











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
Periodontal disease (PD) is a chronic inflammatory disease mainly caused by a dysbiotic film which is characterized by the presence of Gram- negative, anaerobic pathogens that colonize subgingival areas and produce significant quantities of pro-inflammatory mediators (1). During pregnancy, periodontal tissues showed an inflammatory response exacerbated due to female sex hormones (2). Periodontal pathogens such as Prevotellaintermedia (P.intermedia), Porphryromonas gingivalis (P.gingivalis), Tannerela forsythia (T.forsythia), Treponema denticola (T.denticola), Fusobacterium.nucleatum (F.nucletum) and Aggregatibacter actinomycetemcomitans (A.actinomycetemcomitans) are abundant in saliva and subgingival biofilms of patients with pregnancy gingivitis (3.4). PD may act as a distant reserve of microbes and inflammatory cytokines that may impact pregnancy and it is believed that they contribute to the early birth induction (5).
Diagnosis of PD is based on the conventional test such as bleeding, probing depth (PD), clinical attachment level (CAL) and bone loss assessed through X-Rays; these traditional diagnosis proce- dures indicate severity but do not identify suscep- tible individuals who may be at risk for future complications (1). In these days, the use of cellular and molecular biology increased in the search for indicators of health or disease with non-invasive techniques to describe the inflammatory condition and predict the progression of the PD.
Therefore, we propose to assess the periodontal bacteria profile from periodontal pockets and the levels of inflammatory immune markers such as Creactive protein (CRP), Immunoglobulin A and G (Ig A and G), nitrite concentration, and myelo-peroxidase (MPO) activity in saliva of pregnant women with PD and to investigate the relation between these biomarkers with the presence of periodontal pathogens, to know if some biochemical markers could be used as tools to reflect the periodontal health status of the pregnant women.
Materials and methods
A comparative descriptive study was carried out, from March to November 2018, of adult women between 21 and 35 years old. We divided the women in two categories: pregnant and non-pregnant. Both of them attended the Dentistry Service of the Provincial Maternal Hospital of the city of Córdoba Dr. Raúl F. Lucini. The following factors were considered for exclusion: smoking, nutrient deficiency, mother's cardiac disease, mother's kidney disease, mother's anaemia, diabetes, hypertension, infection occurring in utero, with TORCH syndrome, immunosuppressed patients, autoimmune disease and metabolic diseases of collagen and bone tissue, multiple pregnancies, and those women who have received periodon- tal treatment and/or antibiotics during the last 6 months, exposure to alcohol, nicotine, anticonvulsant drugs, and teratogenic agents and not overweight for gestational age and with an OHI-S less than three.
This study was approved by the Ethical Committee of the Provincial Maternal Hospital Dr. Raúl F. Lucini, and the Healthcare Ministry of the Government of the Province of Córdoba (RePIS 3065/16). Patients included in this study signed informed consent before their selection to participate in it. Firstly, the patients received a clear explanation of the research trial based on the principles of the Declaration of the Rights of Patients in Clinical Research Helsinki, and the CIOMS standards, the National Habeas Data Law 25326/2000 (Data Protection Act Personal).
Dental examinations
In the dental office of the Hospital Materno Provincial the oral hygiene status was evaluated by the Simplified Oral Index (OHI-S) the OHI-S consists of two components: plaque index (PI) and calculus index (CI), OHI-S= DI+CI (6). Next, all the selected patients were assessed following the criteria of the Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions (1).
We recorded the following clinical parameters: Superior Plaque Index (SupPI), Inferior Plaque Index (InfPI) we observed the presence or absence of dental biofilm andexpressed in percentage of the total number of point examined. Superior and inferior bleeding was recorded as present or absent within 30s after probing with the periodontal probe. The bleeding index (SB) was calculated and expressed in percentage of the total number of sites examined, registered like superior (SB) and inferior (IB). Probing depth (PD) and clinical attachment level (CAL) were assessed in mm in full mouth of all patients with a periodontal probe (Marquis probe Hu-Friedy (Co., Chicago, IL).
