











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkDengue epidemics have affected all Central American countries since 1993. Costa Rica reported 2 dengue-related deaths in 1997, (case fatality rate (CFR) of 1.4 per ten thousand cases of clinically-diagnosed dengue fever) and 2 in 1999 (CFR of 3.3 per the thousand cases of clinically-diagnosed dengue fever). However, despite an increased dengue incidence, there were no reported deaths in Costa Rica during the time period from 2000 to 2004.
In 1999, 6,040 cases of dengue were reported in Costa Rica. Of these, 117 were dengue with warning signs (DWS) or severe dengue with severe plasma leakage (SDSPL) cases.1 A review of the records of patients treated before August 1999, revealed that late application of appropriate therapeutic measures was a common factor among severe and fatal cases. For this reason, the National Inter Institutional Dengue Commission decided in early August of 1999, after detecting an epidemic in the province of Limón, to immediately establish a dengue ward (60 beds) in the local hospital. This was done with the purpose of applying the treatment protocols successfully used during the previous year’s epidemic in Hospital Manuel Mora in the city of Golfito. In both epidemics dengue virus serotype 3 was recovered. The data presented here was collected from the Dengue Unit at Hospital “Dr. Tony Facio”, in Puerto Limón, Costa Rica. The organizational aspects of the Dengue Unit have been presented in detail elsewhere.2
The clinical features of dengue vary with the age of the patient, the infecting virus serotype, and the immunologic response to a previous infection with a different serotype. Most individuals infected with dengue virus (DV) are asymptomatic or develop a mild, not well differentiated febrile illness. A more symptomatic form includes high bimodal fever, myalgia, headache, skin erythema, a positive tourniquet test, petechiae, upper respiratory symptoms, nausea, vomiting and diarrhea, all of which may last 3 to 7 days. Some patients present a mild mucosal bleeding. The laboratory tests demonstrate leucopenia and thrombocytopenia. This is in the case of classic dengue fever (DF), or dengue. When the fever drops (day zero) most patients recover, but a few patients develop the so called warning signs: abdominal pain, persistent vomiting, clinical plasma leakage (ascites, pleural effusion, edema), liver enlargement, restlessness or lethargy, and thrombocytopenia concurrent with an increase in the hematocrit. This clinical features received the denomination of severe dengue and comprises 3 clinical presentations: 1.- severe dengue with severe plasma leakage (SDSPL), with the former classification of grade I if plasma leakage is only present; grade II, if a moderate bleeding is present. More severe forms of dengue are the so called SDSPL grade III (reversible shock) and grade IV (profound shock). 2.- severe dengue with severe hemorrhage, and 3.- severe dengue with severe organ impairment.
Dengue is a major global health problem. This vector-borne viral disease has been estimated to cause 50 million infections annually, including 500.000 cases of SDSPL, and at least 12.000 deaths.6 Costa Rica reported 1 dengue-related death in 1995, CFR = 1.9/10000 cases of clinically-diagnosed DF, in 1996 1 dengue related-death (CFR= 4.3)/10000 cases), two dengue-related deaths in 1997 (CFR = 0.14/10000 cases) and 2 in 1999 (CFR = 3.3/10000 cases). Of these, 3 deaths were caused by SDSPL treated with saline solution, two were severe dengue with severe hemorrhage, and one presented with HELLP syndrome associated with DF.
