











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
According to the FIFA Women’s Football Member Associations Survey Report of 2019, it was estimated that ~13.36 million girls and women are playing soccer worldwide; with 3.12 million registered youth players (<18 yrs.) and ~1 million registered adult female players (18+ yrs.) (FIFA, 2019). Female soccer is also prominently played at the collegiate level in the United States, with more than 1,500 colleges supporting a women’s soccer program, spanning across 5 division levels: National Collegiate Athletic Association (NCAA) Division 1, D2, D3, the National Association of Intercollegiate Athletics (NAIA), and the National Junior College Athletic Association.
The intensity of soccer combined with the cardiovascular, agility, and muscular components are collectively sufficient to elevate metabolic heat production and core body temperature (Edwards & Clark, 2006). This inevitable increase in core temperature leads to an increase in sweat rate to help diminish excess heat. Maughan et al. (2004), found that the average sweat rate of a soccer player can range from 1-3L per game. Considering that the predominant component of sweat is water from circulating plasma volume, unless players replace the fluid in which is lost, they risk experiencing net loss of body water (Edwards & Noakes, 2009). Continuous, un-altered, net loss of fluid negatively influences circulating plasma volume, and can lead to dehydration.
Dehydration refers to the physiological process of losing body water, ≥2% of body weight (Murray, 2007), whereas hypohydration refers to the uncompensated loss of body water. Hypohydration can be considered mild, moderate, or severe. Being in a state of dehydration is representative of homeostatic imbalance. Dehydration can have numerous adverse effects on the human body, for example cardiovascular strain and drift (Maughan, 2003). Furthermore, players in a state of dehydration can experience specific sport performance impairments. A seminal study by Montain & Coyle found that increases in heart rate and core temperature were proportional to the extent of dehydration (Montain & Coyle, 1992). Exercising in a state of dehydration has also been shown to affect fuel utilization (Logan-Sprenger et al., 2012) and musculoskeletal performance (Rothenberg & Panagos, 2008). Extreme cases of dehydration can also exacerbate the risk of exertional heat illnesses such as muscular cramps, heat syncope, heat exhaustion and heat stroke.
Considering the negative impact of both dehydration and hypohydration on performance, monitoring and ensuring an athlete’s hydration status may be paramount to sporting success. Monitoring hydration can be done in both field and laboratory settings through varying techniques. Some more precise monitoring techniques often require expensive and stationary devices such as measuring Urine Osmolality (Uosm), Plasma Osmolality (Posm), and Isotope Dilution; most of which are not practical for field use. Methods better suited for field measures include measuring Urine Specific Gravity (Usg), observing Urine Color (UC) and changes in body mass. Usg is a measurement of hydration based upon the concentration or density of urine, and is recognized to be a reliable and practical method for assessing hydration status (McDermott et al., 2017). Cut-off values for fluid replacement were included in the National Athletic Trainers’ Association (NATA) Position Statement, a Usg of <1.010 indicates euhydration; 1.010 - 1.020 indicates minimal hypohydration; 1.021 - 1.030 indicates significant hypohydration; and >1.030 indicates serious hypohydration (Casa et al., 2000).
Previous studies have shown that despite the plethora of knowledge highlighting the impairments caused by inadequate hydration, hypohydration is still highly prevalent across all levels of soccer. For example, Phillips et al. (2014) monitored the hydration status via Usg of 14 elite male soccer players over 3 consecutive days and found that 77% of players attended practice already in a dehydrated state on day 1 and 3, and 62% on day 2 (Phillips et al., 2014). Fewer studies exist however looking specifically at female soccer players. Castro-Sepulveda et al. (2016) tracked the hydration status of 17 elite female soccer players before three varying events: training (PT), friendly match (PF), and an official game (PO). It was found that dehydration was prevalent prior to every event (Usg levels: PT = 1.029; PF = 1.023; PO = 1.030) and that an average of 47.05% of players were seriously dehydrated (Usg >1.030) (Castro-Sepulveda et al., 2016). Additionally, Gibson et al. (2012) found comparable results after monitoring the hydration status of 34 elite female Canadian soccer players before 2 non-consecutive training sessions. Over both sessions it was found that 45.4% of players presented to training in a dehydrated state (Usg >1.020); 40.9% were significantly dehydrated (Usg 1.020-1.029); and 4.5% were seriously dehydrated (Usg >1.030) (Gibson et al., 2012).
