











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
The American Association of Endodontists (AAE) describes that the primary objective of endodontic treatment is to prevent and intercept pulpal/periradicular pathosis and preserve the natural dentition when affected by pathosis (1). Endodontic treatment involves chemo-mechanical preparation of the root canal system to eliminate organic, inorganic, and bacterial products, in addition, to sealing the radicular space with a biocompatible material (1). Among the essential phases in endodontic treatment are the disinfection and filling of the root canal, which are primordial for the microbial reduction (2).
A vital pulp tissue maintains an immunological defense capacity. However, a microbial infection will develop in a root canal with necrotic pulpal tissue. The colonization of microorganisms within the root canal represents the main etiological factor of periradicular pathologies (Figure 1) (3).
Thus, teeth diagnosed with pulp necrosis must be considered infected, regardless of the presence or absence of a visible radiographic periapical lesion. Pulpal and periapical pathologies are usually inflammatory and of microbial etiology. Microorganisms and their products play a significant role in the induction and perpetualization of these pathologies (2,3).
The infection of endodontic origin has some characteristics that differentiate it from other infections in the organisms since it cannot be treated through systemic antibiotic therapy. As the pulp tissue is necrotic, no blood vessels can transport the cells and molecules of the immune defense system, as well as antibiotics, into the root canal. Moreover, the microorganisms are contained within the root canal system's microstructure. Thus, this type of infection can only be treated through professional intervention with endodontic treatment.
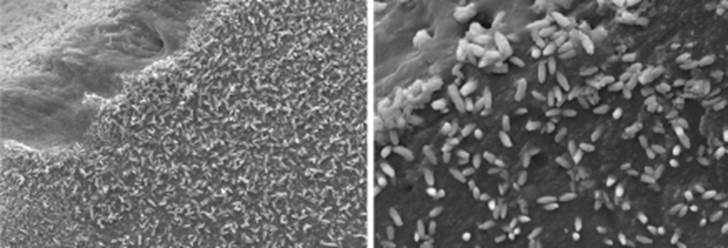
Figure 1 Representative photomicrographs of a radicular canal wall of a tooth diagnosed with pulp necrosis (unpublished data). Photomicrographs were taken with an SEM Philips XL 30 in UFSC, Brazil. A microbial infection will develop in a root canal with necrotic pulpal tissue. Teeth diagnosed with pulp necrosis must be considered infected, regardless of the presence or absence of a visible radiographic periapical lesion.
Cleaning and disinfection
The root canal treatment success depends on correct chemo-mechanical disinfection. Irrigation is a crucial part of this achievement. Irrigants facilitate the removal of microbes, necrotic and inflamed tissue, and debris (4,5). Moreover, irrigation improves the cutting efficiency of rotary and endodontic files by reducing the friction between the instruments and dentin (5,6).
Complete intracanal disinfection is challenging due to the complex anatomy that root canals generally present. Thus, different irrigating agents are used during biomechanical preparation.
Sodium hypochlorite (NaOCl) is the most worldwide used irrigant in endodontics (1,2,3,4,5). NaOCl is antibacterial, dissolves organic tissue, and removes biofilm due to the hypochloric acid affecting the microbial cell's vital functions, resulting in cell necrosis (5,7,8). Sodium hypochlorite in concentrations of 0.5% to 5.25% has a series of relevant properties, among them the effectiveness of dissolving organic tissue, in addition to being antimicrobial. It is ineffective against specific microorganisms at low concentrations, and at high concentrations, it has low biocompatibility, which can cause periapical inflammation (4). Although sodium hypochlorite is the irrigant of choice, it cannot dissolve inorganic tissue present in the smear layer. Evidence showed that microflora and toxins are accumulated in the smear layer, allowing the survival and reproduction of bacteria (9,10).
The combination of different irrigating solutions, which have the capacity to promote inorganic debris removals, such as 17% ethylenediaminetetraacetic acid (EDTA) and citric acid, has been proposed. Both solutions effectively remove the smear layer, and their chelating action generates the detachment of the biofilm found on the canal walls (11). However, alternating NaOCl with EDTA during the instrumentation procedure will detriment the antibacterial activity of NaOCl and should be avoided (5). Evidence showed that the tissue previously exposed to EDTA is not effectively dissolved by NaOCl (5,12).
EDTA is a chelator that only affects the inorganic content of the smear layer. Thus, the complete removal of the smear layer can only be achieved when the final irrigation protocol must combine EDTA and NaOCl (13).
