











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
CBCT is a three-dimensional (3D) dental imaging modality which provides accurate 3D images of fine anatomical structures with high quality and spatial resolution, and has advantages such as lower cost, allowing the use of a smaller field of view (FOV), faster scanning, higher resolution, and more importantly, lower patient radiation dose compared to the computed tomography (1).
VRF refers to the fracture of root structure, along with its longitudinal axis. The prognosis of teeth with VRF depends on several factors, such as patient's age, stage of root development, the magnitude of coronal displacement of the tooth, and the gap between the broken segments. A definite diagnosis of VRF is critical to prevent unnecessary tooth extraction (2). The diagnosis of VRF often requires combined clinical and radiographic assessments, and exploratory surgery in some cases. Recently, the application of CBCT as a more accurate modality was proposed for the diagnosis of VRF (3). Materials with high density/atomic number, such as metals (as in dental implants) cause beam hardening and subsequently decrease the image contrast and cause blurring of the objects of interest and their adjacent structures on CBCT images, which are referred to as image artifacts, and can compromise correct diagnosis of VRFs (4). To minimize the adverse effects of artifacts on diagnostic accuracy, CBCT exposure parameters may be changed or a metal artifact reduction (MAR) algorithm may be applied (4).
This study sought to evaluate the impact of the MAR algorithm and tooth-implant distance on the diagnostic accuracy of CBCT for the detection of VRF in teeth adjacent to dental implants because tooth-implant distance significantly affects the diagnostic accuracy of VRFs and there are a few studies on this subject.
Materials and methods
This in vitro experimental study was conduc- ted on 20 extracted single-canal human anterior and premolar teeth. The study was approved by the ethics committee of Hamadan University of Medical Sciences (IR.UMSHA.REC.1400.383). Absence of fracture confirmed with a magnifying glass and periapical image, and teeth with internal and external resorption and calcification were excluded from the studyto prevent bias related to crown fracture. They were decoronated at the cement enamel junction with disk. The root canal therapy was done by Pro-taper Universal rotary system, and the working length considered 1mm less than the end of the radiographic apex. At each stage, the Canal was washed using a 23-gauge syringe with sufficient pressure and normal saline solution.
Obturation was performed by cold lateral conden- sation method using Guttapercha and resin sealer (META, Chungcheongbuk-do, Korea).Then roots were randomly assigned to two groups (n=10). In group 1, universal testing machine was used to induce a VRF in roots at a speed of 1mm/minute. When the pressure on the teeth was decreased by 20%, the teeth came out from the device(A 20% drop in pressure was indicative a fracture) (Figure 1).The roots remained intact in group 2 (control group). After that, implant hole was drilled at the right second premolar site by a surgical drill for placement of a nickel-titanium implant, and two teeth were randomly selected (both roots can be with fracture or without fracture or one with fracture and the other one without fracture) and mounted in the extraction sockets of right canine (with 20mm distance from the implant) and right first premolar (with 9mm distance from the implant) in the dry human mandible (Figure 2). The roots were then mounted in a sound dry human mandible by melted wax, and the dry mandible was inserted in water in a clear plastic container to simulate beam attenuation by water. CBCT was performed using Kodak 9600 3D CBCT scanner with 8x5cm FOV, 75µm voxel size,8mA, 60 kVp, and 6.1 s time once using MAR algorithm and once without it. Then, the location of the tooth roots was switched, and the dry mandible underwent another CBCT once with the application of MAR algorithm and once without it (Figure 3).

Figure 1 A. Universal testing machine usedto induce VRF in roots. B. Arrow: VRF in the lingual aspect of the root.
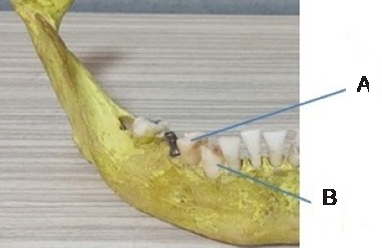
Figure 2 Disposition of the dental implant and roots in the dry human mandible. A. Close distance. B. Far distance.
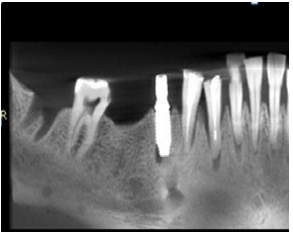
Figure 3 CBCT images for evaluation of VRF in right canine and right first premolar. A. Axial view. B. Panoramicreformat.
One radiologist and one postgraduate student of oral and maxillofacial radiology evaluated the images under similar conditions (in a semi-dark room using OnDemand3D software) in a double- blind manner, and filled out a checklist regarding presence/absence of VRFs. After 7 days, the images were assessed again under the same conditions. Based on provided checklist, both observers recorded their opinion regarding the presence/absence of VRF in teeth in the following four scenarios:
First scenario: Close distance between tooth and implant without MAR algorithm.