Despite evidence supporting the prevalence of hypohydration in soccer players, to our knowledge most literature reports monitoring hydration status only over an acute period of time. Hydration status fluctuates daily due to numerous factors such as diet, environment, and female menstrual phase; therefore, whether it can be claimed that acute hydration status is reflective of more habitual hydration status is arguable. Therefore, the primary aim of this study was to monitor the hydration status of female collegiate soccer players over a 2-week period; inclusive of training sessions, games and rest days.
Materials and Methods
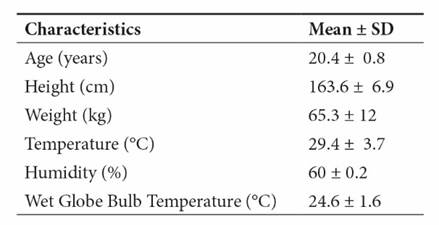
Sixteen collegiate female soccer players were evaluated (age: 20.4 ± 0.8 years; body height: 163.6 ± 6.9 cm; body mass: 65.3 ± 12 kg) during this study. Coaches, staff, and players were informed of the purpose and procedures of the study. In addition, an explanation of the potential benefits and risks were given to the study participants. The experimental protocol was approved by the Auburn University at Montgomery Institutional Review Board (#2016-066). Those players who voluntarily gave informed consent to participate also completed a health history questionnaire.
Experimental Protocol
Data were collected over a 2-week period during a regular National Association of Intercollegiate Athletics (NAIA) women’s soccer season. Participants were asked to collect two urine samples per day. Urine specimens were collected from each player in the morning (AM) and evening approximately one hour before pre-practice or game (PM). Each sample were collected by the player in a sterilized, pre-sealed container distributed the day prior. Urine was used to evaluate the hydration status via the use of urine specific gravity (Usg), and hydration status was classified based on cut-off values recommended by NATA position statement on fluid replacement for players (Casa et al., 2000). Samples were collected Monday through Friday; weekend samples were not required for this study. In total, over the period of 2 weeks, 9 days’ worth of urine samples were collected and analyzed for hydrational status. Additionally, environmental variables were monitored prior to every PM practice/game, but were not controlled for in our study. Temperatures (oC), humidity (%), and Wet Bulb Globe Temperatures (WBGTs) over the course of the study were 29.4 ± 3.7oC, 60 ± 0.2%, and 24.6 ± 1.6oC, which were not controlled for in our study.
Training and Dietary Standardization
Samples were collected at the same time each day (±1 hour). Players were asked to continue with normal daily habits and to sustain normal dietary and fluid intakes. Players were also asked to continue with training as they normally would. No recommendations or results were given to players regarding fluid intake or hydration status to ensure players were not influenced by outcomes, and that data collection was conducted under normal, “real-life” conditions. Players currently taking prescription medicine or supplementation were asked to report this on their health history questionnaire.
Hydration Status
Participants were asked to collect a mid-stream urine sample in a sterile, 4 oz. specimen cup (Dynarex no. 4254, Dynarex, Orangeburg, NY, USA), to ensure a clean sample for later assessment. Daily samples were collected by the investigator each PM. Samples were analyzed within 24 hours. This method is supported by Adams and et al. (2017) who found that urinary hydration markers were stable 1-2 days after collection, with no change in Usg.
Urine analysis was done using a portable, handheld clinical refractometer (PEN-Urine S.G.; ATAGO Co, Tokyo, Japan) which was calibrated as per manufacturer’s instructions using distilled water. Refractometry is a practical method of identifying urine density through emitting a beam of light through the sample. Each urine sample was measured in duplicate by the same researcher. If measurements varied by >0.0010, a third measurement was taken, and an average was determined. Hydration status was determined by using the measured Usg values in reference to cut-off values reported by Casa et al. (2000).
