the anatomical points were excluded, as well as cephalograms that did not project the scale rule required for digital cephalometric tracing.
The sample size was calculated for a significance level of 95% and a power of 90% with a margin of error of 5%, resulting in a required sample size of 236 lateral cephalograms. The sample was randomly selected from the postgraduate orthodontic clinic’s archives. Information on age, sex, date of birth, date of image acquisition, as well as the original digital file of the radiography was obtained from the clinical history. All included radiographs were taken in the radiology department of the Faculty of Dentistry with patients’ heads positioned with Frankfurt plane parallel to the floor by a cephalostat integrated to an Orthoceph OC200 D digital cephalometric radiographic equipment (Instrumentarium Dental Co.).
The digital image archives were stored in a computer designated for the study and were subsequently digitally traced with Dolphin Image software by a single operator, previously calibrated (n=30, 7 days difference between observations, obtaining Kappa values >0.76 and Pearson >0.94). From the digital cephalometric tracing, measurements of facial biotype and growth direction were obtained, according to each studied cephalometric analysis. The used cephalometric landmarks, measurements, and interpretation values for the determination of the studied variables are detailed in Table 1 and Figure 1.
Finally, Cohen's Kappa statistical analysis was performed to determine the concordance assessment between the results obtained from the two different cephalometric analyses studied, using MINITAB software (Minitab, Inc.). The strength of agreement was established based on the obtained Kappa values, using the original table of Landis & Koch (22) (Table 2). Additionally, Kendall's concordance coefficient was calculated and reported for comparison.
Table 1 Cephalometric measurements and interpretation values.
| Analysis | Measurement | Description | Interpretation |
|---|---|---|---|
| Facial Growth Direction | - | - | - |
| Ricketts | Vertical growth coefficient (VERT) | VERT is the sum of the patient’s discrepancy with five angles’ means. Detailed methodology is reported elsewhere (21). | Brachyfacial > 0.5 Mesofacial -0.5 - 0.5 Dolichofacial < 0.5 |
| - | - | Facial axis, formed by Pt point - Gnation (Pt-Gn) and Basion - Nasion (Ba-N) Mandibular plane, angle formed by the mandibular plane (Go-Me) and the Frankfurt plane (Porion-Orbitale) Facial angle, formed by the facial plane (N-Po) and the Frankfurt plane Height of the lower, formed by Anterior nasal spine (ANS) to Xi to Protuberantia menti (Pm) Mandibular arch, formed by Center of condyle (CC) to Xi to Pm | - |
| Björk- Jarabak | Björk-Jarabak polygon (sum of angles) | ∑ of Saddle angle + Articulare angle + Gonial angle | Brachyfacial < 390º Mesofacial 390º - 402º Dolichofacial > 402º |
| - | - | Saddle angle from Nasion (N) to Sella (S) to Articulare (Ar) Articulare angle from Sella (S) to Articulare (Ar) to Gonion (Go) Gonial angle from Articulare (Ar) to Gonion (Go) to Menton (Me) | - |
| Facial Biotype | - | - | - |
| Ricketts | Facial axis | Angle formed by Pt point - Gnation (Pt-Gn) and Basion - Nasion (Ba-N) | Clockwise (CW) <87% Neutral 87% - 93% Counterclockwise (CCW)>93% |
| Björk-Jarabak | Facial height ratio (FHR) | FHR is the proportion of PFH from AFH (FHR = PFH / AFH) | CW <59% Neutral 59% - 63% CCW >63% |
| - | - | PFH is the distance from Sella (S) to Gonion (Go) AFH Us the distance from Nasion (N) to Menton (Me) | - |
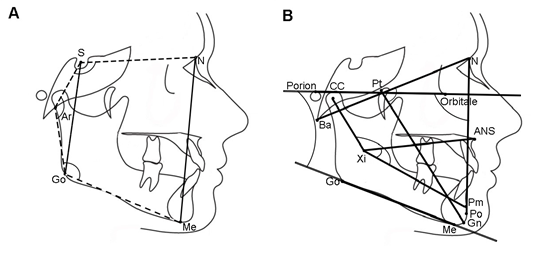
Figure 1 Cephalometric landmarks, planes, and angles for the Jarabak (A) and the Ricketts (B) analyses.
Results
A total of 260 lateral cephalograms of individuals between 18 and 59 years old were analyzed. Sixty-four percent of the sample were female (n=167) and 36% were male (n=93). The mean age was 25.1 years with a standard deviation of ± 8.5 years, a mode of 18 years, and a median of 22 years.
The distribution of the diagnostic results obtai- ned from both analyses for each facial biotype and facial growth direction are presented in Table 3.
Diagnostic Agreement
For the facial growth direction, a slight strength of agreement was found between the results obtained from the Ricketts and Björk-Jarabak analyses, and for the facial biotype, a fair strength of agreement was obtained. Additionally, the strength of agreement was evaluated for each of the diagnostic possibilities (levels), and the results are presented in Table 3.
For the facial biotype a fair strength of agreement was found between the Ricketts and Björk-Jarabak analyses, with a Kappa value of 0.326; however, the concordance increased to moderate when the diagnostic result was brachyfacial (K=0.466), or dolichofacial (K=0.442); for the mesofacial biotype the agreement remained fair (K=0.214). Kendall's coefficient of concordance was 0.79.
Regarding facial growth direction, a slight diagnostic strength of agreement was found between the Ricketts and Björk-Jarabak analyses, with a Kappa value of 0.105; however, such agreement increased to fair when the diagnosis was CCW (K=0.312), remained slight for CW (K=0.035), and decreased to poor for Neutral (K=-0.038). Kendall's concordance coefficient was 0.666.
