











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
1. Introduction
According to the World Health Organization (WHO), violence can be defined as “the intentional use of physical force or power, threatened or actual, against oneself, another person, or against a group or community, resulting in or likely to result in injury, death, psychological harm, maldevelopment or deprivation” (WHO, 2014). This complex phenomenon affects individuals of different genders, ages, ethnicities and social classes, being considered an important public health problem in Brazil and in the world (Mascarenhas et al., 2021).
Violence can take different forms according to its nature, and can be classified as physical, sexual, emotional, psychological, interpersonal, self-inflicted and/or patrimonial (Mendonça et al., 2020). Despite the particularities inherent in each of these scenarios, violence in general represents one of the main causes of hospitalizations in Brazil, with records of, on average, 40,000 homicides per year between 1980 and 2019, accounting for 15.3 % of all murders in the world in 2016 (Kopittke & Ramos, 2021).
This true epidemic of violence associated with the inability of the government to manage it efficiently (Kopittke & Ramos, 2021), results in catastrophic social, economic, epidemiological and individual impacts, such as physical sequelae, depression, alcohol abuse and others drugs, death, among others (Mascarenhas et al., 2021). This situation, in turn, implies high public spending, immeasurable individual suffering and reduced social cohesion, contributing to the reduction of productive capacity and stigmatization of social groups (Corrêa et al., 2021; Mendonça et al., 2020).
Given the complexity and multicausality of this phenomenon, its approach and confrontation require expanded knowledge about its extent, characteristics and consequences (Souto et al., 2017). It is in this context that the Brazilian Ministry of Health, through the Health Surveillance Secretariat (SVS), implemented the Violence and Accident Surveillance System (VIVA), which systematizes data from notifications, allowing the recognition of the magnitude and severity of this problem (Ministério da Saúde, 2011).
Based on data from this system, it becomes possible to optimize the understanding of the dynamics of aggression, exposing the biopsychosocial particularities of the aggressors and victims, as well as the circumstances associated with the occurrences and subsequent forms of management, allowing the characterization of a profile of vulnerability. This, in turn, can serve as a theoretical subsidy for the planning and implementation of government policies and actions necessary to face and prevent this disease and its disastrous consequences. (Mascarenhas et al., 2021; Souto et al., 2017)
Therefore, the objective of the present study is to characterize the main indicators and the way in which they are associated with violence in Brazil according to their forms, means and circumstances of occurrence, based on data from the Information System of Notifiable Diseases of the Brazilian Ministry of Health in the period from 2011 to 2020.
2. Metodology
2.1 Approach
This study presents an analytical quantitative approach on violence data recorded by the Department of Informatics of the Unified Health System (DATASUS). The supply of this system is carried out, predominantly, through notifications and investigations of diseases of compulsory notification, according to national determinations (Ministério da Saúde, 2020).
2.2 Study population
The study population consisted of all reports of physical, self-inflicted or not, psychological and sexual violence recorded by DATASUS between 2011 and 2020 in Brazil. Incomplete data or the absence of parameters of interest were established as exclusion factors, being selected all the cases in which the presence of information regarding the characteristics of the aggressor, socioeconomic determinants related to the victim and elements referring to the place of occurrence were observed.
2.3 Collection techniques
Data collection took place at the beginning of 2022 through the DATASUS File Transfer System, supplied by individual notification/investigation forms on domestic, sexual and/or other forms of violence from the Notifiable Diseases Information System (SINAN), in which symptomatological and sociodemographic information related to the reported cases are collected.
The variables used, as established in the notification forms, were: age, gender, race/color, education, marital status (CC) and the presence of deficiencies and/or disorders, of a physical, mental, visual, hearing or behavioral nature, as far as victims are concerned. In addition, the macro-region of occurrence will be evaluated, the possibility of being a recurrence and the type of violence reported, which in the present study can be physical (self-inflicted or not), sexual or psychological. As for the characterization of the perpetrator of the violence, age, sex and the possibility of using alcohol were analyzed.
2.4 Analysis processing
The RStudio program was used for processing and tabulating the data, as well as performing the analysis procedures in R language. At first, univariate statistical analyzes were carried out in the database.
The pre-selection of variables was based on paired analyzes of chi-square tests, eliminating all those that did not show evidence of association with at least one of the others. The selected set was used to feed a Multiple Correspondence Analysis (MCA) and for a better understanding of its results, the Hierarchical Clustering technique was used, having as a final result the production of a dendrogram based on the total inertia of the system.
Finally, it is worth pointing out that the data used in the present study are in the public domain and have a secondary nature, thus submitting it for consideration by the Research Ethics Committee is dispensable (Guerriero, 2016).
3. Results
An average of 335,277.30 (±74,455.78) cases of violence were recorded per year, of which 155,490.80 (±29,878.21) cases corresponded to physical form, with 55,913.20 (±23,518.71) being the records of self harm. The psychological and sexual forms presented annual averages of 61,056.90 (±10,418.34) and 31,703.20 (±5,686.44) notifications, respectively.
Regarding the spatial stratification of the phenomenon, there was an important participation of the Southeast region of Brazil in the notifications of all forms of violence. In Figure 1, it is possible to observe how the relative participation of each region occurred in the national notifications for each of the analyzed forms of violence.