Statistical Analysis
Acquired data were analyzed using SPSS (v. 23, IMB SPSS Statistics, Chicago, IL, USA) and SAS University Edition (SAS Institute, Cary, NC, USA). We performed estimation and statistical inference for a general linear mixed model with restricted maximum likelihood in SAS (PROC GLIMMIX). Fixed effects included time of day (TOD; AM vs. PM), and day of study (1-9), along with their interaction.
The percentage of players who were euhydrated, minimally, significantly, or seriously hypohydrated, on each day and time point, were calculated using total number of samples of that respective time and day, and the pre-determined cut-off values. All data are reported as means ± standard deviations (SD), and significance was accepted as p<0.05.
Results
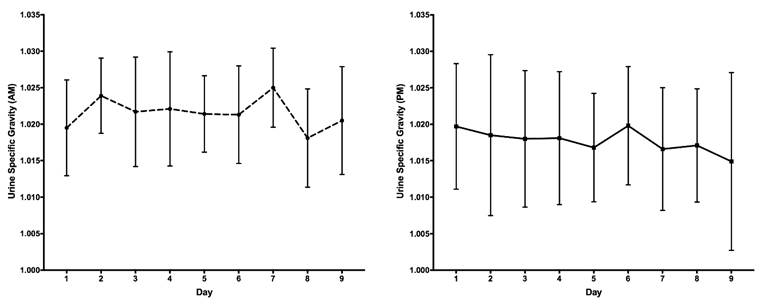
The player’s characteristics and environmental conditions are reported in Table 1. The general linear mixed model showed a significant difference between AM and PM Usg values (F(1,250) = 23.09; p < 0.0001), with a higher mean Usg in the AM (1.021 ± 0.007) vs. PM (1.018 ± 0.009). The average difference between AM and PM Usg values was -0.0038. Daily AM and PM mean Usg values throughout the course of the study are displayed in Figure 1. There was no significant difference found between days (F(15,250) = 1.98; p>0.05), and no time of day*day interaction (F(14,250) = 2.17; p>0.05).
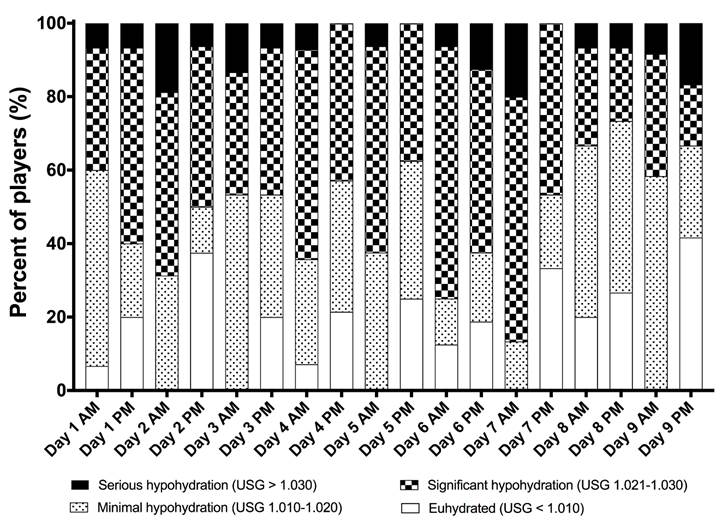
During the study, 100% of player’s AM and PM Usg over the 9 days indicated a hydration status of “minimal” hypohydration or worse (Usg >1.010). Furthermore, on every day and time point, ≥ 58% of players were either “minimally” hypohydrated or worse (Usg>1.010). At least two of the days the player’s hydration status were in the “significant” or “serious” hypohydration state (Usg >1.021). Day 6, sixty-five percent of players PM Usg were in the “significant” or “serious” hypohydration state. Day 7, eighty-seven percent of players AM Usg were in the “significant” or “serious” hypohydration state.
In contrast, our study indicates that the percentage of players that presented in the euhydrated state (Usg ˂ 1.010) in the AM and PM were less than 40% over the 9 days. The highest percentage of players presenting the euhydrated state occurred on Day 8 in the AM (20%) and Day 9 in the PM (42%). Day 1 PM and Day 2 PM, only 20% and 25% of players presented themselves in a euhydrated state to play, respectively. Daily AM and PM percent of total players within each hydration classification is displayed in Figure 2.
