











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
Nursing theories represent a symbolic field of knowledge production as they have characteristics of conceptual interrelation with the observed phenomenon and relative logic.
They are articulated as proven hypotheses of practice, based on a field of technical expertise and scientific principles embedded in the social role of the profession. These hypotheses are validated through systematic and consistent research and constitute the foundation for the construction and advancement of nursing science.1 Their function is to guide the debate toward disciplinary practice through concepts and mental formulations.2
In this context, these components are essential for effective nursing practice. The significance of exploring conscious care, centered on interrelational models of individual and social care, is recognized. These models are capable of fostering a meaningful connection in the moment of care.1 This is perceived through an analysis of the assumptions defended by Jean Watson.
The Theory of Human Caring highlights the importance of a conscious and present nursing performance at the moment of care, so that the relationship established between the nurse and the patient transcends simple care. This relationship allows to create “(...) transpersonal experiences as one’s awareness of identity, or the self, as expanded beyond the singular being, with greater realizations of one’s own interconnection with humankind, life, psyche, and the cosmos”.2,3
Jean Watson considers her theory of transpersonal care to be an auxiliary and supportive tool for conscious and present nursing care, when care phenomena connect in an efficient action. This is because care extends beyond mere physical and procedural contact, reaching a deeper level that fosters a dignified and authentic relationship.1 In other words, care focuses on perceptions and actions based on trust and respect between the nurse and the patient. It implies establishing memories and feelings about the understanding of what it means to “care and be cared for”.4
The theory emerged in 1979 with the proposal of nursing care based on existentialist influences of social relationships and the integration of experiences lived by nurses and patients. Later, in 1985, the theory underwent changes with a redefinition of the concepts used, introducing transpersonal human care into the science of care. This focused on communication and the intersubjectivity of self-centered care. Since 2005, it has brought together a care plan based on interpersonal relationships through care elements called the Clinical Caritas Process, which in 2018 was renamed the Caritas-Veritas Clinical Process, representing the Science of Unitary Human Care in Nursing.5 The theory underwent a further update in 2021 and incorporated Sacred Activism as a presupposition of nursing care.6
In this case, transpersonal care consists of 10 elements related to the care process capable of identifying the correct moment to provide authentic and present care, consisting of: Embrace, Inspire, Trust, Nurture, Forgive, Deepen, Balance, Co-create, Minister and Open.5 It is essential to emphasize the need to develop specific skills for establishing a transpersonal relationship. To achieve this, teaching strategies that recognize the nursing process as an integral part of the moment of care must be incorporated, shaping the practice of conscious care. In other words, the pedagogical approach to nursing education must meaningfully and authentically address the significance of interpersonal relationships, fostering empathetic and conscious interactions between the nurse and the patient. This underscores the role of conscious care and highlights the critical importance of interpersonal relationships in nursing education.7
Carrying out this study is justified by understanding the importance of identifying the current state of transpersonal nursing care, in addition to identifying how the training scenarios of the Theory of Human Caring are constructed according to the precepts of Jean Watson. It is understood that this integrative review addresses the areas of education and care practice, as it responds to Jean Watson's concern in developing her theory with an interconnected approach between education and care.
This study aims to integrate and analyze the application of Jean Watson’s Theory of Human Caring in nursing studies with a particular focus on its implementation in care provision and educational practices within the nursing field.
The research question was: How has the Theory of Human Caring proposed by Jean Watson been used in studies published in the nursing field and education?
Methods
This is an integrative literature review guided by Whittemore and Knafl (2005).8 This method enables searching, selecting, and analyzing broader scientific productions, such as theoretical and empirical literature, to understand a given phenomenon. The steps for conducting an integrative review included: problem identification, literature search, data evaluation, data analysis, presentation. Finally, as integrative reviews do not have their own reporting guidelines, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) was used to ensure transparency in the reporting of results, as recommended in the literature.9,10
The research question to direct the first stage of the study was elaborated using the PICo strategy, consisting of: Population (scientific production of Nursing), Interest (application and approach to the Theory of Human Caring), and Context (application of the Theory of Human Caring by Jean Watson in professional, educational, and care practices).
The search was conducted in March 2023 using a search strategy developed in conjunction with a librarian. The publications were identified by searching for articles in journals indexed in the Web of Science, Pubmed/Medline, Embase, Lilacs, Scopus, and Cinahl databases using the Boolean strategy: (Nursing Theory OR Theory, Nursing OR Nursing Theories OR Theories, Nursing) AND (Models, Nursing OR Nursing Models OR Model, Nursing OR Nursing Model)
AND Jean Watson AND (Theoretical framework of nursing) OR Charitable Factors OR (Watson’s Model) OR (Watson Care Science) OR (Watson’s Science of Human Care) OR (Watson’s Science of Unified Care) AND (Watson’s Theory of Care) OR (Watson’s theory) OR (Watson’s Theory of Human Care) OR (Transpersonal Care Theory).
