










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.54 n.2 San José Apr./Jun. 2012
Original
Characteristics
of Prenatal Care of Pregnant Adolescents, Department of Obstetrics,
Hospital “Dr.
Rafael Angel Calderón Guardia”, 2010
Loretta Giacomin-Carmiol,
Manrique Leal-Mateos
Maternal-Fetal
Department Calderón Guardia Hospital, CCSS.
Abbreviations: CCSS, CajaCostarricense
de Seguro Social
[Costa Rican Social Security
Institution]; CLAP, Centro Latinoamericano
de Perinatologíay DesarrolloHumano
[Latin American Center
of Perinatology
and Human Development];
STDs, Sexually
Transmitted Diseases;
HCG,
“Dr. Rafael Angel Calderon
Guardia” Hospital.
Abstract
Aim:
To compare perinatal results of pregnant
adolescents
that attend the prenatal control consultation at HCG with those
published by
the CLAP for adolescent population in
Materials
and methods: 360
medical records of pregnant patients
under 18 years, that undertook prenatal control at the Adolescents’
Clinic of the Department of Obstetrics of the HCG in 2010, were
studied. The
variables included in the study were those related with prenatal care,
childbirth and postpartum.
Hypothesis
Testing was used to compare the results
obtained in this investigation with those reported by the CLAP. 1.96
was
adopted as the critical value from Z distribution (p <0.05).
Results:
This study showed that maternal morbidity and mortality of adolescent
patients
that received attention in our hospital is lower than that reported by
the
CLAP. Although there was a higher
percentage of some
diseases such as urinary tract infections or anemia in our population,
this
might be due to a better case detection system rather than to an
increase in
disease. With regard to the newborn, there were no significant
differences with
respect to the percentage of preterm births, low birth weight or very
low birth
weight. The fact that approximately 97% of patients had their labor at
term or
close to it (more than 34 weeks gestation) and having a Neonatal
Intensive Care
Unit could explain the low neonatal mortality present in our study’s
adolescents.
Conclusions:
Maternal and neonatal morbidity and mortality in adolescent patients
that
received attention in our hospital is lower than that reported by CLAP
for
adolescent populations.
Keywords:
Adolescents, pregnancy, prenatal control.
In 2005,
the Centro Latinoamericano
de Perinatología y DesarrolloHumano
[
However,
The
purpose of the hereby-described study was to
compare the obstetric outcomes obtained in our hospital with the ones
derived
from CLAP’s research.
Method
We did an
analytical observational cross-sectional
study based on the clinical records of the adolescents that received
prenatal
care during the study’s period. This research was approved by the
Research Ethics Committee of the HCG prior to its execution (Document
CLOBI-13-11-2010).
Using a
consecutive non-probability sampling, 360
medical records were included and analyzed. These records corresponded
to
pregnant patients under 18 years that
undertook
prenatal care at the Adolescents’ Prenatal Clinic of the Department of
Gynecology and Obstetrics of the
The
analysis excluded any patient who had an
incomplete form of any of the variables of interest that would not
allow
meeting the study’s objectives.
The
patients were identified using the daily schedule
of the Adolescents’ Prenatal Care Clinic Consultation. The medical
record
number of each patient was obtained from the schedule in order to
request the
record for review. In case the patient met the exclusion criteria, a
new one
replaced her in a consecutive manner.
The
maternal variables related to prenatal care
included were: age in years, marital status, occupation, school
dropout, use of
licit and illicit drugs, age of first intercourse, number of sexual
partners,
history of sexual transmitted diseases, history of sexual abuse, number
of
pregnancies, history of use and type of birth control method, desired
pregnancy, history of abortions, morbidity previous to pregnancy,
pregnancy-induced morbidity, number of prenatal care visits,
pre-pregnancy body
mass index and weight gain during pregnancy, number of hospitalizations
during
pregnancy and pre-delivery hemoglobin.
The
variables analyzed related to child birth were:
gestational age in complete weeks, type of delivery, use of episiotomy,
presence of tears and presence and type of postpartum complications.
The
neonatal variables studied were: sex, weight at
birth in kilograms, height in centimeters, head circumference in
centimeters, Apgar score at 5 minutes,
need for neonatal resuscitation,
need for hospitalization, number of days in hospital and newborn’s
condition when discharged.
The
information was collected using a spreadsheet
designed for this study.
The EpiInfo 2002 program was
used for processing of data. Qualitative variables were analyzed using
frequencies and proportions. The results obtained from the quantitative
variables were expressed using the arithmetic mean and standard
deviation. For
the comparison of the results obtained in this investigation with the
ones
reported by the CLAP, a Compliance Test for Hypothesis Testing was
used. The
significance level established was values of Z less than or greater
than 1.96
(p ≤0.05)9. Excel 2007 was used to create the tables.