Discussion
This study investigated the incidence of hypohydration in female collegiate soccer players over a 2-week period. Hydration status was assessed upon waking (AM) and prior to practice and official games (PM). The findings of this study highlight that a large proportion of players both awoke and presented to practice or games in a hypohydrated state. This high prevalence of hypohydration is a cause for concern considering the impact sub-optimal hydration has been found to have on sports performance. Research has shown that hypohydration can impact physiological and skill related components of soccer performance. McGregor et al. (1999) evaluated the effect of fluid ingestion on performance of soccer skills. Following a 90-minute Loughborough Intermittent Shuttle Test (LIST), players completed a soccer skill and mental concentration test. It was found that without fluid ingestion, soccer skill performance deteriorated by 5%. Furthermore, data shows that on 5 of the 9 days reported, 100% of players awoke (AM) in a state of hypohydration (Usg >1.010), 2 of which were official game days. Additionally, every day, ≥58% of female soccer players woke (AM) and presented to practice or game in a sub-optimal state of hydration (Usg >1.010). The highest daily incidence of “significant” or worse hypohydration (Usg >1.021) in the AM and PM was 87% on Day 7 and 63% on Day 6, respectively. Furthermore, mean Usg values were significantly higher in the AM vs. PM, with an average difference between time points of -0.0038. This average decrease in Usg between AM and PM could be indicative of players attempting to compensate for their poor morning hydration state before practice or games in the PM.
The high incidence of hypohydration in female collegiate soccer players found in our study is similar to that seen in other literature. Chapelle et al.(2017) found comparable results after monitoring the hydration status of 18 female soccer players over the course of an 8-day tournament. Urine was utilized to measure hydration, and similar cut-off values were used to determine the classification of hydration status. On days 1 to 4, the percent of players who were minimally hypohydrated (Usg >1.010) ranged between 44-78%. On the 5th and final day, all players were also minimally or hypohydrated. Furthermore, similar to our findings, a negative correlation was found between fluid intake and Usg values (Chapelle et al., 2017). In addition to this, a study conducted by Castro-Sepulveda also found after observing 17 elite female soccer players that on average only 2% of players attended training, friendly, or official matches in a euhydrated state; indicating that 98% of players presented to events already in a state of hypohydration (Castro-Sepulveda et al., 2016). Similarly, our study and Castro’s study (Castro-Sepulveda et al., 2016) were conducted in a field setting, with comparable temperatures (29.4oC vs 29oC). Hydration assessment was also analogous in that both studies used Usg to determine hydration status in accordance to the same cut-off classification values.
Although the prevalence of athlete hypohydration in soccer players is evident, literature would further suggest that inadequate hydration is not limited to one sport over another. A large study conducted by Volpe et al. (2009) monitored the pre-practice hydration status of 263 NCAA D1 college athletes (male n = 138; female n = 125) representing 14 college sports. Using Usg to assess hydration, it was found that 13% of athletes were significantly hypohydrated; 53% appeared hypohydrated; and only 34% were suitably euhydrated (Volpe et al., 2009). Furthermore, a study conducted by Osterberg and et al. (2009) monitored the hydration status of 29 professional National Basketball Association players before 2 games over a 4-day period. Alarmingly, despite this population representing the epitome of elite in basketball, it was found that 52% of players presented to games in a hypohydrated state (Usg >1.020) (Osterberg et al., 2009). All in all, it would be erroneous to state that hydration is not a cause for concern or that there is little need for further monitoring considering the evidential prevalence of hypohydration in varying sports, skill level and ages.