The established eligibility criteria included: original journal articles available in full and online, with no time restrictions, published in Portuguese, English, or Spanish; authored by at least one nurse; and exclusively employing Jean Watson's Theory of Human Caring as the theoretical framework. The following reasons were adopted as exclusion criteria: 1. publications focused on other nursing theories and which used the Theory of Human Caring only as a citation; 2. abstracts, event annals; 3. revisions; reflections; experience reports; case studies; conferences; 4. books and chapters; protocols; editorials; theses, dissertations and monographs; opinion articles; letters to the editor; errata; 5. articles published in journals considered potentially predatory; or articles not available for free.
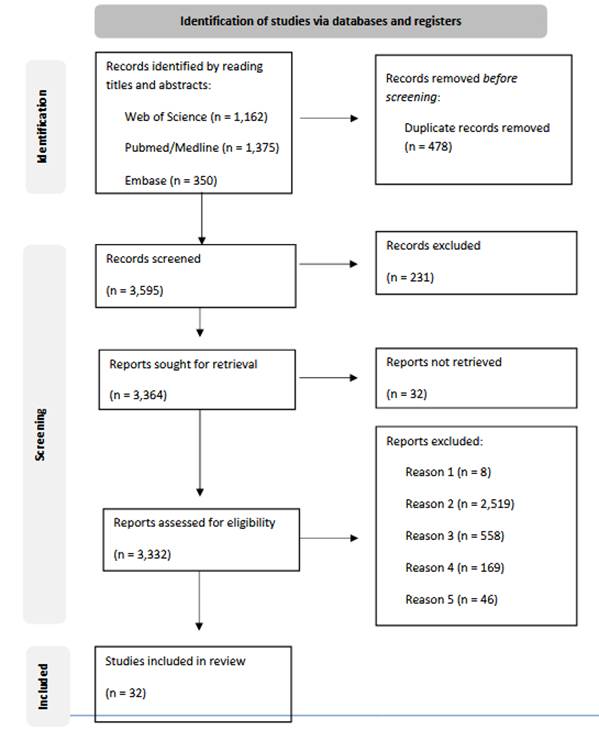
A total of 4,073 articles were initially identified in the databases. An initial reading of the titles and abstracts was carried out, and after excluding duplicates (n = 478) and those which did not meet the eligibility assessment criteria (n= 3364), a total of 32 articles were obtained to compose this review, and thus it was possible to organize the characteristics and general overviews covered in the publications presented in Figure 1.10,11
According to Whittemore and Knafl (2005), included articles underwent a data quality assessment using the Mixed Methods Assessment tool (MMAT).8,12This tool evaluates the relevance of the evidence presented in the selected studies, identifying relevance and methodological discrepancies. Three authors assessed the quality and relevance of studies, and a consensus was reached in most of them (n= 29), which obtained the maximum score. A few studies (n = 3) had inconsistencies about at least one item of the tool; however, the studies showed quality and relevance to integrate the results, so it was decided to keep all of the articles for the synthesis. The summarized table with the quality assessment based on the MMAT can be found in Table S2 (supplemental material). The findings were exported to the EndNote X9® reference manager, where they were organized and duplicates were removed. An instrument was used to collect and organize data, which considered the following criteria: author, year of publication, country of origin, journal, objective, verification of the theoretical/methodological framework, and main results. This ensured that the publications retrieved from the listed databases wereproperly recorded while also guaranteeing reliability when analyzing the information obtained. The data from each study were extracted using Microsoft Excel by an independent reviewer and subsequently verified by the primary author. The analysis stage consisted of interpreting the results through reading, descriptive synthesis, and evaluation of the relationship between each article and the proposed theme. The data was grouped and categorized using descriptive content analysis into three main themes.
As this is a review study incorporating articles available in full and accessible online, it was conducted without the need for submission to the Research Ethics Committee.
Results
The results and flowchart for identifying the studies to be included in the review can be seen in Figure 1.
Of the 32 articles included in this review, the majority are from Brazil (n = 14) and the USA (n = 10), followed by South Africa (n = 2), Saudi Arabia, Canada, Iran, Slovenia, Switzerland and Turkey (n = 1). Studies from 1995 onwards (n = 1) are identified in the temporal distribution, maintaining the trend of one publication per year until 2018, and an increase between 2019 and 2022 publications (n = 12).
The articles were published in the following journals: International Journal for Human Caring (n = 5); Revista Brasileira de Enfermagem (n = 4); followed by Revista Escola de Enfermagem da USP and Texto e Contexto Enfermagem, with (n = 2) articles each.
The majority were written in English (n = 18), followed by Portuguese (n = 13) and Spanish (n = 1). Qualitative, descriptive and exploratory studies (n = 22) stand out regarding the research method used, followed by Phenomenology (n = 3); then, randomized controlled clinical trials and descriptive survey studies with (n = 2) articles each. Correlational, qualitative-longitudinal, quantitative-qualitative, and cross-sectional methods were used in one article each. The data collection technique used was semi-structured interviews (n = 20), followed by a questionnaire (n = 11), and one article did not describe the collection technique. The most used data analysis was content analysis (n = 21), followed by comparative analysis, analysis of variance, interpretive analysis, chi-squared analysis, descriptive statistics and phenomenology stages, with one article each.