Sample taking and biochemistry determinations in saliva
Total unstimulated saliva was collected by spontaneous salivation into sterile tubes (appro- ximately 3ml). Then it was centrifuged for 5min at 3000g (6) and in the supernatant were determined the concentrations of IgA, IgG, high sensitivity C-reactive protein (hsCRP) and myeloperoxidase (MPO) activity using a commercial ELISA kit through immunoturbidimetric assay according to the manufacturer's instructions (Wienner Lab, S.A.), and the nitrite concentration was determined through modified Griess reaction using sulphanila- mide as a substrate (8).
Subgingival plaque sample taking and microbiology analysis
Subgingival plaque samples were taken during the appointment and after taking the saliva sample.The supragingival plaque removed with sterile gauze. A No.40 sterile paper point was then placed to remove bacteria from the upper 2/3 of the bag. Then, to obtain the sample from one site of each sextant with the deepest PD and greatest loss of CAL, five paper points were placed consecutively with a catheterization movement and remained in the pockets for 15 seconds. The specimen-laden paper point was then placed in a capped vial and stored at 4°C until processing (9).To the capped vial containing the paper point impregnated with material from the periodontal pocket, 200µl of saline buffer was added. They were then incubated at 37ºC for 10 minutes and centrifuged at 14,000 g for 5 minutes. To verify the presence of DNA in the supernatant, electrophoresis was performed in 0.8% agarose gel stained with ethidium bromide, which was visualized with UV light (10).
Statistical analysis
Statistical analysis was performed using Infostat vs2008e data analysis software. Significance was defined as p values under 0.05 (p>0.05). A sample size of 100 subjects was needed to provide 80% potency with a confidence interval (CI) of 95% taking into account that the prevalence of the periodontal disease in the local population is 54%. Qualitative variables SupPI, InfPI, ISB, IIB and frequency of periodontal pathogens in the pockets were expressed as absolute and percentages. Quantitative variables were expressed as means and standard deviation. Group comparisons were assessed through the Student T-test, X2 test, Kruskal Wallis test. The relative risk of developing PD was calculated against red-complex bacteria and biochemical variables.
Results
The study population was formed by 100 pregnant women and 50 non-pregnant women, mean age 26.8±5.6 years old, (range 21-35 years).
The two groups of women matched for age, oral hygiene status, bleeding on probing index and pocket probing depths.The mean of the oral hygiene status, in pregnant women, was 4.16±0.03 and 3.2±0.017 for nonpregnant women. The diffe- rence was because the normal gestational inflammation. At the moment of including patients in this study, 21% of the pregnant women were in the first trimester, 47% were in their second and 32% were in their third trimester. Table 1 shows the periodontal clinical parameters of both groups and according to the Consensus report on the Classification of Periodontal and Peri-Implant Diseases and Conditions the diagnosis of periodontitis in the two groups of patients was Stage 1 and A Grade.
The five studied pathogens were identified in the 600 samples collected in subgingival biofilms of pregnant women and 300 samples of non-pregnant women.
Table 2 shows the frequency of identification of each bacterium in relation to the total number of pockets analysed in each group.
It was observed that T.forsythia had different frequencies between pregnant and non-pregnant women. A.actinomycetemcomitans and P.intermedia were not detected in non-pregnant women pockets. Afterwards, periodontal pockets were classified according to the PD as follows: category one up to 4mm and category two from 5 to 7mm and the bacteria distribution were analysed in both categories in each study group (Figure 1).
Table 1 Periodontal variables in pregnant and non-pregnant women.
| - | Pregnant women | Non-pregnant women | p value |
|---|---|---|---|
| PD | 4.26 ± 0.9 | 3.75 ± 1.5 | 0.0045 |
| (mm) | (600) | (300) | |
| CAL | 2.39 ± 1.2 | 3.2 ± 0.8 | 0.047 |
| (mm) | (600) | (300) | |
| SupPI | 97 (56.8-76.6) | 35 (40-59) | 0.105 |
| CI 95% | (100) | (50) | |
| InfPI | 83 (65.7-72.6) | 33 (34-59.6) | 0.049 |
| CI 95% | (100) | (50) | |
| ISB | 68 (0.53-0.62) | 23 (0.36-0.43) | 0.041 |
| CI 95% | (100) | (50) | |
| IIB | 67 (0.54-0.61) | 24 (0.28-0.45) | 0.039 |
| CI 95% | (100) | (50) |
The scores represent means ± standard error; in millimeters of probing depth (PD) and clinical attachment level (CAL), Sup PI Superior Plaque Index, Inf PI Inferior Plaque Index; Plaque Index ISB Index of superior bleeding, IIB Index of Inferior Bleeding: expressed in percentage, between brackets confidence interval at (CI95%). Mean differences in Student T test for CAL and PD and X2 test, for percentages. The significant p-value <0.05, is indicated in bold font.
