










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.54 n.3 San José Jul./Sep. 2012
Original
Esophageal leiomyoma.
Experiencewith nine
surgical patients
Giovanna
Mainieri-Breedy1, José-Alberto Mainieri-Hidalgo2
Thoracic
Surgery Department,
Dr.
Rafael Ángel Calderón Guardia, Caja Costarricense de Seguro
Social. Author’s Memberships:
1Gastric Cancer Early
Detection Center.
Hospital
Max Peralta, Caja Costarricense de Seguro Social. 2 Thoracic Surgery Department, Hospital Calderón Guardia, Caja
Costarricense de Seguro Social.
Abbreviations:
FNAB, fine
needle
aspiration biopsy; GIST, Gastrointestinal stromal
tumor; CAT scan, computed axial tomography; T2, measure on magnetic
resonance
that indicates an increased eco time and a greater repetition time;
EUS,
endoscopic ultrasound.
Correspondence:
mainierijose@hotmail.com
Abstract
Aim: The aim of
this study is to inform the experience acquired operating esophageal leiomyoma in the Thoracic Surgery Department of
the
Hospital Calderón Guardia.
Methods: Fourteen
patients with submucosal esophageal tumors
were
referred to the Thoracic Surgery Department at Hospital Calderón
Guardia during the twelve-year period comprised between 1999 and 2011.
The
approach for four asymptomatic patients with a small mass was
observation,
and the remaining ten underwent surgical procedures to confirm the histologic
diagnosis
of Leiomyoma. With authorization provided
by the
Ethical Committee of the Hospital, clinical records were reviewed,
considering
personal characteristics, symptoms, methods for diagnosis, surgical
treatment
and follow-up for the patients involved.
Results: Ten
surgical patients were analyzed, eight were male and two female. Their
age
ranged from 38 to 71 years, with an average of 56 years. Their primary
complaint was dysphagia. In three cases
the tumor
findings were incidental, while performing an upper endoscopy for
digestive symptoms.
In all cases the method used for detection was an upper endoscopy
describing
either a submucosal tumor or an extrinsic
compression
of the esophageal wall. The endoscopic ultrasound correlated in all
cases that
the tumor originated from the fourth layer of the esophagus, compatible
with leiomyoma. In two cases the
possibility of malignancy was
questioned due to the dimensions of the lesion. Nine patients were
operated
through a thoracotomy and one through a laparotomy. In 7 cases enucleating was
successful without
perforation of the mucosa. In two patients partial esophagectomy
with anastomosis and diaphragmatic patch
was
performed. In an exceptional case, the tumor extended from the cervical
esophagus to the esophagogastric union, so
a total esophagectomy was done with a
gastric interposition. There
was no mortality reported. One patient complicated with an
small anastomotic leak that was resolved
without
intervention. Two patients had respiratory problems that prolonged
their
hospital stay. In the 12 years and 8 months of follow up, there has not
been
any relapse or complication.
Conclusion:
The
surgery of submucosal esophageal tumors
can be
performed without mayor morbidity if there is an adequate preoperative
evaluation
and Management is made. None of the cases of this series had
complications or
recurrence to the date the study was made.
Key words:
esophageal leiomyoma, esophagus, tumors,
endoscopic
ultrasound.
Benign
tumors of the esophagus are rare, constituting
less than 1% of neoplasias of this organ. Leiomyoma is the most common, occurring in about
two thirds
of cases, representing 10% of gastrointestinal leiomyomas.
The rest are cysts and polyps. The overall incidence of esophageal leiomyomas is 8 to 43 per 10,000 cases, in a
series of
autopsies. 90% are diagnosed between the ages of 20 and 70 years old,
and are
twice as common in men than in women (2:1).1
Leiomyomas
are mesenchymal tumors that grow intramurally.