The most studied population in these articles were Nurses (n = 20), followed by the Nursing Team (Nurses, Nursing Assistants and Nursing Technicians) (n = 8), and Health Professionals (Nurses, Massage Therapists, Doctors and Physiotherapists) (n = 4). The articles that studied nurses addressed the direct work with patients (n= 21), the perception about care and self-care (n= 7), and the supervised care with the nursing and health team (n = 2). The studies that used health professionals as the sample addressed care actions in an interdisciplinary manner and care behaviors after education/training, (n = 1) article each.
Page (2020). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. 10.1136/bmj.n71
Figure 1: PRISMA flow diagram of the literature search, identification, screening, and selection. Source: PRISMA flowchart.
These characteristics enabled organizing the themes into the following categories: theme 1: Unveiling the Dimensions of Care in the Light of Jean Watson’s Ideas; theme 2: Beyond the Concept of Care; and theme 3: Care Management and Organizational Culture. The articles addressed in each category can be found in Table 1.
Theme 1: Unveiling the Dimensions of Care in the Light of Jean Watson’s Ideas
A total of twelve studies were integrated in this theme and among them, six used Caritas elements to address Nursing care, five focused on the importance of the theory in the care process, and one dealt with the care of nurses as “healers”.
In terms of the ten Caritas elements, one article addresses the perception of nurses and nursing assistants about patients’ satisfaction with the care received. These professionals exhibited significantly different perceptions regarding various factors. Notable differences were identified in sensitivity, helping relationships, expression of emotions, problem solving, teaching, environment, and spirituality, as well as in general care factors.13 A second article outlines the humanization of care for institutionalized older adults during the implementation of Caritas, with the nursing professionals perceiving the humanization of care as involving “closeness, commitment, interaction, respect, autonomy, and appreciation for older adults”. However, they suggested a lack of preparation for care in the process of death and dying among older adults.14 A third article was carried out with the health team of a pediatric ICU and semi-intensive care unit, addressing interprofessional human care, demonstrating the use of the ten Caritas/Caritas- Veritas literacy processes, and understanding that an effective interprofessional collaboration is essential.15
Another study implements the ten Caritas elements in an analysis of the care provided to children and their families in a pediatric oncology unit. It establishes a relationship with “empathy and creativity, encouragement of faith and hope in treatment, sensitivity and flexibility when dealing with the child, acceptance of the expression of feelings, investment in communication and team meetings” to reflect on the care offered.16 The implementation of the Clinical Caritas Process was also used to verify the ease and difficulties faced by nurses in carrying out transpersonal care. In terms of facilities, it is necessary to consider the patient’s individuality, scientific knowledge, the development of a relationship of trust and security, support the patient’s feelings, pay attention to tone of voice and gestures, as well as expressing respect and sensitivity. The difficulties lie in individual beliefs and the rigid norms of institutions.17 Finally, a study based on Caritas elements conducted with nurses who survived COVID-19 in their recovery and care processes shows that they experienced an increase in anxiety, fear of death and losing their relatives, and distancing from family members in order to avoid contagion. However, this distressing process strengthened the nurses.18
This theme also included six studies that deal with providing care to sick people (n = 05) and with professionals as “healers” (n = 1). The first study sought to understand how humanized care manifests itself in light of Watson’s theoretical framework. This science complements routines and tasks in conventional care, making the practice integrated, individualized, and based on human values. However, they also emphasize that teams lack awareness and appropriate references to deal with families.19 The second study, also related to the oncology unit shows that nurses emphasized that patients have different levels of well-being: their beliefs about the nature of human beings influence interpersonal encounters; respect for life and individual differences is essential; they see their role in the nurse-patient relationship as facilitators; and they deliberately attempt to create a “welcoming” environment that is beneficial from a physical, social, and psychological standpoint.20 In a third study related to providing care to people with spinal cord injuries, nurses divide care into three dimensions: care oriented towards basic human needs; care as an educational action; and attitudes and behaviors in care.21 The complexity of caring for others is also highlighted in two articles conducted in surgical units, as it is important to focus on establishing trusting relationships for care and ensuring the physical needs and the safety of patients.22 The first article highlights that when caring for patients with dementia in critical situations, nurses expressed feelings such as frustration and emotional exhaustion when experiencing the complexity of care. Care involves establishing a nurse-patient relationship to offer safe and quality care. The second article emphasizes that students need to be educated within the framework of Watson’s theory, with an emphasis on the transpersonality of caring, and nursing administrators need to engage and support the Caritas clinical model to create a caring environment for nurses.23
Finally, a phenomenological study emphasizes the importance of recognizing the sacredness of healers’ experiences and their implications for healthcare professionals, particularly nurses. It questions the extent to which these attributes are openly recognized within the nursing profession. This recognition presents an empowering opportunity for mutual learning, highlighting the inherent healer within each individual. By fostering a sense of collaboration and community in their practice, nurses can contribute to the advancement of the profession in meaningful ways.24
Theme 2: Beyond the Concept of Care
A total of nine studies were integrated into this theme; one addressed the importance of physical contact, five highlighted spirituality as an essential element in care, and three highlighted the team’s self-care.
