










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.54 n.2 San José Apr./Jun. 2012
Original
Decision
to Study Medicine: Determinants and Specialty Choice
1Academic Research and Development Universidad de Iberoamérica, UNIBE.
2Academic Quality
Unit, Universidad de Iberoamérica, UNIBE.
Abbreviations: CCSS, Caja
Costarricense de Seguro Social; (Costa Rican
Social Security Institution)
CENDEISSS,
Centro de Desarrollo Estratégico e Información en Salud y
Seguridad Social. (Center
for Strategic Development and
Information on Health and Social Security)
Contact: apadilla@racsa.co.cr
Abstract
Introduction:
The decision to study medicine as a career depends on many factors,
including
intrinsic (personal) and extrinsic ones to the individual. To be aware
of these
factors could be useful for curriculum development and student
counseling.
Therefore, the study was proposed to identify the key factors taken
into
account to make this decision, intention of specialization and the main
areas
chosen.
Materials
and Methods: This is a
descriptive research based on a
survey applied to a sample of 84 active medical students of a private
university (Universidad de Iberoamerica,
UNIBE).
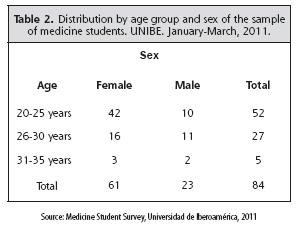
Results:
The survey was applied to 84 students, 28.6 % were male and 71.4 % were
female.
39.5% reported to have physicians as relatives. The main reason to
study
medicine was self-conviction without outside influence and motivation
due to
humanitarian issues. Most of them chose to study this career between 16
and 20
years old. 91.6% of the subjects surveyed has
the
intention to follow a specialty. The main choices for specialization
were Internal
Medicine and its specialties; followed by surgery and its related
branches.
Conclusion:
The study determined an important predominance of females. The main
motives to
study medicine and follow a specialization are humanitarian and
altruistic
ones. The areas with the highest demand are Internal Medicine and
Surgery. This
information might be useful for decision making on undergraduate
curriculum
management and for planning postgraduate specialization programs.
Keywords:
Decision, medicine programs, factors, specialty
According
to Blustein, the
motivations for choosing a career are intrinsic and extrinsic.
Intrinsic
motivation depends on the need to perform activities that provide
satisfaction.1
Extrinsic ones depend on external
factors such
as family or group influence. Furthermore, Krumholtz
postulates that there are 4 groups of factors that influence the
decision to
study certain careers: genetic and cultural, environmental conditions
and
events, learning experiences and task approach skills.2
Cultural and
genetic characteristics include ability, disability, ethnicity, gender
and
physical appearance. Learning experiences refer to the events which
influence,
such as contact with a disease or the presence of high-quality role
models.
Environmental conditions are mainly of an economic and geographical
kind.
According to this model, these 4 factors shape the self-belief and
define what
it is possible for us to achieve according to our environment.3
For
university authorities responsible for the
administration of a curriculum in medicine, it is extremely important
to know
the reasons that motivated the student’s career choice. This allows the
identification of students who require reallocation or counseling, and
helps to
make adjustments to the curriculum in order to allow students to obtain
the
greatest benefit according to their expectations. Furthermore, it is
important
to recognize the predominant orientation of the student either towards
the
practice of general medicine or towards specialization. This is because
students should compare themselves with the current and projected
demand in
their environment. According to the “Report on the Assessment of
Required
Medicine Professionals “ prepared by Parada
et
al for the Center for Strategic Development and Information on
Health and
Social Security [Centro de Desarrollo Estratégico e Información
en Salud y Seguridad
Social] (CENDEISSS) of the Costa Rican Social Security Institution [Caja Costarricense
de Seguro Social] (CCSS), the health model
currently practiced
by our social security system is aimed towards primary attention.4
Therefore, it is of great importance to have enough general
practitioners.