Mostly located in the distal third (60%), followed by the middle (33%)
and
upper third of the esophagus (7%).2 Histologically, the tumors are comprised
of smooth
muscle tangles, well-demarcated by adjacent tissue or by a connective
tissue
capsule. Macroscopically, well-defined masses are visualized in the
esophageal
wall; cut surface is solid with a grayish white color. The majority
occur as
single lesions, of less than 5cm in diameter, but 5% may be multiple,
especially
patients with Alport’s Syndrome. Large
tumors
present themselves as posterior mediastinal
masses
that compressed adjacent organs and may be confused with neoplasias.3
The
differential diagnosis is made with esophageal cancer, gastrointestinal
stromal tumors (GIST) and other benign
esophageal tumors.4
Leiomyomatosis is characterized by
diffuse
hypertrophy of all muscle layers of the esophagus and the presence of
lymphocytic and plasma cell infiltration; usually accompanied by leiomyomas elsewhere, neuropathy, hearing
problems, myopia
or astigmatism (Alport’s Syndrome). The
management in these cases consists of esophageal resection and
replacement with
the stomach or the colon. 5.7
When small
(less than 5cm), manifestation of symptoms
is rare. Their growth is usually slow and, as they grow, symptoms are
intermittent and progressive similar to those of esophageal cancer,
such as dysphagia, retrosternal
discomfort, chest pain, weight loss, esophageal obstruction and
regurgitation. The
size to produce symptoms is usually greater than 6 or 8cm.8
The
diagnostic methods commonly used are: esophagogram,
endoscopy, endoscopic ultrasound (EUS), and
computed axial tomography (CAT scan). On esophagogram,
the classic appearance is a filling defect, smooth and concave border
in the
underlying normal mucosa. 1,3 By
endoscopy,
a mobile submucosal lesion can be seen,
with a intact
mucosa. If a leiomyoma is suspected,
biopsy by any
method should be avoided, the tearing of the mucosa difficult extramucosal resection (enucleation).
If ulceration is present or there is suspicion of malignancy, a biopsy
should
be performed; a useful method is fine needle aspiration biopsy (FNAB).
If a
biopsy is performed, it is recommended to postponed surgery at least 2
weeks,
to allow the esophageal mucosa to heal and diminished the risk of
perforation. 9
Endoscopic ultrasound, demonstrate a homogeneous region of juxtaposed hypoechogenicity with the overlying mucosa. The
radiologic
findings of an
esophageal
leiomyoma described it as a marginal mass,
smooth,
round or lobulated, projecting to one or
both sides
of the mediastinum, along the course of
the
esophagus. The CAT scan disclosed homogenous intramural mass, round or
ovoid;
or a thickening of the esophageal wall, without alterations in the mediastinal fat. Magnetic resonance imaging with
T2, emit
an iso-intense signals, while esophageal
cancer emit
high intensity signals. 2,3
Small and
asymptomatic submucosal
tumors may be periodically monitored. The indication for resection is
based on
symptoms, size (>5cm), evidence of growth, ulceration or malignant
degeneration, but this is rare. 10 The recommended method
of
resection is enucleation, preserving the
integrity of
the mucosa. When the tumor is larger than 8cm, when adhered to the
mucosa, or
when there has been an extensive tearing during dissection, it may be
necessary
to remove part of the esophagus. The concomitant use of endoscopy helps
to
locate the lesion and detect perforations in the esophageal wall.11
In 1992, Everitt
reported the
first successful thoracoscopic esophageal enucleation, and in 2010, Wang et al reported 12-14
thoracoscopic resection of 42
esophageal leiomyomas or GISTs, with
diameters up to 5cm. Thus, concluding that endoscopic surgery can be
performed
with good results, although there is a greater risk for perforation
when
comparing to conventional surgery. 15
Mortality
of a thoracotomy
excision is 0-1.3%,2 and
the
described morbidity includes pain, atelectasia
and
pneumonia. The follow up consists in periodic esophagograms
and endoscopies to detect recurrences.
The goal
of this paper is to review the cases treated
in the Department of Thoracic Surgery of the Hospital Calderón
Guardia, which is a reference center of this condition, in order to
analyze and
inform particular characteristics of patients with leiomyomas,
detection tests and methods; and the results of surgical removal.
Materials
and methodology
Upon
review and approval of the protocol by the Ethics
and Research Comitee of the Hospital, we
review the
clinical records of fourteen patients included in the database of the
Department of Thoracic Surgery, which were evaluated as esophageal leiomyomas during the period 1999 and 2011,
analyzing the
patient’s characteristics, clinical detection methods and tests,
performed surgery and postoperative control. Four asymptomatic patients
with
suspected leiomyomas were not included in
the review
and continue control in the Gastroenterology Department.
Results
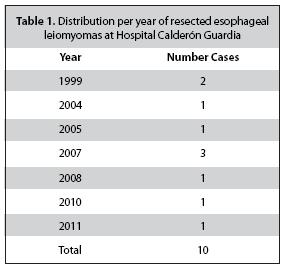
During the
studied period, 10 patients with esophageal
leiomyomas underwent surgery. Ages ranged
from 38 to
71 years old, with an average of
The
detection distribution per year is shown in table
1, and corresponds to less than one case per year, in a third level
national
reference center, attending a little more than a third of the adult
population.