The results of one study regarding the experience of physical contact at the end of life, carried out by professional and volunteer massage therapists, suggest the mutual benefit of physical contact. It has enhanced caregiving relationships, pattern recognition, and wholeness, as well as transformation and transcendence for people near the end of life.25 Another five articles deal with spirituality in the act of caring in the hospital environment as one of the elements proposed by Watson.
Two of the studies were conducted in a neonatal ICU and Maternity Hospital for the spiritual care of mothers of babies with malformations. In this context, nurses understand that the connection between spiritual care and the physical needs of mothers and babies is fundamental, and is manifested through faith, the belief in a greater being, God, and the dialogue between nurses and mothers.26 The encouragement of spiritual and religious practice in the general ICU was recommended for patients undergoing palliative care, seeking alternatives beyond respect for individual beliefs and offering comfort, prayers, reading the Bible and even visits from a religious leader chosen by the patient. They also focused on the lack of professional preparation for this practice.27
Two studies conducted in a general hospital with the nursing team aimed to understand spirituality in nursing care. The first study identifies spirituality as an element that promotes health in the spiritual, physical and emotional dimensions. The Systematization of Spiritual Nursing Care stands out as a timely resource, with the use of spiritual anamnesis, NANDA diagnoses, and planned and evaluated interventions that may include listening and welcoming, music, prayer, accessibility to religious leaders/practices, among other guidelines for mobilizing faith and hope in the patient and their family. They also point out the lack of training and professional preparation in this regard.28 The second study highlights spirituality in care through daily prayer before the start of the shift, addressing work overload and the complexity of care. It was mentioned that the inconsistency in praying in the daily work of the nursing team generated feelings of satisfaction (presence) and frustration (absence).29
The last study included in this theme was conducted in a geriatric center to analyze the care provided by nurses from the perspective of the spiritual dimension of care, permeated with words of encouragement related to faith, beliefs, strength, and acceptance. It highlighted the importance of prayer and participation in religious activities.30
Two of the three studies included which deal with self-care of nursing professionals were carried out in intensive care units. The first study deals with nursing caregivers in the ICU who show themselves to be human beings who present their own way of being in the world of care, with beliefs and a humanistic-altruistic value system that reveres life, love, and respect for human beings, and who have freedom of choice, which, according to Watson, constitutes a solid basis for human care. They asked for help to cope with psychological suffering in an attempt to maintain balanced and continue caring for others.31 The second study shows that attempts to maintain spirituality and provide moments for rest and relaxation are beneficial, as well as creating a vocabulary around caregiving to help with interprofessional communication.32 The last study regarding aspects of self-care was conducted in a general hospital with nursing assistants. This study describes how care for inner strengthening enables personal, professional, social, and economic fulfillment based on the communion of the “I-You”, in addition to the ability to dialogue with oneself and with others.33
Theme 3: Care Management and Organizational Culture
This category includes eleven articles discuss the supervision and provision of resources for care delivery, the perception of care and self-care among health and nursing professionals, and, finally, work management and training based on the theory of transpersonal care.
Three articles were identified which deal with care supervision and the potential for nursing leadership in managing transpersonal care, distinguishing between different moments of patient care. They highlight that there are two moments of care in the nursing process, one that takes place exclusively with the patient and another that provides the resources to perform the care. In this sense, nurses must understand how their behaviors can influence the patient’s perception of care and healing in each moment of care.34,35,36
The use of a theoretical framework or model of care can serve to guide leadership actions in clinical environments. This will likely translate into a reduction in negative behaviors, decreased absenteeism, increased employee satisfaction, and increased productivity and loyalty to the organization. Therefore, nurses must recognize the difference between managerial and caregiving.36 The management and care aspects must be constituted at different times, so that patient care has meaning and importance.34 The potential for nurse leadership permeates the subjectivity of the interpersonal care process between nurse and patient. Nurses need to develop skills in a context of leadership and care management to exert a direct positive influence on the patient. Furthermore, they need to be concerned about the repercussions on working conditions, knowing how the positive and negative results of their behaviors can directly influence the illness and recovery of patients.35
Regarding the implications when planning and organizing direct patient care, there were five articles that studied nurses and health professionals (physiotherapists, social workers and pharmacists) to understand and analyze their perceptions of care delivery, using the elements of the Theory of Human Caring for work organization and management.