The cardinal feature of SDSPL is not hemorrhage, but an increase in vascular permeability which causes plasma leakage. Dengue-infected blood cells, mainly macrophages, release pro-inflammatory cytokines which damage the zonula occludens (occludin, claudins, EV-cadherins) in the vascular endothelial cells, causing impaired permeability and reorganization of its barrier, promoting the plasma leakage.7-9 Plasma loss into the extravascular compartment causes hypotension, which could result in dengue shock syndrome (DSS).10-13 There is no effective antiviral drug against dengue virus (DV). The treatment of DWS, SDSPL and DSS is supportive; patients can recover after a critical period ranging between 24-72 h. 6
SDSPL has been compared with a severe, acute diarrheal syndrome.14 In both situations, rapid, large fluid losses cause hypotension and subsequently hypoxia and acidosis. In SDSPL the losses are directed to the extra-vascular compartment causing hypovolemia, which results in the release of catecholamines that cause arterial pulmonary and peripheral vasoconstriction. Hypoxia and acidosis cause arterial pulmonary vasoconstriction and arterial peripheral vasodilation. To reverse these ominous features it is necessary to restore the intravascular volume with a balanced polyelectrolyte solution containing alkali. This treatment counteracts acidosis, prevents the constriction of pulmonary arteries, and avoids pulmonary edema.15-17 The rate and amount of intravenous fluid can be regulated by monitoring the mean arterial pressure (MAP). The aim is to maintain the MAP during the hypotension period at a level between the lower and medium level.
The aim of this article was to present the administrative and therapeutic procedures adopted in Costa Rica to prevent dengue mortality, during the dengue epidemic of 1999, which included the use of polyelectrolyte intravenous solutions and monitoring of the patients using MAP level that is normal for age.
Methods
The new World Health Organization (WHO) classification for SDSPL was used, instead of the old classification that included dengue hemorrhagic fever.6
We report the treatment experiences of patients affected during the dengue epidemic in the province of Limón, Costa Rica, in August and September of 1999. Such treatment strategy was proven successful in 1998. The underlying scientific rationale for using MAP to detect, monitor and treat hypotension rather than the traditional recommended method of monitoring (serial hematocrits), was based on previous experiences in treating diarrheal dehydration with polyelectrolyte intravenous solutions.3-5
Patient recruitment and evaluation
Individuals presenting to the outpatient clinic with acute fever in the absense of an obvious focus of infection were followed-up until fever resolved. Those who presented with spontaneous bleeding, a platelet count ≤ 100 000/mm3, hypotension, or appearing very sick were admitted to the dengue ward. After a clinical assessment by a hospital physician, the patients or child’s parents or guardians were informed about the protocol, and the hospital admission document was signed. The diagnosis of severe dengue was established upon discharge of the patients, based on the clinical evolution and results of laboratory tests (platelet count, plasma protein and albumin levels). A diagnosis of SDSPL required the presence (or history) of acute fever, platelet count ≤ 100 000/mm3, low plasma protein or albumin, and spontaneous petechiae, bleeding, or a positive tourniquet test and clinical evidence of plasma leakage (edema, ascites, pleural effusion, low MAP).
Laboratory
Blood samples were collected for hemoglobin, hematocrit, leukocytes, platelets and serum protein levels on admission and every day until discharge. A blood sample was drawn during the first five days of the febrile period for virus identification using RT-PCR. Upon discharge and six days after the onset of fever, another blood sample was collected for serum anti-dengue IgM or IgG antibody determination.