Second scenario: Far distance between tooth and implant without MAR algorithm.
Third scenario: Close distance between tooth and implant with MAR algorithm.
Fourth scenario: Far distance between tooth and implant with MAR algorithm.
The diagnostic sensitivity and specificity values were computed independently for each observer and for each procedure, and the receiver operating characteristic (ROC) curve was created for comparison with the standard values. Intraclass correlation coefficient (ICC) was calculated to assess the inter-observer and intra-observer agreements. All statistical analyses were carried out using SPSS version 21 at 5% level of significance.
Results
Table 1 presents the diagnostic sensitivity, specificity, accuracy and positive predictive value for two observers in their first observation for different scenarios.
As shown in Table 1, in close distance without MAR, the first and the second observers correctly detected the roots with VRFs in 50% and 70% of cases, respectively. Furthermore, the first and the second observers correctly detected the roots without VRFs in 90% and 80% of the cases, respectively.
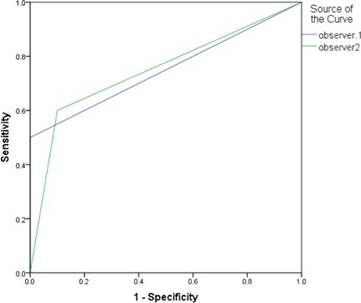
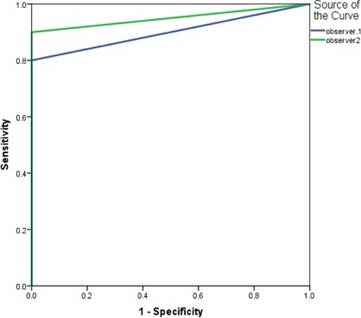
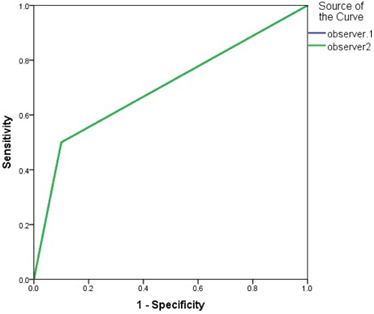
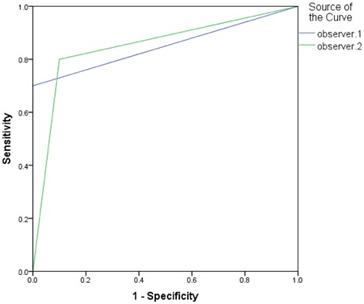
Figure 4 to Figure 7 show the ROC curve regarding the performance of two observers in detection of VRFs in the four scenarios in their first observation.
The maximum area under the curve (AUC) for the first and second observers was recorded in the second scenario, which was 0.9 and 1.00, respectively.
Table 2 presents the diagnostic sensitivity, specificity, accuracy and positive predictive value for the two observers in their second observation separately for each scenario.
Table 1 Diagnostic sensitivity, specificity, accuracy and positive predictive value (in percentage) for the two observers in their first observation for different scenarios.
| Scenario | Observer | Sensitivity (%) | Specificity (%) | Accuracy (%) | Positive predictive value (%) |
|---|---|---|---|---|---|
| Close distance without MAR | First | 50 | 90 | 70 | 83 |
| - | Second | 70 | 80 | 75 | 78 |
| Far distance without MAR | First | 80 | 100 | 90 | 100 |
| - | Second | 100 | 100 | 100 | 100 |
| Close distance with MAR | First | 70 | 80 | 75 | 78 |
| - | Second | 40 | 90 | 65 | 80 |
| Far distance With MAR | First | 70 | 100 | 85 | 100 |
| - | Second | 80 | 80 | 80 | 80 |
Sensitivity: The proportion of samples that are genuinely positive and provide a positive result using the test in question. Specificity: The proportion of samples that are genuinely negative and provide a negative result using the test in question. Accuracy: The proportion of true positive results (both true positive and true negative)in the selected population.
Positive predictive value: The probability that a sample returns a positive result is positive.