For an effective care delivery, it is important to establish a relationship of trust with the patient through assertive and understanding communication. It is important to highlight that the nursing team needs to develop skills to perceive the organizational dimension of healthcare in order to promote comprehensive care, offering adequate conditions for an active and conscious care.37 Thus, the practice of quality care must permeate the paradigm of transpersonal care theory, which is centered on the authenticity and legitimacy of actions in the moment of care. To this end, attention and concentration during procedures and techniques must use elements of the theory that serve as symbolic reminders of beneficial care.38 Effective transpersonal care must be based on confidence in interdisciplinary skills. In addition, it must be based on technical and scientific knowledge before starting care practice, as the person learns to recognize themselves in others through the moment of caring by reducing work processes into objects of care.39 The nurse’s competence during the moment of transpersonal care must be evaluated based on attitudes related to the care elements. This means that care actions must be committed to the Caritas Process, as the nurse is able to influence the patient’s perception of recovery and care. Competencies involve knowledge, specific skills, and values necessary for patient care.40 Thus, care is involved in the process of teaching patients and family members, and therefore the nurse must recognize the importance of human contact, good communication, and assertiveness to impact the patient’s experience.41
Work management includes the themes of organizational climate and culture, and there were three articles that addressed the perception of care and self-care. These articles highlight the importance of the nursing team recognizing that their caring attitudes and behaviors influence the patient’s perception of care and recovery. Therefore, they suggest objectively applying the Caritas Process to promote changes in care and interpersonal relationships between nurses and patients.
The importance of the Theory of Human Caring as the responsibility for improving the quality of life at work fills gaps in knowledge about care, organizational climate and culture.42 Care guided by theory improves communication and coexistence in the nurse’s work environment. Furthermore, it benefits job satisfaction and meets the personal and mental needs of professionals, as it promotes a friendly social culture capable of organizing actions, behaviors, and work routine.43
The last article on this topic analyzes care behaviors after education and training which were modified after the workshops. Job engagement has a positive impact on organizational goals, leading to greater commitment and collaboration.44
Table 1: Summary of the articles included according to the themes identified
| AUTHOR, YEAR AND COUNTRY | DESIGN (objective, type of study, sample and collection) | MAIN RESULTS |
|---|---|---|
| THEME 1 - Unveiling the Dimensions of Care in the Light of Jean Watson’s Ideas | ||
| McNamara, 1995, United States | Determine how care is practiced in perioperative nursing. Qualitative, Descriptive. n = 6 nurses. Interview. | Ensuring physical and safety needs, incorporating existential, phenomenological and spiritual forces into care behaviors, aiming for the integrity of patients. |
| Perry, 1998, Canada | Enhance our understanding of exemplary nursing care. Qualitative, Descriptive. n = 8 nurses. Interview. | Beliefs about the definition of health and the nature of human beings are fundamental to the philosophy of nursing, influencing interpersonal encounters. |
| Hemsley et al., 2006, United States | To base a hermeneutic phenomenological study of the extraordinary and transformative experiences of healer nurses. Qualitative, Phenomenology. n = 11 nurses. Interview. | Shared awareness of transpersonal fields promotes healing. This complex experience is important for holistic nursing practice. |
| Carvalho et al., 2008, Brazil | To understand the meaning of care for Portuguese, Spanish, and Brazilian nurses who care for hospitalized people with spinal cord injuries. Analysis in the light of Jean Watson’s transpersonal care model. Qualitative, Longitudinal. n = 30 nurses, 10 Portuguese, 5 Spanish and 15 Brazilians. Interviews. | The meaning of care directs the satisfaction of basic needs within the biological field. Care is involved in meeting basic and emotional needs and is involved in actions aimed at teaching and learning activities. |
| Byers et al., 2008, United States | To record the care experiences of patients with dementia in critical (acute) care situations. Qualitative, Descriptive, Phenomenology. n = 9 nurses. Interview. | The need to be known and to know oneself in relation to others and the world is manifested in the way nurses express the need to be present, engaged, and committed to caring for patients. |
| Santos et al., 2013, Brazil | To unveil the elements of humanized care present in the encounter between nurses, families, and children with cancer; identify the perception of these nurses regarding the humanization of care and verify in which situations the nurse perceives that humanization is anchored to care. Qualitative, Descriptive. n = 9 nurses. Interview. | Being authentically present to enable and maintain a deep system of beliefs and a subjective world of self and being-for-care requires establishing a sincere relationship to build trust. |
| Santos et al., 2014, Brazil | To know the advantages and difficulties of nurses in the delivery of care for families of hospitalized children, in light of Jean Watson’s Theory of Human Caring. Qualitative, Descriptive. n = 12 nurses. Interview. | The use of the theory values the work of nurses and enables opening the self in human relationships, rescuing goodness and gentleness in an authentic and genuine way. |
| Pajnkihar et al, 2017, Slovenia | To explore the relationships between nurses’ education level, nurses’ and nursing assistants’ perception of care factors and patient satisfaction in Slovenian healthcare institutions. Transversal. n = 327 nursing assistants, 266 nurses and 475 patients. Questionnaire. | Transpersonal care is perceived differently between nurses and nursing assistants as the relationship in care, the expression of emotions, problem solving, teaching, environment, spirituality, and the overall care are significantly influenced. |