Sodium, potassium, chloride, CO2, urea nitrogen, creatinine and glucose serum levels were determined with the Multianalizer Astra 8, Beckman Instruments, Fullerton, CA, USA. pH, partial pressure of carbon dioxide, and bicarbonate were determined with pH/Bood Gas Analyzer Model 131, Instrumentation Laboratory, Milan Italy. Plasma albumin levels were determined with Beckman Coulter Synchron, Brea CA. USA
Vital signs
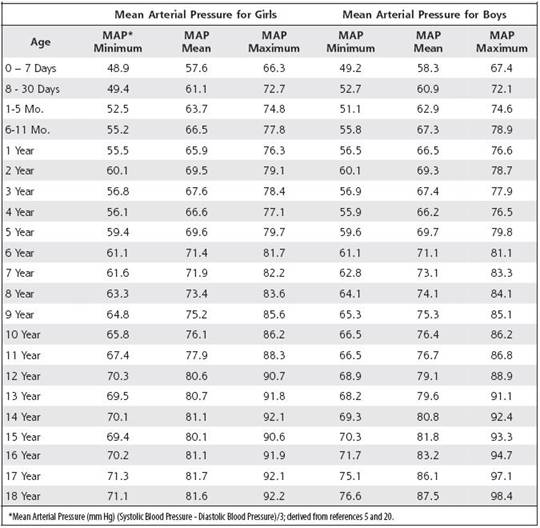
A blood pressure monitor was placed in one arm and vital signs were recorded hourly, and every 15 minutes after the first hypotensive episode. The initial blood pressure recorded at admission was considered the baseline blood pressure for each patient not presenting with indirect signs of hypotension (tachycardia and /or orthostatic syncope or pre-syncope, the latter referring to an episode which may include lightheadedness, dizziness, weakness or blurred vision). We defined hypotension as MAP between 68 and 61 mmHg for previously normotensive adult patients, or between 61 and 80 mmHg for previously hypertensive patients. Shock was defined as the hemodynamic condition when the MAP was minimum than 61 mmHg.10-12 A period of sudden hypotension or shock was arbitrarily defined as “Dip”. 18-19 In the absence of a standard MAP table for children, we devised a table according to the guidelines of the Task Force on Blood Pressure Control in Children.5 The MAP was estimated with the following formula: [(systolic blood pressure-diastolic blood pressure)/3)] + diastolic blood pressure.20 mean MAP was calculated from the mean blood pressure given by the Task Force on Blood Pressure Control in Children. The lower MAP was calculated from the mean blood pressure minus one standard deviation, while the maximum, as the mean blood pressure plus one standard deviation (Table 1). As such, the MAP for a 5 year old child is 70 mmHg and the minimum MAP is 60 mmHg. A 15% decrease from a MAP of 70 mmHg is 60 mmHg, and a 15% decrease from 60 mmHg is 51. For this 5 year old child, hypotension is defined as a MAP between 51 and 60 mmHg and shock as a MAP below 51 mmHg.
Urine output and volume of infused solution were recorded every 8 hours and were expressed as liters (L).
An intravenous line was placed in one arm using a catheter with a cap filled with heparin. Patients were invited to take more fluids than usual with WHO oral rehydration solution (ORS), plain water, or fruit juice. If they had mild to moderate signs of dehydration or developed persistent vomiting and were reluctant to drink fluids, a 25 mL/kg bolus of intravenous polyelectrolyte solution was administered during an hour. Thereafter, if the patient still could not drink fluids, it was administered at a rate of 2-3 mL/kg/h until oral hydration was established. Children under 10 years of age with hypotension received an intravenous polyelectrolyte solution that resembles the ORS, containing (mmol/L) Na+ 90, K+ 20, Cl- 60, acetate 30, and anhydrous dextrose 111, for a concentration of 311 mOsm/kg water. Adults with hypotension received intravenous “Dacca” solution, containing (mmol/L) Na+ 133, K+ 13, Cl- 98, acetate 48, and anhydrous dextrose 56, yielding 348 mOsm/kg water. The solution was infused at the maximum rate until the minimum normal MAP was registered. As MAP increased, the rate of infusion was diminished, until stabilization of MAP at a level between the minimum and mean normal values (70 to 80 mmHg for adults; for children, according to age and sex). When MAP rose to a level near the higher normal value, the infusion was stopped if there were no contraindications to oral hydration. No isotonic saline nor colloid IV fluids were used.
Results
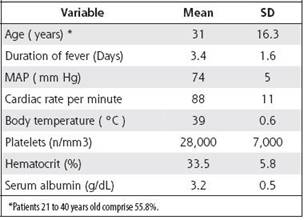
A total of 4,463 patients presented to the outpatient Fever Clinic from August 1st to September 30th of 1999. Of these, 1,010 were clinically and epidemiologically diagnosed as Dengue (D) and managed as outpatients, and 404 were hospitalized in the Dengue Unit. Of these, 110 (27%) were diagnosed as DWS or SDSPL, and none died. Laboratory tests confirmed that the infection was caused by DENV-3 in 20% of the 110 patients. The complete medical chart of the first 61 patients who developed DWS or SDSPL were reviewed. The main patients clinical features and laboratory tests on admission are presented in Table 2.