Results
General
characteristics of the study population
From the
total study population, the mean age was 16.6
years (SD + 1.16). A56.1% (n=202; 95% CI 50.8-61.3) of the patients
were single
at the time of their first prenatal care appointment. The percentage of
school
dropout was 51.7% (n=186; 95% CI 46.4-56.9) and only 6.7% (n=24; 95% CI
4.4-9.9)
had some kind of employment. A 7.5% (n=27, 95% CI 5.1-10.9) reported to
have
used some type of legal or illegal substance. The prevalence of
smoking, as
well as of alcohol and drug consumption for the total sample was 18.1%
(n=65;
95% CI 14.3-22.5), 0.6% (n=2; 95% CI 0.1-2.2) and 2.8% (n=10; 95% CI
1.4-5.2),
respectively.
A16.9%
(n=61; 95% CI 13.3-21.3) suffered from some
type of disease before pregnancy. Of these, 34.4% (n=21; 95% CI
27.7-47-7)
reported bronchial asthma as the most common disease.
The mean
age of first sexual intercourse was 15.1
years (SD + 1.29). The median of sexual partners was 2, with a range
from 1 to
30. The prevalence of sexually transmitted diseases (STDs) diagnosed in
the
sample was 6.7% (n=24; 95% CI 4.4-9.9). The most common STD diagnosed
was
infection with human papillomavirus in 19
of these 24
patients (79.2%; 95% CI 57.8-92.9). Only 5.3% (n=19; 95% CI 3.3-8.3)
reported
history of sexual violence.
A 79.2%
(n=285; 95% CI 74.6-83.2) reported their
pregnancy as "unplanned." In contrast, only 28.1% (n=101; 95% CI
23.5-33.1) reported to have used some birth control method after the
onset of
sexual intercourse. Oral contraceptives were the most used by 52.5%
(n=53; 95%
CI 42.3-62.5) of patients.
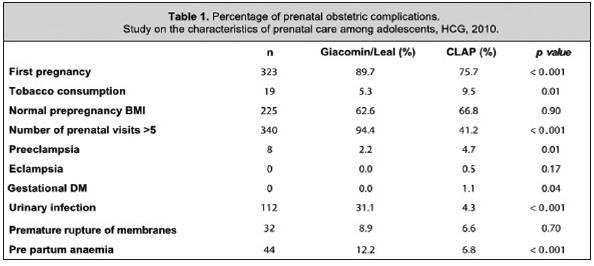
Characteristics
of prenatal care
Regarding
their prenatal care, 89.7% (n=323; 95% CI
86.1-92.7) of patients were in their first pregnancy. Only 62.2%
(n=224; 95% CI
57.0-67.2) had reliable dates of last menstrual period. However, 72.8%
(n=262;
95% CI 67.9-77.3) had an ultrasound early in the first quarter that
confirmed
gestational age.
A 94.4%
(n=340; 95% CI 91.4-96.5) reported more than 5
prenatal care appointments. Only 62.6% (n=221; 95% CI 57.3-67.7) had a
normal
pre-gestational Body Mass Index (BMI). The mean weight gain during
pregnancy
was
A 12.2%
(n=44; 95% CI 9.1-16.2) of patients suffered
from anemia. The mean value of pre-partum hemoglobin was 12.3 g/dl (SD
+ 0.97).
The 31.1% (n=112; 95% CI 26.4-36.2) reported some type of urinary tract
infection. A 2.2% (n=8; 95% CI 1.0-4.5) suffered from pre-eclampsia;
there were no cases of eclampsia. Neither
were there
cases of gestational diabetes mellitus; the mean blood glucose value
following
a 50-gram glucose load was 95.1 mg/dl (SD + 15.6).
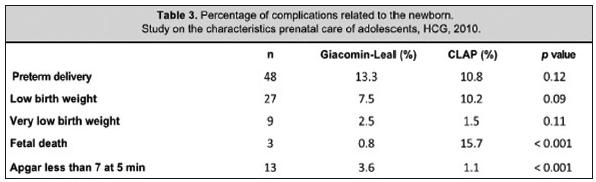
Only 16.5%
(n=59; 95% CI 12.9-20.8) of the patients
required hospitalization during their pregnancy. The most common
diagnosis for
hospitalization was threat of preterm delivery in 24 of these 59
patients
(40.7%; 95% CI 28.1-54.3). The prevalence of preterm delivery on the
sample was
13.3% (n=44, 95% CI 10.1-17.4). Out of the total patients, 3.3% (n=12;
95% CI
1.8-5.9) gave birth before 34 weeks and 10.0% (n=36; 95% CI 7.2-13.7)
between
gestation weeks 34 and 37. An 8.9% of them (n=32; 95% CI 6.2-12.4) had
a
premature membrane rupture.
The
percentage of congenital defects detected during
prenatal care was 5.3% (n=19; 95% CI 3.3-8.3). Of the total of defects
detected, those related to the urinary system were the most common
(n=4/19;
21.5%).