| Oliveira et al., 2018, Brazil | To reveal the nursing professional’s experience in developing care and relationships with institutionalized older adults based on adopting Jean Watson’s theory. Qualitative, Descriptive. n = 10 nurses and 14 nursing technicians. Interview. | Establishing a sincere relationship to build trust was how the worker at a Long-Term Care Facility (LTCF) for older adults exercised congruence with older adults, going beyond productive work. |
| Wei & Watson, 2019, United States | To describe interprofessional team members’ perspectives on human care based on the Ten Caritas®/Caritas-Veritas Literacy Processes of Watson’s Theory of Human Caring within the Science of Unitary Care. Qualitative, Descriptive. n = 27 nurses and doctors. Interview. | Caring relationships built between members of the interprofessional team can play a key role in creating a caring and healing environment; not only for patients, but also for others. |
| Costa et al., 2019, Brazil | To understand the care experiences of nursing professionals and to identify their relationships with the Clinical Caritas Process from Jean Watson’s Theory of Human Caring. Qualitative, Descriptive. n = 15 nurses and 11 nursing technicians. Interview. | The empathetic stance adopted by professionals, combined with creativity, may influence care, potentially causing change in an unfavorable environment in order to meet the physical, mental, and emotional needs of individuals. |
| Durgun et al., 2022, Turkey | To explain the feelings and experiences of nurses who survived COVID-19 in their care and recovery processes, based on Watson’s Theory of Human Caring. Qualitative, Descriptive. n = 15 nurses. Interviews. | Some nurses who survived COVID-19 stated that they felt fear during the disease process, lost faith and hope, and even considered leaving the profession. |
| THEME 2 - Beyond the Concept of Care | ||
| Vianna & Crossetti, 2004, Brasil | To understand how nursing caregivers perceive the care process for themselves and others in the ICU. Qualitative, Descriptive. n = 2 nurses and 6 nursing technicians. Interview. | The nursing caregiver in the ICU presents their own way of being in the world of care, having beliefs and a humanistic-altruistic value system that reveres life, love, and respect for human beings. |
| Vieira et al., 2007, Brazil | To identify perceptions and conceptions of nursing assistants at the Brasília Support Hospital regarding self-care. Qualitative, Descriptive. n = 14 nursing assistants. Questionnaire. | The integration of the mind at different levels establishes a harmonious relationship of the meaning of existence during self-care. |
| Clerico et al., 2013, United States | To examine nurses’ perception of being cared for in the hospital work environment. Quantitative, Survey. n = 324 nurses. Questionnaire. | It is important to meet the emotional and spiritual needs of patients in the healthcare environment to improve care outcomes. |
| Veras et al., 2019, Brazil | To analyze the nurse’s care in the light of the spiritual dimension of hospitalized older adults. Qualitative, Descriptive. n = 17 nurses. Interview. | Dialogue with patients is a form of care that goes beyond the dimension of words to the spiritual dimension by stimulating faith, belief, strength, and acceptance. |
| Maran et al., 2020, Brazil | To understand spirituality and the practice of euphemism experienced by nursing professionals in the hospital context. Qualitative, Descriptive. n = 18 nursing team professionals. Interview. | The spiritual dimension evokes a condition that is inseparable from the physical and mental dimension of the human being, because statements about the importance of God permeate care and not only produce benefits for the caregiver, but also for the patient. |
| Nunes et al., 2020, Brazil | To unveil spirituality in the care process of nursing professionals in the hospital context through the lens of Transpersonal Care. Qualitative, Descriptive. n = 6 nurses and 10 nursing technicians. Interview. | Spirituality as an element of health promotion is admitted to have great influence on understanding care. |
| Reed et al., 2021, United States | To explore how providers perceive the experience of physical contact in end-of-life care, with the hope that the knowledge gained can promote greater use of intentional and caring physical contact in nursing practice. Qualitative, Descriptive. n = 12 massage therapists and 7 nurses. Interview. | Pattern recognition is the set of information received from sensory, pan-dimensional consciousness that reveals a compelling sense of integrity amidst life’s variety of phenomena. |
| Viana et al., 2022, Brazil | To investigate the understanding of clinical nurses about spirituality and analyze the spiritual care provided by nurses to the mother of a baby with malformations in light of Jean Watson’s Theory. Qualitative, Descriptive. n = 11 nurses. Interview. | Nurses recognize that there is a greater conciliation with the divine through spiritual care, as it involves holding hands, listening, and talking about God. |
| Evangelista et al., 2022, Brazil | To analyze the role of nurses in assisting patients in palliative care, emphasizing the spiritual dimension, in light of the Theory of Human Caring. Qualitative, Descriptive. n = 10 nurses. Interview. | Encouragement and respect for spiritual and religious beliefs and practices are attitudes that enhance the patient’s dignity. |
| THEME 3 - Care Management and Organizational Culture | ||
| Minnaar, 2001, South Africa | To explore the meaning of caring for caregivers from the perspective of nurses and nursing managers. To determine the expectations of nursing professionals regarding the care related to nursing management. To identify common themes and practices related to care in nurse management. Qualitative, Phenomenology. n = 12 nursing managers. Interview. | Nursing management is an interactive process and therefore, emphasis was placed on relationships and interaction. |