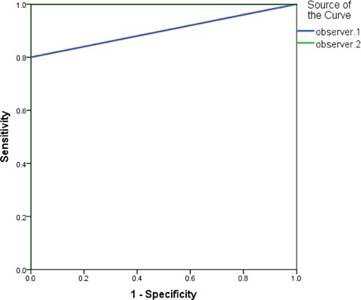
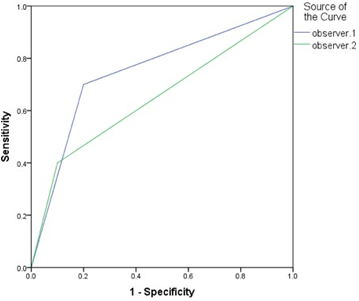
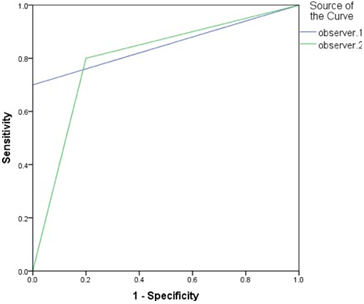
Table 2 Diagnostic sensitivity, specificity, accuracy and positive predictive value for the two observers in their second observation separately for each scenario.
| Scenario | Observer | Sensitivity (%) | Specificity (%) | Accuracy (%) | Positive predictive value (%) |
|---|---|---|---|---|---|
| Close distance without MAR | First | 50 | 100 | 75 | 100 |
| - | Second | 60 | 90 | 75 | 86 |
| Far distance without MAR | First | 80 | 100 | 90 | 100 |
| - | Second | 90 | 100 | 95 | 100 |
| Close distance with MAR | First | 50 | 90 | 70 | 83 |
| - | Second | 50 | 90 | 70 | 83 |
| Far distance with MAR | First | 70 | 100 | 85 | 100 |
| - | Second | 70 | 100 | 85 | 100 |
As shown in Table 2, in close distances without MAR, the first and the second observers correctly detected the roots with VRFs in 50% and 60% of the cases, respectively. Moreover, the first and the second observers correctly detected the roots without VRFs in 100% and 90% of the cases, respectively.
Figure 8 to Figure 11 show ROC curve regarding the performance of two observers in detection of VRFs in the four scenarios in their second observation.
The maximum AUC for the first and second observers was recorded in the second scenario, and was 0.90 and 0.95, respectively.
Table 3 presents the kappa values for intra-observer agreement of each observer for each scenario.
The highest agreement between the first and second observations for the first and second observers was in the second scenario, in an amount of 100% and 90%, respectively.
Discussion
Partial or complete longitudinal root fractu- res known as VRFs often call for tooth extraction (5,6). VRFs may be difficult to diagnose, and early identification is crucial to stop further bone loss by adopting preventative action (6). Although peria- pical radiography is often the first choice for the detection of VRFs, it may lead to misdiagnosis since it provides 2D images and causes image distortion and superimposition of anatomical structures. By the provision of 3D images, CBCT eliminates the superimposition of anatomical structures to a great extent, and minimizes distortion, resulting in higher diagnostic accuracy than periapical radiography for detection of VRFs (7). Nonetheless, the quality of CBCT images often decreases in terms of the presence of metals, such as dental implants and compromises correct diagnosis in areas adjacent to metal objects. To minimize the effects of artifacts on diagnostic accuracy, CBCT exposure parameters can be altered or MAR algorithm can be applied (8). According to the results, in close tooth-implant distance, the diagnostic sensitivity (detection of teeth with VRF) and the specificity roots without VRF were lower in the application of MAR algorithm, compared with no MAR. In distant position, the sensitivity and the specificity was lower in application of MAR compared with no MAR. Furthermore, the maximum AUC in both the first and second observations for both observers was recorded in the second scenario (distant position, no MAR), indicating that the second scenario had the highest diagnostic accuracy.
The highest diagnostic accuracy for both observers was noted in far distance without MAR, and the lowest diagnostic accuracy for both observers was noted in the close tooth-implant distance, without MAR for the first observer and with MAR for the second observer. This result can probably be explained by the beam hardening phenomenon, which is the increase in X-ray beams with moderate energy levels as a result of low-energy photons being absorbed by the objects rather than high-energy photons, which results in artifacts generated by the implant material that mask the fracture line or streaks that resemble VRF and produce false positive results (9). MAR algorithm is used to decrease the artifacts of the final image and increase its diagnostic accuracy. Nonetheless, the present results showed that applying MAR decreased the diagnostic accuracy, sensitivity, and specificity value for the detection of VRFs on CBCT scans, compared with no use of MAR algorithm. In general, the diagnostic accuracy in distant position was higher than that in the close tooth-implant distance, and in both scenarios, the diagnostic accuracy without MAR was higher than that with MAR (except for the first observation by the first observer, where, the diagnostic accuracy in the close distance was higher in the presence of MAR, compared with absence of MAR).