Nevertheless, there is also need for specialists,
since the projections for the next 10 years (from 2002 when the report
was
released) estimate that the number of specialists required would exceed
one
thousand. In conclusion, the demand for professionals in medicine is on
the
rise and a proportional supply of specialists and general practitioners
must be
guaranteed.
This is a
correlation-based descriptive research based
on a survey applied (given previous consent) to a sample of 84 active
students
of the Licenciatura∗ in
Medicine and Surgery at
the Universidad Iberoamericana, in San
José,
Costa Rica, during the period between January and March 2011.
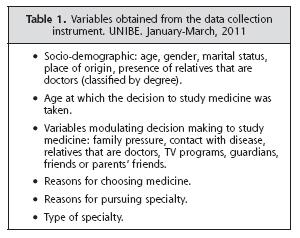
The data
collection instrument consisted of 35
questions, which were divided into 4 main sections. The first one,
comprising 6
questions, focused on socio-demographic factors. The second consisted
of 3
questions, aimed at the factors that determine the decision to study
medicine.
The third section sought to understand which were
the
personal motivations to choose to study medicine, for which 23
questions were
assigned. In the fourth and final section, the instrument asked
about the
interest and inclination towards undertaking a medical specialization.
For this
last part, 3 questions were assigned. Prior to its application,
professionals
in psychology and medicine working for the university that conducted
the study
approved the questionnaire.
The
variables obtained from the instrument are shown
in Table 1.
This study
was approved by the Institutional Research
Ethics Committee of UNIBE on July 2, 2010. The data obtained from the
survey was
processed using the SPSS (Statistical Package for Social Sciences
version 17,
2008, IBM Corporation,
Results
A total of
84 surveys were obtained, but several
questionnaires showed some incomplete answers, this missing data did
not exceed
5.0% of total responses. The majority of respondents (38.8%) came from
the
With
respect to the distribution by marital status,
most of the respondents are single (88.2%). In the case of age-marital
status relationship,
although most respondents in the 20-25 years age group are single in a
ratio of
approximately 4 to
To the
question about having any relatives that are
doctors, the answer was affirmative in 39.5% of the cases. For those
respondents whose answer was affirmative, most replied that the
relative was an
uncle/aunt or cousin. In only 8.1% of cases, it was the father and in
only 2.3%
of cases it was the mother.
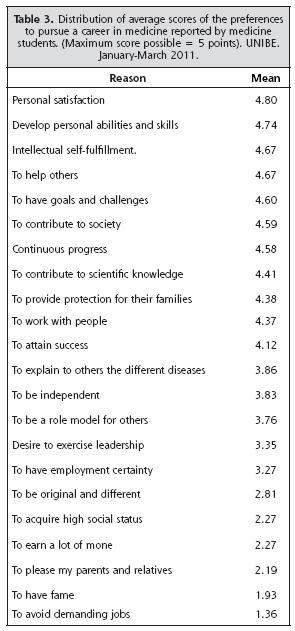
In order
to assess the determinants for the decision
to study medicine, a scale of 1 to 5 points was defined to assign each
of the
reasons to study medicine. After obtaining the average for each reason
with
respect to the entire population, the top three reasons in descending
order
were: personal satisfaction, to develop personal skills and
intellectual
self-fulfillment. Only a minority of respondents said that they took
the
decision because of family pressure (Table
3). The majority of the
respondents
indicated that the age at which they decided to study medicine was
between 16
and 20 years (57.0%). Only 15.1% indicated an age of less than 10 years.
With
regard to interest in undertaking a specialty,
91.6% of respondents answered affirmatively. The percentage of
undecided was
only 7.1%. As to the motivation to make a specialty, most of those who
said
that it would allow them to help other people, were women in a ratio of
3 to 1
with respect to men. This ratio is virtually the same in all of the
reasons
assessed, including the one referred to obtaining a higher income.