Table 2 Bacteria frequency in pregnant and non-pregnant women.
| - | Pregnant women | Non-pregnant women | p value |
|---|---|---|---|
| Gram negative. | 415 (0.69) | 150 (0.50) | 0.247 |
| P. gingivalis | 173 (0.42) | 83 (0.55) | 0.074 |
| T.denticola | 225 (0.54) | 97 (0.64) | 0.083 |
| T.forsythia | 316 (0.76) | 36 (0.24) | 0.001 |
| A.actinomycetemcomitans | 8 (0,02) | 0 | -- |
| P.intermedia | 92 (0.22) | 0 | -- |
Numbers show the amount of pockets in which each bacterium was identified, relative frequency between brackets. Differences between proportions were done through Fischer exact test considering a p value of <0.05, is indicated in bold font.
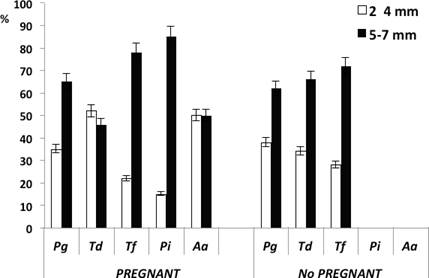
Pg=P. gingivallis, Td=T.denticola; Tf=T.forsythia; Aa=A.actinomycetemcomitan; Pi=P.intermedia. Vertical lines represent percentage errors. The presence of bacteria is expressed as the percentage of sites in which a bacterial species was detected based on the total number of sites studied.
T.forsythia was identified as the most frequent bacteria in 5mm pockets in non-pregnant women and P.intermedia was identified in deep pockets in pregnant women. T.denticola decreased the frequency in 2-4mm deep pockets from pregnant women, while in the same pocket deepness of non-pregnant women P.gingivallis, T.denticola and T.forsythia increased frequencies.
To elucidate whether the differences observed in Table 3 were related to characteristics of the pregnancy, the patients were classified according to the trimester of pregnancy in which they were at that moment of integrating the study and associa- ted the studied variables which were statistical differences between pregnant and non-pregnant women. Results are shown in Table 4.
We observed that CAL increase in pregnant women in the third trimester compared with the women in the others trimester (p=0.02). Besides, in the same women, we observed a significant decrease in the level of IgA in saliva. We did not observe differences in Ig G and MPO in the saliva of the women among the different trimesters. T.forsythia and P.intermedia (p=0.045) were identified more frequently in pregnant women in their 3rd trimester, as well as we detected a linear correlation between the presence of P.intermedia and CAL (Pearson coefficient of 0.78) and for T.forsythia and CAL (Pearson coefficient 0.94 p=0,013).This positive correlation would indicate that, the increase in CAL may be caused by a greater presence of T.forsythia and P.intermedia in periodontal pocket. We did not observe any type of correlation between other variables.
It is known that P. gingivalis, T. denticola and T. forsythia trigger the PD, so we classify the perio- dontal pockets according to they had Pg+Td+Tf and such pockets were associated with each biochemical variable in pregnant and non-pregnant women. Table 5 shows that in pregnant women the high IgA level in saliva (p=0.03), when is the presence Pg+Td+Tf in pockets. In non-pregnant women, the MPO activity is higher in the presence of the bacterial triade (p=0.046).
In summary, P.intermedia and T.forsythia were the most frequent bacteria detected in 5-7 mm periodontal pockets in pregnant women (Figure 1) and the presence of these two bacteria was statistically associated with the IgA levels in saliva and CAL.