The irrigating procedure was usually performed with a syringe and needle. In recent years, several new devices have been launched to enhance the agitation of the irrigation solution to facilitate and improve the cleaning and disinfection of the root canal. Passive ultrasonic irrigation (PUI) consists of transmitting energy from an ultrasonically oscillating instrument to the irrigant solutions in the root canal to improve their antibacterial and dissolution properties (9,10,11). Other types of equipment introduced to the field of endodontics include the EndoActivator®, EndoVac®, and Vibringe®, among the most used. Several reports have indicated that the various devices may facilitate the cleaning and disinfection in difficult-to-reach areas, such as isthmuses and secondary canals (14,15). Likewise, the sonic and ultrasonic activation were equally effective in increasing the dissolution effectiveness of NaOCl, up to over ten-fold as compared to passive irrigation (5,11,16). Moreover, PUI and some sonic devices positively influenced the push-out bond strength of epoxy resin-based root canal sealers with dentin (17) and tubular dentin sealer penetration (18).
Effects of the irrigation procedure in the intraradicular dentin
Dentin is a substrate with a complex organic and inorganic structure. This substrate is composed of an extracellular collagen matrix (ECM) with immersed apatite crystals (19). The dentin matrix is a reservoir of non-collagenous proteins (NCPs), which display some biological properties.
Indeed, DMPl and DSPP have previously been described as active promoters and controllers of the biomineralization of dentin (20,21,22). Previously was demonstrated that DSPP and its cleaved products are critical for dentin mineralization, and they may function synergistically with DMPl and the cleaved by-products of both proteins (21).
Apatite deposition among collagen fibrils is a key factor in the regeneration of mineralized tissues (19,22,23,24). Previous data of our laboratory demonstrated that the controlled mineral nuclea- tion on demineralized dentin involves complex molecular signaling that guides the site and rate of apatite formation (22). In a previous study, we reported the ability of a bioactive material to biomi- neralize dentin in a phosphate-containing fluid (25). We hypothesized that the recombinant DMPl molecules could recognize a specific molecular signature on the apatite surface, thereby guiding calcium phosphate clusters during recruitment through the collagen matrix, triggering an ion migration flux and attracting crystal precipitation in a process described as controlled biomineralization (20,21,22,25).
Moreover, our research group demonstrated that the remineralization of radicular dentin can be achieved with the aid of bioactive materials and a standardized demineralization procedure to expose NCPs in the dentin matrix, allowing MMPs to convert structural matrix proteins into signaling molecules and generating peptides, which allows a specific attraction flux of apatites to guide mineral nucleation and maturation (22). Furthermore, our data revealed, for the first time in literature, the migration of the mineral precipitates from their ion source (bioactive material) to dentin, indicating the presence of an attraction flux and specific sites of nucleation in the intratubular dentin (Figure 2) (22).
Nowadays, compelling evidence shows that hypochlorite solutions affect the mechanical properties of dentin via the degradation of its organic components (19,23,24,26). The dentin substrate is exposed to solutions deposited in the root canal during the irrigation protocol. A study showed that irrigation with 5.25% NaOCl, compared to saline solution, reduces the flexural strength and the lastic modulus of dentin (27). Also, the use of NaOCl and PUI induced major changes in the substrate, with intertubular dentin erosion (Figure 3) (24). When dentin collagen is dissolved by NaOCl, the release of oxygen occurs and interfere with the polymerization of resins and adhesive materials (24). Thus, studies reported that NaOCl affected the sealing ability and adhesion of dental materials, such as resin-based cements and root canal sealers, to radicular (28,29) and coronal dentin (29,30).
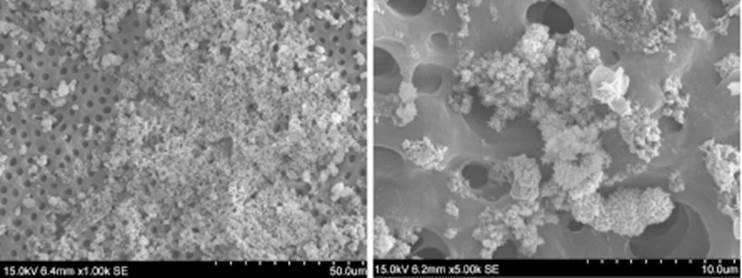
Figure 2 Representative SEM photomicrographs demonstrating the intratubular remineralization of radicular dentin in our previous study (22).