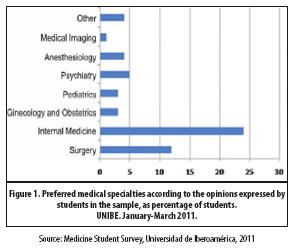
As to the
actual specialty, internal medicine and its
subspecialties prevailed with a 27.9%, followed by surgery and related
sciences
with 14%. (Figure 1).
Discussion
The
subject of vocational orientation has been widely
studied and has stirred several theoretical proposals to explain career
choice.
At very early stages vocational orientation adopts even unrealistic
forms, and
it is not until adolescence that a transition occurs towards a more
realistic
reasoning about the consequences and responsibility of choosing a
career.
Donald Super proposed in his vocational choice theory 6 stages:5
Crystallization
stage (ages 14-18)
Specification
stage (ages 18-21)
Implementation
stage (ages21-24)
Stabilization
stage (ages 24-35)
Consolidation
stage (age 35)
Readiness
for retirement stage (age 55)
One of the
main contributions of Super’s
vocational choice theory has been the emphasis he assigns to the
self-concept
in taking this decision. Later, in 1959, John Holland adds his own
theory and
establishes that the choice of an occupation depends on personal needs
and what
provides him or her self-fullfilment.6 This
includes the possibility to perform their skills and abilities, express
their attitudes,
as well as assimilate problems and roles. Also in this regard, Bandura developed the social learning theory in
which
genetic and learned factors influence the individual’s self-efficacy.7
So, if a person believes that he or she possess the skills to succeed
in a
particular occupation, and that pursuing that occupation will bring
success in
life, he or she will persevere in studying and training to achieve it.
Under the
premise of the latter theory, it can be deduced
that it is more likely that a student with the skills and the best
vocational
profile to be a doctor will maintain interest in the career and finish
it.
Acknowledging this allows for appropriate counseling and eventually a
reduction
in dropout and fail rates on the courses of
the
medicine curriculum. This study showed, for the analyzed population,
predominance of females and of a motivation based primarily on self-fullfilment. Similarly, Soria
et
al found that the motivation to enter this career was mainly
altruistic and
humanitarian.8
On gender
differences, Millán
et al found greater emotional maturity and sensitivity among
female
medicine students, while male students showed a strong sense of
utilitarianism
and of competition.9 The present
study did
not find an important difference on this utilitarianism between the
sexes.
Apart from these differences in the psychological profile, it has been
shown
that women must face more obstacles than men to enter medical school.
According
to Reed et al, domestic responsibilities, discrimination,
rigidity of
the career structures and psychological barriers are some of the
adverse
situations for women to choose medicine as a career.10
The
intention to specialize and which were the main
choices were also evaluated. On the same aspect, Wright and et al
investigated the choice between general medicine or
specialty by students in three medical universities in
In our
study, most of the respondents indicated they
made the decision to study medicine at an age between 16 and 20, which
corresponds to an overlap between the age of crystallization and
specification
of Super’s stages. Therefore, if planning to increase the availability
of
general practitioners, it would be necessary to conduct an early
motivational
strategy. This is so important that Bunker highlights the need to
include in
the prevocational stage of the medicine student’s training, exposure to
family practice and to motivate towards this alternative.14
Finally,
Thistlewaite proposes as an alternative to
foster an
increase in the percentage of students that choose to be a generalist
or at
least to practice family medicine; to show the flexibility, autonomy
and
holistic advantages it offers.15
Although
it was not evaluated in this study, there are
other factors that influence the choice of specialty, such as the type
of
personality. Thereon, Petrides et al
found
that in the case of internal medicine, students showed affinity for
research,
while those who chose surgical specialties were more practical.16
The choice of specialty may vary, and only 20% of students enter the
specialty
they had planned at the beginning of their career studies.17
Scott et
al show that influence of a medical tutor that can either support
or
dissuade them from the decision is among the factors related to the
change of
specialty choice.18
In
summary, this study confirms, like others, that
humanitarian reasons prevail as motivators for deciding to study
medicine. No
important family influences were identified. There is very little
interest to
continue as general practitioners. The motivation to specialize is
primarily
altruistic and of self-fulfillment and not economic. It must be
recognized that
the research undertaken did not explore other potential factors that
might
condition the decision to study medicine and the influence of other
factors in
choosing a certain specialty; which could encourage a further study.