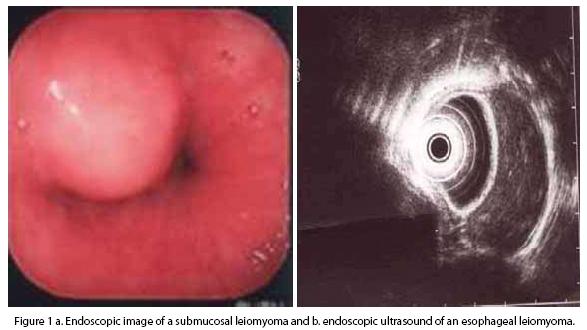
Of ten
patients, seven consulted for dysphagia,
and in three cases the finding was incidental,
while performing an endoscopy for upper gastrointestinal symptoms. The
detection method in all cases was with endoscopy, describing the
presence of a
well-defined submucosal lesion or an
extrinsic
compression of the esophageal wall, with integrity of the mucosa (Fig.
1a). In
one occasion, an ulceration of the mucosa was described.
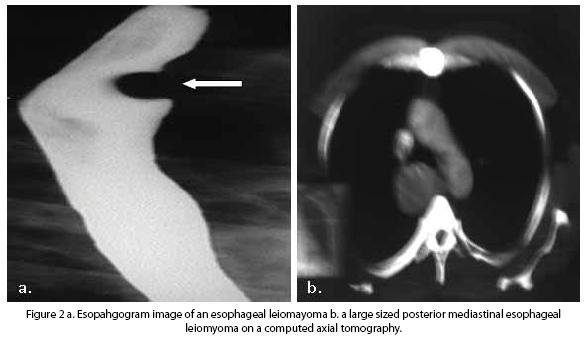
The esophagogram was
performed in five cases; in two cases an extrinsic compression of the
esophageal wall was described; in another two a lesion that diminished
the diameter
of the lumen of the esophagus, of origin to be determined, and in one
case, a submucosal tumor (Fig. 2a).
In nine of
ten cases, the endoscopic ultrasound
described a lesion that emerged from the fourth layer, with similar
size as
described by the pathologist in the surgical specimen. In one case, the
study
was not performed. The diagnosis by an ultrasonographist
was leiomyoma in seven cases, and leiomyoma
or leiomyosarcoma in 2 cases (Fig. 1b).
In one
case, the growth was towards the lumen,
reaching a great size, seen in a CAT scan as a posterior mediastinal
tumor (Fig. 2b).
Surgical
treatment in seven cases was enucleation
of the tumor, maintaining the integrity of the
mucosal layer. Two patients underwent partial esophagectomy
with end-to-end anastomosis and
diaphragmatic patch;
and in the case of a leiomyoma that
extended from the
neck to the cardioesophageal junction, a
total esophagectomy with gastric ascension
and cervical esophagogastro anastomosis was
performed.
The
location of the lesions, in one case was in the
proximal third, in an intrathoracic
position; eight
were located in the middle third, all underwent a right thoracotomy;
and one was in the distal third, and was accessed by laparotomy.
No patient
died. Apatient with
esophagectomy presented a small anastomosis
leakage, described in an esophagogram as a
diverticuli at the level of the anastomosis,
which did not require reintervention. Two
patients
developed respiratory infections that prolonged their post operatory
stay. One
complained of prolonged pain in the dermatome of the surgical approach,
requiring infiltrations and psychological support.
No
recurrences or complications have been presented
and the follow up of the patients varies from 8 months to 12
years.14
Discussion
Esophageal
leiomyoma is an
unfrequented tumor, and over a 12 years study, only ten were excised,
in a
higher national reference center. The main symptom, same as the
majority of
esophageal diseases, was dysphagia, so it
does not
direct to a specific diagnosis. However, the esophagogram
and the endoscopy are highly suggestive, with a classic image shown on
figures
1 and 2. It is relevant to point out the importance of not performing
any type
of biopsy in resectable tumors, so it can
be excised
extramurally, such as in the seven cases in which esophagectomy
was not required.
Endoscopic
ultrasound performed by an experienced operator,
helped to confirm the origin of the tumor in the muscle layer of the
esophagus,
such as in nine cases in the review, performed by the
The
tendency of the tumor is to compress the
esophageal lumen and cause obstruction, manifesting as dysphagia,
and this was the surgical indication in seven patients. In three cases,
the
tumor grew outside the wall; one of them reach a size of approximately
8cm and
in CAT scan was presented as a posterior mediastinal
tumor.
The enucleation was
performed in seven cases, without complications. The esophagectomy
was performed in three cases, associated in one case with a small anastomosis leakage with no further morbility,
and two patients presented respiratory infections, and were discharged
in the
tenth and twelfth postoperative day, in good conditions.