Patients age ranged from 5 to 80 years. Only 5 patients were younger than 15. The group included 41 women (67%) and 20 men (33%).
Thirty one (51%) patients were diagnosed as presenting with DWS and thirty (49%) patients presented with reversible shock and were classified as SDPL. The close supervision of patients avoided the progression of cases presenting with SDSPL to Irreversible Dengue Shock Syndrome.
Hypotensive episodes
Hypotension occurred 5.5 ± 1.3 days after the onset of fever, that is, the day of resolution of the fever, or shortly thereafter. The hypotensive episodes lasted from 15 minutes to more than 24 hours. Most patients presented one or two dips per day. The first and last dips were most commonly seen between days 1 and 3. In the group with SDSPL, three patients developed two shock episodes and 27 developed only one of such episodes. The lowest registered MAP was 50 mmHg in a 25 year old female. During the initial hypotensive episodes, the systolic blood pressure dropped, and the diastolic blood pressure was normal; thereafter, both of them dropped. The mean baseline blood pressure (mmHg, systolic/diastolic) was 103 ± SD 8/64 ± SD 5) and during the hypotensive episode 82 ± SD 7/50 ± SD 6.
Treatment
Twenty-two patients presenting with DWS received intravenous fluids (4.341 L ± SD 5.776) during the hypotensive episode, and on the the days after a total of 7.295 L ± SD 4.709 (p=0.036) The urine output during the hypotensive episode was 2.909 L ± SD 4.390, and on the the days between such episode and discharge was 9.564 L± SD 3.856 (p=<0.0001).
For those patients presenting with overt shock, the volume of intravenous fluid administered was 8.100 L± 5.945 during the hypotensive episode, and on the day until discharge they received 7.620 l ± SD 5.0 (p= 0.37) The urine output during the “dip” episode was 6.131 L ± SD 5.812, and the urine output between the “dip” episode until discharge was 8.879 L ± SD5.236 (p=0.032). During the intravenous treatment, when the minimum normal MAP was achieved, many patients had a urine output nearly equivalent to the intravenous volume administered. For instance, an 11-year old child received 17.5 mL/kg/hour over 7.5 hours, and had a urine output of 17.1 mL/kg/ hour. After the fourth day of hospitalization, he had lost 1.5 kg.
Laboratory findings
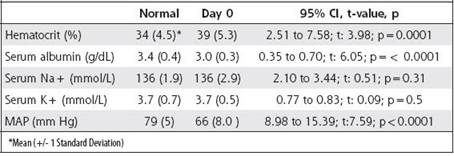
During the hypotensive period, the hematocrit increased in both SDSPL ( Table3) and DWS ( Table 4), and there was a statistically significant difference in the hematocrit decrease between the hypotensive period and the post hypotensive period in both groups (after receiving treatment): 14.7% and 12.6% drop in the hematocrit value (p=0.007 and p=0.00009 respectively). Patients with DWS developed their lowest platelet count on day 5.23 ± SD1.56 (mean value 27,353/mm3±7,710) similar to SDSPL patients (4.59 days ± SD1.60, p= 0.4, and mean value 27,852/mm3 ± SD 7,015, p=0.6). The minimum value for serum albumin was recorded on day 5 after the onset of fever for DWS and SDSPL. The mean nadir serum albumin level (g/ dL) was higher for DWS than for SDSPL (2.94 ± SD 0.33 and 2.84±0.39, respectively, p=0.03). The mean highest observed serum albumin level was lower in the SDSPL group compared with DWS (3.31 ± SD 0.47. and 3.50 ± SD 0.40, respectively, p=0.02). There was no significant difference between the mean higher or mean nadir serum albumin level for DWS and SDSPL (p=0.15 and p=0.25 respectively). The serum sodium level for the patients with DWS and SDSPL at the time of fluid administration was (mmol/L) 136 ± SD 2.89 and 136 ± SD 2.72 (p=0.25), respectively, and after recovery of the blood pressure was 136 ± SD 11.87 and 137 ± SD 2.22 (p=0.3) respectively. The serum potassium level during the administration of fluid was (mmol/L) 3.67 ± SD 0.55 and 3.36 ± SD 0.64, p=0.31 and after recovery was 3.7 ± SD 0.74 and 3.8 ± SD 0.29 (p=0.4) for DWS and SDSPL, respectively (Tables 3and 4).