Table 3 Strength of agreement and Kendall concordance coefficient for the facial biotype and the facial growth direction obtained by the Björk-Jarabak and Rickett analyses.
| - | Björk-Jarabak % (n) | Ricketts % (n) | Matches % (n) | Kappa | Agreement | Kendall |
|---|---|---|---|---|---|---|
| Facial biotype | - | - | 58.5 (152) | 0.362 | Fair | 0.790 |
| Brachyfacial | 21.5 (56) | 34.2 (89) | 0.466 | Moderate | - | |
| Mesofacial | 49.6 (129) | 41.2 (107) | - | 0.214 | Fair | - |
| Dolichofacial | 28.9 (75) | 24.6 (64) | - | 0.442 | Moderate | - |
| Facial growth direction | - | - | 41.5 (108) | 0.105 | Slight | 0.666 |
| CW | 15.0 (39) | 29.2 (76) | - | 0.035 | Slight | - |
| Neutral | 43.9 (114) | 44.2 (115) | - | -0.038 | Poor | - |
| CCW | 41.2 (107) | 26.6 (69) | - | 0.312 | Fair | - |
Discusion
The main objective of this study was to determine the strength of agreement of the direction of facial growth and facial biotype, assessed by Ricketts' and Jarabak's analyses, the subjects selected for the sample had complete permanent dentition and had concluded their growth stage, to avoid any type of bias in the investigation. The sample size was calculated to achieve statistical significance for the studied population.
According to the results obtained in this study, it was found that there are differences in the determination of facial growth direction and facial biotype when comparing the results of the Ricketts and Björk-Jarabak cephalometric analysis. The literature lacks information regarding this specific agreement verification for the studied characteristics. Nevertheless, some other cephalometric characteristics have been evaluated and the strength of agreement among different authors’ analyses has been reported. For example, Villanueva (2020) reported a fair strength of agreement (Kappa=0.21) when comparing the results obtained from five cephalometric analyses for the determination of skeletal class (23). Likewise, Gómez-Medina 2020, reported the strength of agreement for the determination of the protrusion and inclination of the incisors from 260 lateral cephalograms, comparing various cephalometric analyses and finding strengths of agreement between acceptable and moderate (20).
In a study published in 2017, Qamaruddin studied cephalometric values of ANB angle, Wits, Beta angle, W angle, and Yen angle, and found a significant difference between the measured values for the determination of skeletal classes (p<0.001) using an ANOVA test. And concluded that the analyses performed were equally reliable in the diagnosis of sagittal skeletal patterns since a statistically significant correlation was found between the skeletal classes of each of the studied analyses (24).
To the authors' knowledge, there is no information published specifically regarding assessing facial growth direction agreement; regarding facial biotype agreement, de Novaes (2016) reported that there is a slight strength of agreement between Jarabak's and Ricketts' measurements for facial biotypes, which partially coincide with the results of the present study; the study justifies the results with the fact that both measurements are not obtained by the same angle directly, which may result in finding different interpretations on the description of facial biotypes, and concludes that the difference in interpretation may lead to different therapeutic approaches, and, therefore, to different results in orthodontic treatment planning (16).
Herreros (2017) evaluated the concordance between different cephalometric values, relating the skeletal class values defined by Ricketts, Steiner, and McNamara, as well as the concordance between the facial biotype values by Jarabak, Steiner, and Ricketts. The percentage of agreement between Jarabak and Ricketts for the determination of facial biotype was 49.4%. The concordance was evaluated with Cohen’s kappa, and a slight strength of agreement was found in both skeletal classes and facial biotype; when comparing Ricketts and Jarabak, found a fair agreement (K=0.25), which coincides with this study’s results (19). Recently, Medina-Grandez et al. (2023) published a study about the agreement in assessing facial biotype through Björk-Jarabak analysis and photographic analysis in 244 patients and found a slight strength of agreement (K=0.02) (17).
The results of this study could help to understand that different diagnostic interpretations of facial growth direction and facial biotype could be obtained from the same patient due to the use of one or the other studied cephalometric analysis.
Conclusions
A fair diagnostic strength of agreement was found for the determination of facial biotype, and a poor one for the determination of facial growth direction between Ricketts’ and Björk-Jarabak’s cephalometric analyses in a population from Yucatan, Mexico. However, when inspecting each diagnostic possibility, the strength of agreement improved to moderate when brachyfacial facial biotype and dolichofacial facial biotype were found; likewise, it improved from poor to acceptable when determining CCW facial growth direction.
Due to the findings, cautious evaluation of the results of different cephalometric analyses applied in the same patient should be performed since it can be challenging to achieve a unanimous diagnosis, which could lead to different therapeu- tic approaches for the same patient, depending on the result obtained. However, the different cephalometric analyses have diagnostic relevance and reliability in themselves to know the main morphological characteristics of the skeletal and dental components of patients requiring orthodontic treatment, so they can be used complementary to each other to have a greater cephalometric diagnostic perspective and to be able to elaborate an orthodontic treatment plan knowing the characteristics of each individual.
Author contribution statement
Conceptualization: F.J.A.P. and G.C.R.
Methodology: D.A.P.
Formal analysis: J.R.H.A. and M.G.C.G.
Investigation: E.B.M.
Writing-original draft preparation: D.A.P. and E.B.M.
Writing-review and editing: F.J.A.P., J.R.H.A. and M.G.C.G.
Project administration: G.C.R.
Funding acquisition: J.R.H.A.
All authors have read and agreed to the published version of the manuscript.