According to Nikneshan et al. (10) the diagnostic sensitivity and specificity without MAR were higher than the values in the presence of MAR (10). Oliveira et al. (11) concluded that application of MAR had a negative effect on the detection of VRF in teeth without root canal filling, and in teeth with gutta-percha root filling material, and metal posts. De Rezende Barbosa et al. (12) reported that applying MAR did not improve the diagnosis of VRFs. Moreover, they added that the diagnostic accuracy was lower for teeth with cast pins, irrespective of applying MAR algorithm. Similarly, Bechara et al. (13) and Bezerra et al. (14) showed that application of MAR algorithm decrea- sed image artifacts but had no positive effect on diagnostic specificity and accuracy of detection of VRFs. In a research by Dalili Kajan et al. (15) the specificity of CBCT images with MAR was lower than CBCT images without MAR, results showed that the sensitivity of images with MAR for detec- tion of VRFs in the presence of posts and pins was greater than the sensitivity of images without MAR. In a study by Fontenele et al. the ROC curve and sensitivity values were not significantly different in different tube currents, irrespective of presence/ absence of implant and MAR algorithm. The specificity values were not significantly different among multiple tube currents; however, the specificity was significantly different in presence and absence of dental implant, and it was lower in presence of dental implants (4). The present results revealed that application of MAR decreased sensitivity, specificity and diagnostic accuracy in close and distant scenarios compared to the absence of MAR. Moreover, the diagnostic accuracy, sensiti- vity, and specificity in distant scenario were higher than the corresponding values in the close tooth- implant distance.
Saati et al. (16) and Freitas et al. (17) showed that generated artifacts mimicked the fracture pattern, and caused a false positive result, also the application of MAR improved specificity and diagnosis of VRFs (16,17).
CBCT scanners use specific image reconstruction algorithms that affect image quality and enhance diagnosis. Nonetheless, adjustable parameters, such as FOV and voxel size have significant effects on the final image. Although there is little information available about CBCT manufacturers and the way MAR algorithms work, it is assumed that they are engaged in response to a certain threshold. The gray values of very hypodense or hyperdense streaks of high-density materials like gutta-percha and metal items (like dental implants) are modified, allowing for a more precise identification of any structure that deviates from the gray value threshold (18).The fracture line and dentin density were almost the same when using MAR algorithm, which is the most probable explanation for the reduction in diagnostic accuracy in the use of MAR.
For the detection of VRFs, the image quality should be high enough to reconstruct the hypodense fracture line in contrast to the adjacent structures. CBCT image quality is affected by a number of different factors, such as FOV (a large FOV has lower contrast and spatial resolution than a small FOV), voxel size, signal/noise ratio, contrast, spatial resolution, scattering, artifacts, detector quality, and image reconstruction algorithms (11). Voltage (kVP) is among the most influential parameters on artifact generation, probably because it is responsible for the energy level of photons. Theoretically, higher voltage levels translate to higher mean energy levels of photons, which are less filtered by metal objects and result in less artifact generation (16). Therefore, selecting different parameters like voltage in different studies can affect the final results. Aside from different parameters, the type of implant alloy, the type of CBCT scanner, and factors like bone density can affect the severity of artifacts, irrespective of the type of dental implant alloy (19). Panjnoush et al. (20) evaluated the effect of exposure parameters on the amount of metal artifacts generated by different CBCT scanners, and concluded that increasing the voltage decreased the metal artifacts.
Although MAR algorithm can increase image quality by noise reduction around dental materials on images, it does not necessarily have a positive effect on diagnostic accuracy (21). It was reported that MAR algorithm may effectively enhance the diagnosis of VRFs when artifacts are generated in an area other than the site of respective tooth, especially because it does not interfere with the amount of beams received by the patient. Moreo- ver, MAR algorithms have different performances depending on the type of scanner, FOV, and material properties (22,23), which can explain the difference between the results of Saati et al. (16) and Freitas et al. (17) with the present findings.
Conclusion
The current findings showed that the MAR algorithm's use had no beneficial influence on the CBCT's diagnostic precision for detecting VRF in teeth both close and distant from a dental implant. In general, instances distant from the implant have a more accurate diagnosis than those close to the implant.
Suggestions
Future studies are required to assess the effect of different materials simulating the effect of soft tissue on quality of CBCT images to better simulate the clinical setting under in vitro conditions.
Author contribution statement
Conceptualization and design: F.S. and Z. M.
Literature review: Z.M. and V.H.
Methodology and validation: Z.M. and M.F.
Formal analysis: M.F.
Research and data collection: Z.M. and H.V.
Resources: F.S. and M.F.
Data analysis and interpretation: Z.M., M.F. and H.V.
Writing-preparation of the original draft: Z.M.
Writing: proofreading and editing: Z.M. and F.S.
Supervision: F.S.
Project administration: F.S. and Z.M.
Acquisition of funds: Self-financed