We
conclude that surgery of submucosal
tumors of the esophagus, when studied and handled properly
preoperatively,
surgery can be performed without increased morbidity, and in none of
the cases
studied were complications or recurrences to date of the review.
References
1. Punpale A, Rangole A, Bhambhani N, Karimundackal G, Desai N, de Souza A, Pramesh CS, Jambhekar N, Mistry R. Leiomyoma of Esophagus. Ann Torac Cardiovasc Surg 2007; 13:78-81. [ Links ]
2. Saleh W, Bamosa A, Al-Mutairi H, Al-Kattan K. Thoracoscopic enucleation of esophageal leiomioma in patient with MEN I syndrome. Ann Thoracic Med 2010; 5:47-49. [ Links ]
3. Yang P.S., Lee K.S., Lee S.J., Kim T.S., Choo I.W., Shim Y.M., Kim K., Kim Y. Esophageal Leiomyoma: Radiologic Findings in 12 Patients. Korean J Radiol 2001; 2:132-137. [ Links ]
4. Loviscek L.F., Yun J.H., Park Y.S., Chiari A., Grillo C., Cenoz M.C. Leiomioma de esófago. Cir Esp. 2009; 85: 147-51. [ Links ]
5. Boran C., Sengul N., Balaban Y.H., Gürel S. Multinodular leiomyoma of the esophagus with internodular hydropic degeneration and bulbous serosal protrusions similar to cotylednonoid uterine leiomyoma. Diseases of the Esophagus 2007; 20:187-189. [ Links ]
6. Okugawa Y., Mohri Y., Toiyama Y., Yokoe T., Ohi M., Tanaka K., Uchida K., Shiraishi T., Kusunoki M. Multiple Solitary Leiomyomas in the Esophagus: Report of a Case. Surg Today. 2011; 41: 563-567. [ Links ]
7.Obuchi T., Sasaki A., Nitta H., Koeda K., Ikeda K., Wakabayashi G.Minimally invasive surgical enucleation for esophageal leiomyoma: report of seven cases.Diseases of the Esophagus. 2010; 23: E1-E4. [ Links ]
8. Asteriou C., Konstantinou D., Lalountas M., Kleontas A., Setzis K., Zafiriou G., Barbetakis N. Nine year experience in surgical approach of leiomyomatosis of esophagus. World J Surg Oncol 2009; 7: 102. [ Links ]
9. Jiang G., Zhao H., Yang F., Li J., Li Y., Liu Y., Lui J., Wang J. Thoracoscopic enucleation of esophageal leiomyoma: a retrospective study on 40 cases. Diseases of the Esophagus. 2009; 22: 279-283. [ Links ]
10. Schorlemmer G., Battaglini J., Murria G. The Cervical Approach to Esophageal Leiomyomas. Ann Thoracic Surg 1983; 35: 469-472. [ Links ]
11. Li Z.G., Chen H.Z., Jin H., Yang L.X., Xu Z.Y., Liu F., Yao F. Surgical treatment of esophageal leiomyoma located near or at the esophagogastric junction via a Thoracoscopic approach. Diseases of the Esophagus 2009; 22: 185-189. [ Links ]
12. Zaninotto G., Portale G., Costantini M., Rizzetto C., Salvador R., Rampado S., Pennelli G., Ancona E. Minimally invasive enucleation of esophageal leiomyoma. Surg Endosc 2006; 20: 1904-1908. [ Links ]
13. Dapri G., Himpens J., Ntounda R., Alard S., Dereeper E., Cadiere G.B. Enucleation of a leiomyoma of the mid-esophagus through a right thoracoscopy with the patient in prone position. Surg Endosc. 2010; 24: 215-218. [ Links ]
14.Wang L., Fan C.Q.,Ren W., Zhang X., Li Y.H., Zhao X.Y.Endoscopio dissection of large endogenous myogenic tumors in the esophagus and stomach is safe and feasible: A report of 42 cases. Scandinavian Journal of Gastroenterology.2010; 46:627-633. [ Links ]
15. DeUgarte D., Teitelbaum D., Hirschl R., Geiger J.D. Robotic Extirpation of Complex Massive Esophageal Leiomyoma. J Laparoendoscopic & Advanced Surgical Techniques. 2008; 18: 286-289. [ Links ]
16. Slesser A.A.P., Shaw I. A Large Esophageal Leiomyoma. International Journal of Surgical Pathology 2009; 17: 401. [ Links ]
17. Gupta V., Lal A., Sinha S.K., Nada R.,


{kind=link}
{kind=link}
{kind=link}