Table 3 Biochemical parameters in saliva from pregnant and non-pregnant women.
| - | Pregnant women (100) | Non-pregnant women (50) | t | p value |
|---|---|---|---|---|
| Ig A (mg/dl) | 65.9 ± 11.3 | 38.4 ± 9.1 | 2.03 | 0,013 |
| Ig G (mg/dl) | 82.53 ± 21.2 | 53.0 ± 10.3 | 1.17 | 0,045 |
| hsCRP (mg/dl) | 3.58 ± 0.27 | 3.14 ± 0.08 | 1.4 | 0,165 |
| Nitrites (µM/ml) | 10.68 ± 3.58 | 17.06 ± 10.1 | -1.37 | 0.174 |
| MPO (UI/ml) | 39.53 ± 15.04 | 88.2 ± 73.9 | -2.34 | 0.018 |
Values represent the mean ± standard error. IgA: Immunoglobulin A, Ig G: Immunoglobulin G, hsCRP: high sensitivity C-reactive protein, MPO: Myeloperoxidase, Student T test p<0.05, is indicated in bold font.
Table 4 Periodontal and biochemical parameters according to the pregnancy trimester.
| - | CAL mm | PD mm | Ig A (mg/dl) | Ig G mg/dl | MPO (UI/ml) | T.forsythia % (CI) | P.intermedia % (CI) |
|---|---|---|---|---|---|---|---|
| 1st T (21) | 2.2 ± 1.6 | 4.3 ± 0.6 | 78.9 ± 7.6 | 68.9 ± 5.5 | 31 ± 10.2 | 24 (17-32) | 16 (10-23) |
| 2ndT (47) | 2.3 ± 1.4 | 4.1 ± 0.6 | 72.2 ± 4.3 | 63.6 ± 13 | 32 ± 11 | 43 (11-19) | 19(15-24) |
| 3rd T (32) | 3.1 ± 1.2 | 4.3 ± 0.9 | 44.1 ± 2.6 | 78.1 ± 5.5 | 37.5 ± 12.2 | 61(25-38) | 33(26-39) |
Values are the mean ± standard error for CAL, PD, Ig A, Ig G, and MPO and % to T.forsythia and P.intermedia. T: trimester of pregnancy (N), PD: Probing depth, CAL: Clinical attachment level in millimetres, IgA: Immunoglobulin A, Ig G Immunoglobulin G, MPO Myeloperoxidase. indicate significative difference (p<0.05) by Chi square test to bacterial proportions and ANOVA to quantitative variables.
Table 5 Relationship between biochemical parameter levels in saliva and presence of red complex bacteria in periodontal.
| - | - | Pg+Td+Tf = 0 | Pg+Td+Tf = 1 | p value |
|---|---|---|---|---|
| Ig A (mg/dl) | PW | 53.6±35 (170) | 77.42±69.3 (290) | 0.03 |
| - | NPW | 43.12±23 (60) | 34.98±10.4 (80) | 0.98 |
| MPO (UI/ml) | PW | 36.14±46.7 (170) | 24.24 ± 65(290) | 0.85 |
| - | NPW | 24.92±25 (60) | 135±171(80) | 0,046 |
Pg=P.gingivalis; Td=T.denticola; Tf=T.forsythia; Pg+Td+Tf=0: periodontal pockets without these bacteria; Pg+Td+Tf=1 periodontal pockets with these bacteria. Values represent the mean ± standard deviation. The method used was Kruskas Wallis with a p value <0.05, is indicated in bold font.
Discussion
Different authors described changes in the bacteria composition of biofilm during pregnancy (11,12,13,14). In this study, we detected a higher proportion of T.forsythia and P.intermedia in perio- dontal pockets from-pregnant women. It is well known that these pathogens may migrate to other tissues; periodontal bacteria have been isolated in the amniotic fluid of pregnant women (15,16, 17). The combinations of spread bacteria through the bloodstream and inflammatory mediators that are formed in periodontal tissues seem to be the mechanism that compromises the foetal-placental unit and would represent a risk factor for adverse pregnancy outcomes (18,19).