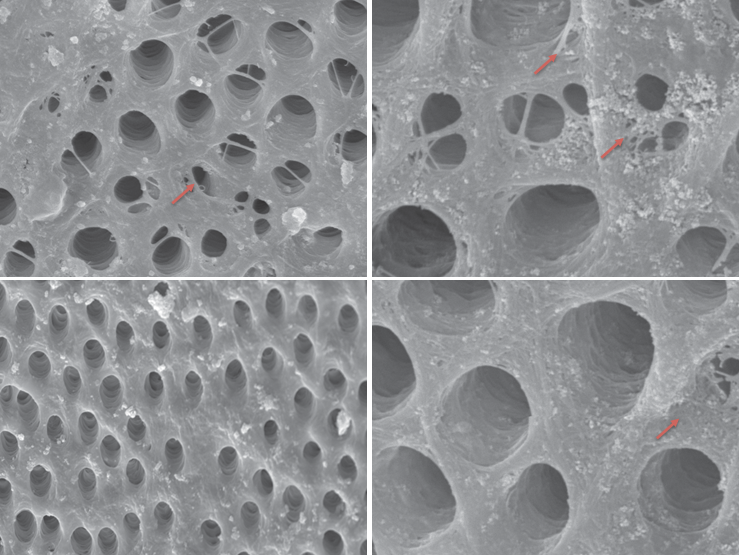
Figure 3 Representative SEM photomicrographs demonstrating the intratubular erosion, pointed out with red arrows, caused by the final irrigation protocol with NaOCl and PUI (19).
Our previous results indicated that the use of most common irrigants affects the expression of MMPs on radicular dentin. NaOCl and CHX cause lower expression of MMPs, while EDTA increases their expression in the root canal dentin (23). Moreover, we demonstrated that the ultrasonic activation of irrigants to obtain better cleaning and disinfection, caused relevant alterations on radicular dentin composition, as well as an important proteolytic effect on DMP1-CT (Figure 4) (19). DMP1 is an essential regulator in regeneration and biomineralization (19,22). The potential loss of this signaling molecule after irrigation procedu- res could affect the dentin matrix as an unsuitable environment for successful regenerative procedures (19).
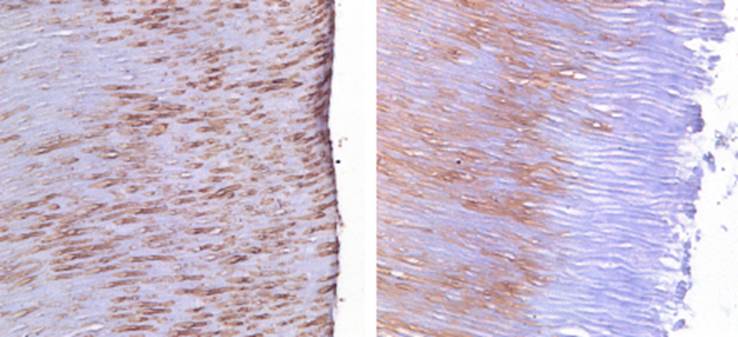
Figure 4 Representative DMP1-CT immunohistochemical photomicrographs. A. Positive control group pattern of normal DMP1-CT spatial distribution in radicular dentin. B. Effect of the final irrigation protocol with NaOCL, EDTA, and PUI showing the detrimental effect on the immunoexpression of DMP1-CT (19).
Most studies that aimed to analyzed the cleaning and disinfection ability of irrigating protocols do not contemplate the effect of the endodontic treatment on enamel and dentin substrates, and how this can be detrimental for the tooth restoration. Irrigation protocols with the most favorable cleaning and disinfection results demonstrated to have a detrimental effect on dentin ultrastructure and biochemical composition.
The clinical relevance of this article remains in alerting to the dental community the alterations that occur in dentin ultrastructure when different irrigation protocols are performed. In clinical scenarios in which is advocated to take advantage of the bioactivity of dentin, for regenerative endodontic treatment and to promote a biomineralization process, it is necessary to ensure that disinfectants do not counteract the function of bioactive molecules (19). For disinfection, lower concentrations of NaOCl are still effective and may preserve more of the protein components in dentin. Development of biocompatible disinfecting solutions is essential to preserve the signaling molecules and maintain a suitable environment when dentin remineralization and/or tissue regeneration are to be achieved. Future research must focus on a balance between biological and mechanical goals for endodontic treatment.