| Nelms et al., 2011, United States | To implement a nursing unit-based intervention to decrease medication errors (MAEs) by nurses. Quanti-Quali Study. n = 13 nurses. Questionnaire. | The intervention allowed for better focus on medication, which should have led to a reduction in medications. |
| Nunes & Muniz, 2016, Brazil | To unveil the individual nurse in the leadership process for the transpersonal care of the nursing team. Qualitative, Descriptive. n = 10 nurses. Interview. | For the process of leadership in caring for others to happen, it is necessary for nurses to perceive themselves as leaders from the perspective of servant leadership which underpins this profession. |
| Olender, 2017, United States | To examine the relationship and factors that influence nurses’ perceptions of Nursing Manager Care (NMC) and perceived exposure to workplace bullying (WPB) in various healthcare settings. Descriptive correlational. n = 156 nurses. Questionnaire. | The most commonly selected nursing manager caring behavior that participants disagreed with was the item “creates a healing environment.” |
| Molala & Downing, 2020, South Africa | To understand the lived experiences of newly qualified critical care nurses caring for pediatric patients’ post-cardiothoracic surgery in a private hospital in Gauteng. Qualitative, Descriptive. n = 6 nurses. Interview. | Participants realized that caring for pediatric heart patients is completely different from caring for adult heart patients. |
| Maniago & Albougami, 2020, Saudi Arabia | To determine the competence, feasibility, importance, frequency, and satisfaction of Saudi emergency nurses in practicing care factors based on Watson’s Theory of Human Caring (1985/1988). Quantitative, Survey. n = 1,050 nurses. Questionnaire. | The elements of the Theory of Human Caring are strongly influencing factors for nursing practice and improving the level of satisfaction between nurses and patients by demonstrating the importance of spirituality. |
| King et al., 2021, United States | To assess nursing perspectives on unsupportive behaviors in the workplace and how to intervene to reduce bullying in nursing relationships. Qualitative, Descriptive. n = 139 nurses and 25 nursing assistants. Questionnaire. | It is important to improve the level of trust in care relationships, valuing leadership and assertiveness. |
| Antonini et al., 2021, Switzerland | To evaluate the medium and long-term effects on caring attitudes and behaviors on the quality of life at work in an educational intervention. Randomized controlled clinical trial. n = 72 nurses. Questionnaire. | The caring factors of sensitivity, help relationship, teaching humanism and necessity must be valued to provide opportunities for changes in caring attitudes and behaviors. |
| Elahi et al., 2021, Iran | To determine the effect of education based on the Theory of Human Caring on caring behaviors and work involvement of nurses in ICUs. Randomized clinical trial. n = 110 nurses. Questionnaire. | Workshops and training increase the behavioral level and involvement in the work of the nursing team during care. |
| Silva et al., 2022, Brazil | To analyze the production of palliative care developed by health professionals for home care patients. Qualitative, Descriptive. n = four nurses, three doctors, one speech therapist, one physiotherapist and four NTs. Interview. | It is important to develop a relationship of help and trust in care, using kindness and active listening during practice. |
| Pariseault et al., 2022, United States | To understand the perceptions and experiences of nurses caring for patients and families while facing the communication challenges mentioned above during the COVID-19 pandemic. Qualitative, Descriptive. n = 17 nurses. Interview. | It is important to maintain effective communication between patients, families, and nurses to promote positive care. |
Discussion
The discipline of nursing has an ontological advance because it has its reason for being and a practice that drives it. Additionally, technological advances in health sciences, the diversification of healthcare at all care levels, and sub- specializations pave the way for people’s quality of life in a greater health-disease continuum. Meditation also brings deeper meaning to nursing, as the transcendence of its practice spans from the foundational teachings of caring for others, to the philosophical complexity of nursing actions. It not only fosters reflection on healing but also positions the nursing process as a central component of care. In a way, nursing in its reflection returns to the existential roots of care to the need for a professional nursing-person relationship that goes beyond mere daily care. Therefore, the disciplinary trajectory bases the epistemology of care, centering it on the person cared for without neglecting the caregiver. In this sense, care is understood as a moment that requires a relationship process between two people, meaning a field of integration and union to create the care relationship.
It is clear from this review that this relationship is formed from the meetings between these two people (nurse and patient), and care would then become humanized when there is a clear consideration of the person’s life history, recognizing its complexity, its integration with the body-mind-spirit, and not just the search for physical healing in times of illness.
In humanized care, individual needs must be identified, treated with respect, and approached with adequate disposition at the time of care, because if there is support from disciplinary bases, timely and quality humanized care becomes the focus of nursing professionals.45 The nurse, as a caregiver, must meet with the patient and offer a therapeutic relationship, not just a practice of physical recovery, but an encounter between people which transcends clinical reasons.
Care has several objectives, including helping, alleviating, restoring, and promoting health, even in the absence of any diseases or conditions.46 The theoretical and conceptual development of human care has allowed it to evolve into several more integral positions such as the Theory of Human Caring, an alternative to give meaning and dignity to the field of nursing.