Discussion
We have presented our experience in the management of DWS and SDSPL based on knowledge of the pathophysiology of the disease and the local resources available. By monitoring the MAP, and by administering intravenous fluids as soon as the MAP began to drop, we prevented a more severe hypovolemic state. The hematocrit did not increase over 20% as required by the WHO definition for SDSPL.21 As noted earlier, the hematocrit increased 14.7% in group SDSPL during the “dip” episode. The rapid intervention of administering intravenous fluid as soon as the MAP diminishes is a safer therapy that prevents more deleterious consequences. MAP monitoring can be easily performed as needed, and only requires a stethoscope and a sphygmomanometer with appropriate cuffs for the patient’s size. In our hands, monitoring vital signs by this approach was not only easier, but a more rapid and direct indicator of tissue perfusion.22 By monitoring the MAP it is possible to quickly detect the hypovolemic episode, its duration, and indirectely estimate the magnitude of volume loss. By infusing the appropriate rate of fluids to keep the MAP near the estimated minimum value, the intravascular volume is maintained in a physiologic range to avoid tissue hypoperfusion. During the hypotensive episode the administration of generous volume of intravenous polyelectrolyte fluid is safe because the urine volume is equally generous. But as soon as the MAP begins to rise, the urine output diminishes and the intravenous treatment must be slowed or stopped in order to avoid overhydration. By keeping the MAP between the mean and lower limits during the treatment phase we prevented overhydration. The serum albumin level was lower in the group with SDSPL, both in the higher and lower determinations compared with the DWS group, indicating the greater protein loss in the extravascular compartment in those patients in the SDSPL group.
Hypertension and obesity increase the MAP, therefore it is prudent to consider a urine output between 0.5 and 1.0 mL/kg/h, besides the normal MAP, as a requirement to assess fluid treatment in those patients.23-24
While catecholamines cause constriction in peripheral vessels, hypoxia and acidosis cause vasodilation.25-27 The approach to simultaneously fight hypovolemia and acidosis is achieved by means of administering a poly-electrolyte solution containing a balanced amount of sodium, potassium, chloride and bicarbonate (acetate), replenishing the intravascular volume, and at the same time preventing pulmonary vasoconstriction28 in order to avoid pulmonary edema, hence promoting blood oxygenation. The acidifying saline solution is not the preferable solution.
Table 3: Results of laboratory tests and Mean Arterial Pressure. Patients presenting overt shock, SDSPL.
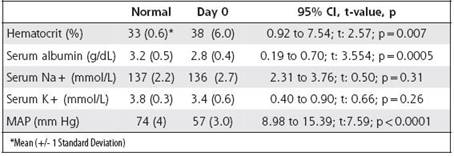
Table 4: Results of laboratory tests and Mean Arterial Pressure. Patients presenting hypotension, DWS
Dacca Solution was used for adults and a WHO ORS-like polyelectrolyte solution for children, with great success.
Our treatment protocol was based on careful reflection on dengue pathophysiology and the mechanisms of fluid loss in other situations, and the need to apply limited resources with maximum efficiency.
When this treatment protocol was used in uncomplicated DWS and SDSPL in Costa Rica, the mortality rate was null. Nevertheless unusual cases need a specialized approach in accordance with the problem (encephalitis, myocarditis, hepatic failure, etcetera).