Moreu et al. recorded periodontal clinical data of 96 pregnant women during their first, second and third trimesters and concluded that periodontal disease was a risk factor for low-birth- weight children (OR 1st trimester: 0.81; OR 2nd trimester: 1.08; OR 3rd trimester: 1.99) (20). In our study, we were observed that patients in their third trimester presented a high CAL, a decrease in IgA level and an increase in T.denticola y T.forsythia identification. In a consecutive and prospective study, Adriaens LM et al. informed the major changes in microbial levels occurred between weeks 28 and 36 of pregnancy (3°trimester for us) (21). These data may indicate that in the 3° trimester the periodontal conditions could deteriorate when the pregnant has not been treated for chronic periodontitis. A study observed that levels of 17 of 37 species analysed by checker- board DNA-DNA hybridization, decreases during a normal pregnancy. Nevertheless, subgingival levels of A.actinomycetemcomitans, P.gingivalis, T.forsythia, and T.denticola did not change and the observed that at week 12 of pregnancy and elevated levels of P.gingivalis and T.forsythia were associated with BOP (22).
Recent studies on massive sequencing have shown that some bacteria species increase in number in oestrogen rich environments which supports the idea that oestrogens have an impact on their colonization (23). This idea is supported by the sample analysis of supragingival plaques of pregnant and non-pregnant women during the 1st, 2nd and 3rd trimesters of pregnancy and the postpartum period. Results showed that Neisseria, Porphyromonas y Treponema were higher in pregnant women. Moreover, it was shown that there are significantly higher bacteria diversity in pregnant women during their third trimester (22). Therefore, it seems that hormones during pregnancy boost the differences in the composition in pregnancy, especially during the third trimester where progesterone in saliva and estradiol increase compared to the first trimester (22). In another study, it was shown that T. forsythia was the only bacteria detected in placenta samples of women who delivered early and underweighted children when born. Such bacteria are related to deep periodontal pockets (24). Such data coincide with the results of this study in which a variety of bacteria species were detected in periodontal pockets in pregnant women and a higher frequency of T.forsythia during the third trimester of pregnancy.
In this study, there were no differences between groups as regards hsCRP activity in saliva. However, there is a slight increase in pregnant women, but it is not significant. hsCRP is synthesized by the liver and it is a systemic marker released during an acute stage of an inflammatory response (25). It is higher in saliva in people with chronic or progressive and in pregnant women with periodontal disease (26,27). In this study most patients in both groups were diagnosed with stage I and II periodontitis, therefore PD could not have triggered the inflammatory response sufficient to increase salivary hsCRP levels.
Madianos et al. found that high IgG levels against certain oral bacteria in the mother's serum can be related to a lower early birth rate and an increase in the weight of the newborn. This suggests that the antibody has a certain protective capacity (27). It was reported in a study that patients with PD presented high serum and saliva IgG levels against A.actinomycetemcomitans compared to healthy patients. Furthermore, they demonstrated that elevated hsCRP was a negative predictor of high levels of IgG titers against A.actinomycetemcomitans in serum and saliva (29,30).
As a result of the neutrophil extravasation in deep pockets containing bacteria, it was found that there is an increase of MPO activity in non-pregnant women with the presence of P. gingivallis, T.denticola and T.forsythia in periodontal pockets.Taba et al. related the increase in MPO activity with progressive periodontal destruction (31). It is suggested that such increase is due to the abnormalities in the apoptosis of neutrophils that lead to the accumulation of MPO that has as a consequence the subsequent destruction of the connective tissues which leads to a risky periodontal state (30).
Conclusion
In this study, it was observed that pregnant women in their third trimester had a higher CAL, low IgA levels (p=0.047) and presence of T. denticola and T.forsythia (p=0.013) in deep pockets than pregnant in other trimesters. This environment may constitute a complex and risky situation since the presence of these two bacteria would allow the access of other bacteria species and aggravate the PD. The IgA levels in saliva may reflect the immune situation during pregnancy. This could be used to monitor the immune state of gingival tissues during pregnancy.
Author contribution statement
Conceptualization and design: M.M.U. and A.S.
Literature review: A.S. and M.M.U.
Methodology and validation: S.T.
Formal analysis: S.T.
Investigation and data collection: N.S., L.S. and C.R.
Resources: N.S. and S.T.
Data analysis and interpretation: M.M.U., L.S. and N.S.
Writing-original draft preparation: N.S.
Writing-review & editing: A.S.
Supervision: M.M.U.
Project administration: A.S.
Funding acquisition: A.S. and M.M.U.