It is possible to define the search for knowledge of good practices dedicated to the patient and to consider their individuality, as well as to establish a relationship of trust and safety at the time of care. This means a practice that is established, understood, and perceived through sensitive interpersonal relationships and lived experiences.27
When reflecting on the actions of humanizing care and how to implement elements of Caritas elements, it is possible to correlate the practices with the awareness of self-knowledge and experimentation, which are mentioned by Jean Watson when she says that nursing care can be achieved through the body-mind-soul.28 Such reflection involves recognizing the practice from the perspective of the human being and its organic and spiritual dimensions. An article highlights the importance of developing a relationship of trust and safety to support the patient’s feelings.17 With this, the recovery of comprehensive care offers autonomy and individuality, considering the moment of care as sacred.
However, the analysis of the studies revealed the importance of the nursing team taking ownership of transpersonal care to achieve awareness of the care moment with its full strength and understanding. A study conducted in the context of the COVID-19 pandemic guides professional preparation for the moment of care, adopting an empathetic stance, maintaining in establishing interpersonal relationships, and maintaining behavior that generates favorable changes to meet the patient’s physical, mental, and emotional needs.47
From this perspective, by valuing the development of transpersonal theory skills, the nursing team identifies itself as “curators” of holistic processes, integrating physical, emotional, and psychosocial aspects during their care. This view transcends traditional, mechanistic, and task-centered practice as it emphasizes the ability to promote recovery through meaningful connections. A similar approach is evidenced in an article that analyzes the concept of healing and care in nursing; it highlighted the importance of understanding this concept to provide care to patients in therapeutic physical, emotional, and spiritual processes.48 This recognition encompasses the sacred, which attributes holistic knowledge and practices to healthcare. It is an important contribution to nursing practice, as it incorporates an inclusive approach and appreciation of the individual “who cares” during care.49
In this review, physical contact and spirituality are aspects that interact with people in care settings, as they determine compassion, sensitivity, and kindness. In particular, spirituality is an element that highlights human existence and thus, integrates the professional practice in a specific dimension.28 Encouraging spiritual and religious practice shows respect for the patient’s beliefs; it requires the use of listening, communication, and valuing silence as a bond to minimize negative feelings and emotions experienced during illness.50
It is important to train nurses on promoting spiritual care to patients and families appropriately, considering the development of self-knowledge and the reflection on the meanings of self-awareness, especially when spiritual care is part of the physical, psychological, and social needs of human beings.30,51,52
The review also points out that care requires management and attention that must constitute differentiated care actions, with a meaningful and relevant approach to patient care. Separating each moment, allows for efficient management that provides humanized and holistic resources and processes. Therefore, it is important for nurses to deliver transpersonal care, managing sufficient material and human resources to establish an active and harmonious connection with the patient. Another important aspect in managing transpersonal nursing practice is the perception of care and self-care among the nursing team.53
Nursing leaders, under a shared management practice, currently allow the nursing team to be involved in activities such as conflict resolution, decision making, strategic planning, among others, which has a positive impact on team satisfaction.54 Furthermore, when shared management is increased, it improves nurses’ empowerment and also generates healthy and ideal work environments that facilitate a more humanistic dynamic focused on developing the potential of each one. It also implies a change in management models, in the structure of a more horizontal hierarchical approach, in which levels of work commitment, structural and psychological empowerment, and job satisfaction are supported, making the workspace a place of articulation and human connection to achieve goals.55,56
By understanding these perceptions and adopting the Theory of Human Caring in nursing work management, it is possible to implement an authentic care culture and professional behavior that helps meeting the patient’s needs.57 Therefore, the importance of present and genuine nursing management is emphasized.
Transpersonal nursing education guides the development of knowledge and skills for transpersonal practice, while also fostering empathy and self-awareness as prerequisites that facilitate the experience of bodily sensations and transcendence of the merely theoretical plane. The objective of nursing educators when teaching these theories is to provide students with an understanding of practice and the essential components for practicing the art and science of the profession.58,59
Nursing care and management behaviors are important to implement nurse training spaces focused on the theory of transpersonal care. A study emphasizes the influence of the theory on the transformation of professional behaviors and the awakening to holistic, empathetic and comprehensive care in caring relationships. The authors emphasize that the theory strengthens the technical dimension of nursing care, as well as the emotional and psychosocial relationships, resulting in a more humanized nursing practice.15 The results obtained may have omitted evidence produced in the 1970s, due to the unavailability of files in digital format.
Conclusions
This review has highlighted how Jean Watson's Theory of Human Caring is applied in both nursing practice and educational proposals. It has demonstrated that the knowledge applied in practice and in educational frameworks is crucial for developing essential care skills, such as sensitivity, commitment, interaction, compassion, and empathy. These elements strengthen respect for the patient and emphasize the importance of authentic presence during care.
Spirituality emerged as a prominent theme in the studies included in this research, underscoring its role as a vital component of care. It is evident that spirituality integrates, in a disciplinary and multidimensional way, the connection between the physical and the spiritual, fostering faith. This emphasizes the need to promote the spiritual development of each nurse to better understand and address the true illnesses and needs of every individual.
Finally, transpersonal care is fundamental and must begin within the organization itself, where internal analysis enables exploring perceptions about care and promotes comprehensive care. Good leadership is needed to generate direct and positive influence on its members, and, in turn, to have a positive impact on the perception of human care that people receive through human contact and assertive communication.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to declare.