Despite
these limitations, this research allows academic authorities to
identify the
student’s motivations and to take them into account in the review of
the
curriculum.
References
1. Blustein DL. The relationship between motivational processes and career exploration. J Vocat Behav.1988; 32:345-357. [ Links ]
2. Krumholtz, JD, Mirchell AM, Jones GB. A social learning theory of career selection. Counseling Psychologist. 1976; 6:71-81 [ Links ]
3. Mc Harg J, Mattick K, Knight LV. Why people apply to medical school: Implications for widening participation activities. Med Educ. 2007; 41:815-821. [ Links ]
4. Parada N, Méndez E, Fuentes C, Baéz N. Valoración de Necesidades Cualitativa y Cuantitativa de Profesionales en Medicina: Estimación a 5 y 10 años. Centro de Desarrollo Estratégico e Información en Salud y Seguridad Social. (CENDEISSS), Caja Costarricense del Seguro Social, 2002. [ Links ]
5. Super D. Dimensions and Measurements of Vocational Maturity. Teachers College Record. 1955; 57:151-163. [ Links ]
6. Holland JL. A theory of vocational choice. Journal of Counseling Psychology. 1959; 6:35-45. [ Links ]
7. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977; 84:191-215. [ Links ]
8. Soria M, Guerra M, Giménez I, Escanero J. La decisión de estudiar medicina: características. Educ Med. 2006; 9:91-97. [ Links ]
9. Millán L, Soares R, Rossi E, Neves De Marco O, Bueno Millán M, Vaz de Arruda P. What is behind a student´s choice for becoming a doctor? Clinics 2005; 60:143-150. [ Links ]
10. Reed V, Buddeberg-Fischer B. Career obstacles for women in medicine: an overview. Med Educ. 2001; 135:139-147. [ Links ]
11. Wright B, Scott I, Woloschuk W, Brenneris F. Career choice of new medical students at three Canadian Universities: family medicine versus specialty medicine. CMAJ. 2004; 170:1920-24. [ Links ]
12. Shadbolt N, Bunker B. Choosing general practice. Aust Fam Physician. 2009; 38:53-5. [ Links ]
13. Jordan J, Brown JB, Russell G. Choosing family medicine. Can Fam Physician. 2003, 49:1131-37. [ Links ]
14. Bunker J, Shadbolt N. Choosing general practice as a career. Aust Fam Physician. 2009; 38:341-344. [ Links ]
15. Thistlethwaite J. Kidd M, Leeder S. Choice of general practice as a career. Aust Fam Physician. 2008; 37:964-967. [ Links ]
16. Petrides KV, McManus IC. Mapping medical careers: Questionnaire assessment of career preferences in medical school applicant and final year students. BMC Medical Education 2004; 4:1-17. [ Links ]
17. Kassebaum DG, Szenas PL. Medical student career indecision and specialty rejection: roads not taken. Acad Med. 1995; 70:937-43. [ Links ]
18. Scott I, Gowans M, Wright B, Brenneis F. Why medical students switch careers Changing course during the preclinical years of medical school Can Fam Physician. 2007; 53:94–5. [ Links ]
19. Newton D, Grayson M. Trends in career Choice by US Medical School Graduates. JAMA. 2003; 290:1179-1182. [ Links ]
20. Chang P, Hung C, Wang K, Huang Y, Chang K. Factors Influencing Medical Students Choice of Specialty. J Formos Med Assoc. 2006; 105:489-496. [ Links ]
Date
received: June 9, 2011 Date
accepted: February 15, 2012


{kind=link}