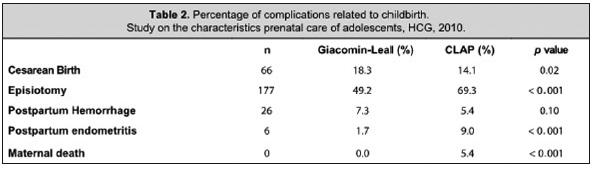
Characteristics
ofthe delivery
With
respect to the variables of delivery, the mean
gestational age was 38.2 (SD ± 2.2) weeks. The mean weight of newborns
was
Characteristics
of the postpartum
Regarding
the postpartum variables, 24.2% (n=87; 95%
CI 19.9-29.0) had at least one complication. Of these, the most
frequent
complication was postpartum anemia in 33.3% (n=29, 95% CI 23.6-44.3) of
cases,
followed by episiotomy dehiscence in 20.7% (n=18; 95% CI 12.7-30.7) and
mastitis in 17.2% (n=15, 95% CI 10.0-26.8) of the cases.
Tables 1, 2 and 3 show the
comparison
between
adolescents in our study and what the CLAP published in their 2005 study
Discussion
This
research shows the results obtained from a study
of the patients who attended the adolescents’ consultation of the HCG,
which was formally established in the year preceding the execution of
this
research. Because it is a hospital-based study and not a population
study, the
results are applicable only to patients treated in the HCG.
This study
is not free from information bias, since it
uses information from the medical records of the patients
asa source of data.
Notwithstanding
these methodological limitations, this
material shows how maternal morbidity and mortality of adolescent
patients
treated in our hospital is lower to the one reported by CLAP.13
Although some diseases, such as urinary infections and anemia, occurred
on a
significantly higher percentage in our population, this is perhaps due
to a
better detection system rather than to an increase of the pathology. In
recent
years, it has been compulsory to conduct a urinalysis on all patients
in every
prenatal care visit and to evaluate at least on two occasions
hemoglobin levels
in our patients. This could justify the results obtained.10
Likewise,
the percentage of more-than-5 prenatal care
appointments in our population surpasses those reported by the CLAP13,
suggesting also a better surveillance system for these diseases during
pregnancy. The latter may be improving also due to early detection of
modifiable risk factors or certain diseases, such as preeclampsia,
which,
recognized in advance, decrease the prevalence of obstetric
complications in
our teenagers.
With
regard to the newborn, we did not find significant
differences in the percentage of preterm births, underweight or very
low birth
weight products. While it was not detailed in the paper published by
CLAP13,
approximately 97% of births patients treated in our clinic came at or
near term
(more than 34 weeks gestation), which could explain the low neonatal
mortality
in our adolescents. However, it should be noted the HCG also has a
Neonatal
Care Unit that allows an integral treatment of patients and allows the
provision of specialized resources for their care.
However,
even if taking into consideration the
availability of resources offered by our hospital, we consider that
most of the
good results obtained in this study are due to the implementation of an
exclusive outpatient clinic for the pregnant adolescent patient. The
integrated
(perinatologist, nurse midwife,
psychologist and
social worker) and systematic approach of patients allows, as we said
above,
the early identification of some factors or situations, that when
recognized
early, decrease the prevalence of obstetric complications.
Contribution
of each author: each of the authors
participated in the planning of the study, collection and processing of
data,
as well as in the analysis and interpretation of it.
References
1. Maddaleno M, Silber TJ. An epidemiological view of adolescent health in Latin America. J Adolesc Health. 1993; 14:595-604. [ Links ]
2. Scholl TO, Hediger ML, Belsky DH. Prenatal care and maternal health during adolescent pregnancy: A review and meta-analysis. J Adolesc Health 1994; 15: 444-456. [ Links ]
3. Otterblad OP, Cnattingius S, Goldenberg RL. Determinants of poor pregnancy outcomes among teenagers in Sweden. Obstet Gynecol 1997; 89: 451-457. [ Links ]
4. Fraser Am, Brockert JE, Ward RH. Association of young maternal age with adverse reproductive outcomes. N Engl J Med 1995; 332: 1113-1117. [ Links ]
5. Jolly MC, Sebire N, Robinson HS, Regan L. Obstetrics of pregnancy in women less than 18 years old. Obstet Gynecol 2000; 96: 962-966s [ Links ]
6. Smith GC, Pell T. Teenage pregnancy and risk of adverse perinatal outcomes associated with the first and second births: Populations based retrospective cohort study. BMJ 2001; 323: 476-479. [ Links ]
7. Berg CL, Chang J, Callahan WN, Whitehead SJ. Pregnancy- related mortality in the United State 1991-1997. Obstet Gynecol 2003; 101:289-296. [ Links ]
8. Conde A, Belizán JM, Lammers C. Maternal-perinatal morbidity and mortality associated with adolescent pregnancy in Latin America: Cross-sectional study. Am J Obstet Gynecol 2005; 192: 342- 349. [ Links ]
9. Sentís J, Pardell H, Cobo E, Canela J. Prueba de hipótesis. En: Manual de Bioestadística 2º ed. Barcelona: Masson; 2001. pp 125-138. [ Links ]
10. Caja Costarricense del Seguro Social. Guía de la atención integral de las mujeres, niños y niñas en el periodo prenatal, parto y postparto. San José: C.C.S.S. 2009. [ Links ]


{kind=link}
{kind=link}
{kind=link}