The use of Usg for measuring hydration status has been widely utilized in the field due to its portability, ease of use and cost-effectiveness in comparison to other more laboratory-based methodologies. Cut-off values and classifications for Usg derived measurements however can be inconsistent in the literature. The seemingly general consensus, as outlined by the American College of Sports Medicine, is that a Usg value of ≥1.020 is indicative of being in a hypohydrated state (Sawka et al., 2007). However, this singular cut-off value is not the only classification method utilized in hydrational research practices. In the NATA position statement regarding fluid replacement for athletes, several cut-off values are identified to help define hydration status: euhydrated <1.010; minimally hypohydrated 1.010-1.020; significant hypohydration 1.021-1.030; and, serious hypohydration >1.030 (Casa et al., 2000). The use of these more specific cut-off values has been similarly utilized in other research studies (Chapelle et al., 2017; Kilding et al., 2009).
One novel finding of this study is that players were observed over a longer period of time (2-weeks; 9 days of data collection) in comparison to previous studies. This represented habitual, day-to-day hydration behaviors as opposed to acute behaviors. Players were also observed in the field and were asked to continue with normal daily habits, including physical activity, and to sustain normal dietary and fluid intakes. This ensured that players were not influenced or tempted to change habitual drinking habits throughout this study. Furthermore, hydration was assessed at 2 time points, in both the morning (AM) and pre-practice/game (PM). This allowed for us to assess whether or not players who woke up hypohydrated would compensate for this sub-optimal state of hydration by time of pre-practice/game. Fortunately, the majority of players waking in a hypohydrated state had improved hydration statuses by pre-practice/game; however, these improvements weren’t substantial enough to bring those hypohydrated players back into a preferable, euhydrated state.
Limitations
There were some limitations to our study. Firstly, the effect of the female menstrual cycle on hydration indices was not taken into consideration over the course of the study. Although literature remains unclear on the impact of the menstrual cycle on hydration, Volpe et al. (2009) found that hydration status did not differ over the phases of the menstrual cycle in female collegiate athletes (Volpe et al., 2009). Future studies are warranted to generate further knowledge and understanding on this. Secondly, in some instances, players missed sample collection in either the AM or PM; forgot to return samples; or, dropped out due to injury or lack of interest. This influenced statistical power and analytical options. Thirdly, the primary focus of this study was to purely monitor AM and PM hydration status via Usg; therefore, no measurement of pre/post body weight, sweat rate or practice fluid consumption or performance measures were taken. The addition of these measurements could have aided in providing more information on the individuality of hydration habits, sweat rates and performance for each player. Fourthly, we did not control for temperature during training and games or exposure to exercise conditions. Lastly, the Hawthorne effect may have played a role for some of the PM measures for hydration status that were observed (McCambridge et al., 2014).
Practical Applications
One of the most vital practical findings of this study was the confirmation that the vast majority of female soccer players awoke and attended practice or games already in a hypohydrated state. While the effect of sub-optimal hydration on sporting performance varies between individuals, neglecting to account for pre-event hypohydration could augment existing hydration levels and impair major physiological functions required in soccer. Therefore, to reduce the risk of impeded performance, monitoring hydration status should be recommended within teams. This practice could be put in place by assessing the first urine voided of the morning, with athletic trainers, coaches or staff, using a simple portable refractometer to measure Usg to quickly inform players of their initial hydration status and generate an individualized hydration plan for each player.
Conclusion
In conclusion, our data indicates that the participant’s hydration status in our study were predominately in the hypohydration state in the AM and PM. The highest incidences of hypohydration were found in the morning, with Usg values showing hypohydration of all players on 5 out of the 9 observed days. This prevalence of hypohydration is consistent with previous observations of female soccer players, but over a longer period of time. Hypohydration may negatively impact physiological, psychological, and skill related performance, it can also lead to an increased risk of injury or heat-related illness. Therefore, it is vital for coaches and athletic staff to be aware of the importance of adequate hydration, to monitor hydration status of players and consider the implementation of hydration practices. These practices could in turn help to alleviate the incidence of pre-exercise hypohydration, benefiting both the individual player and team performance on a whole.
Acknowledgements
The authors would like to thank the Department of Kinesiology at Auburn University at Montgomery and the assistance of the Human Performance Laboratory and its members for all the help and guidance throughout this study. The authors would like to thank Dr. Richard Armenta for his assistance with the statistical analysis. Furthermore, the authors would like to thank all the players, coaches and staff who cooperated and gave consent to participate in this study.