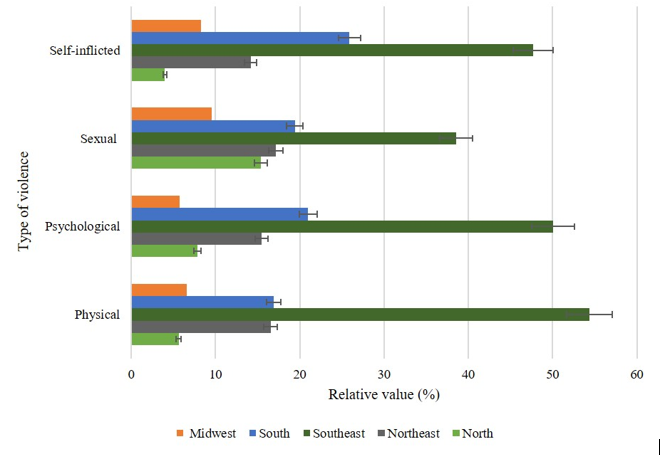
The authors, 2022
Figure 1 Distribution of cases of violence in Brazil, according to region and type of violence, reported in the Information System for Notifiable Diseases (SINAN)
The analysis of the notifications regarding the sex of the victim showed the predominance of the female population. Of the cases of physical violence, 71.53 % (±14.40) had female as victims. In the notifications referring to self-harm, this value becomes 68.39 % (±15.29). For the psychological and sexual forms, 83.94 % (±9.53) and 87.83 % (±7.56) of the total, respectively, have the female population as victims.
With regard to the ethnicity of the individuals who were victims of violence, most of the records corresponded to whites or browns. In Table 1, it is possible to observe in greater detail the relative value of cases by ethnicity according to the type of violence reported.
Table 1 Distribution of cases of violence in Brazil, according to race and type of violence, reported in the Notifiable Diseases Information System (SINAN).
| Type of violence | Color/Race | ||||
| White | Black | Yellow | Brown | ||
| Self-inflicted ( %) | 54.13 | 7.14 | 0.78 | 37.96 | |
| (±0.14) | (±0.07) | (±0.02) | (±0.13) | ||
| Physical ( %) | 44.86 | 9.84 | 0.82 | 44.48 | |
| (±0.08) | (±0.05) | (±0.02) | (±0.08) | ||
| Psychological ( %) | 46.30 | 10.41 | 0.78 | 42.51 | |
| (±0.13) | (±0.08) | (±0.02) | (±0.13) | ||
| Sexual ( %) | 40.29 | 9.85 | 0.81 | 49.05 | |
| (±0.18) | (±0.11) | (±0.03) | (±0.18) |
The authors, 2022
With regard to the victims' schooling, the notifications corresponded predominantly to individuals who had between the fifth grade of elementary school and complete high school. Other information regarding the victims' schooling can be seen in Figure 2.
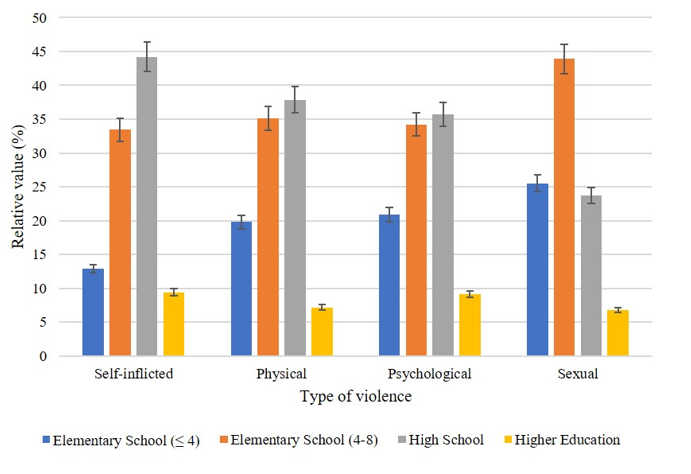
The authors, 2022
Figure 2 Distribution of cases of violence in Brazil, according to schooling and type of violence, reported in the Notifiable Diseases Information System (SINAN)
The use of alcohol by the aggressor was found in 43.71 % (±17.39) of the records of physical violence. In cases of self-inflicted violence, this value becomes 21.79 % (±12.05) of the total number of notifications. For occurrences involving psychological and sexual violence, there are respectively 44.38 % (±17.45) and 33.40 % (±15.73).
Recurrences corresponded to 62.38 % (±16.59) of reports of psychological violence and 47.17 % (±17.62) of records of sexual violence. For physical violence, this value becomes 46.11 % (±17.57) and 47.47 % (±17.63) when only cases of self-harm are considered.
With regard to the ages of those involved, the predominance of adult individuals was noted as the main aggressors in all forms of violence analyzed. As for the age of the victims, in the modality of sexual violence there is a predominance of individuals aged between 0 and 20 years, for physical violence and self-harm the age group with the highest occurrence corresponds to the interval between 10 and 29 years. For cases of psychological violence, there is a significant participation of the group between 10 and 39 years old. More details regarding the ages of victims and aggressors can be seen in Table 2.
Table 2 Distribution of cases of violence in Brazil, according to the ages of victims and aggressors according to the type of violence, reported in the Notifiable Diseases Information System (SINAN)
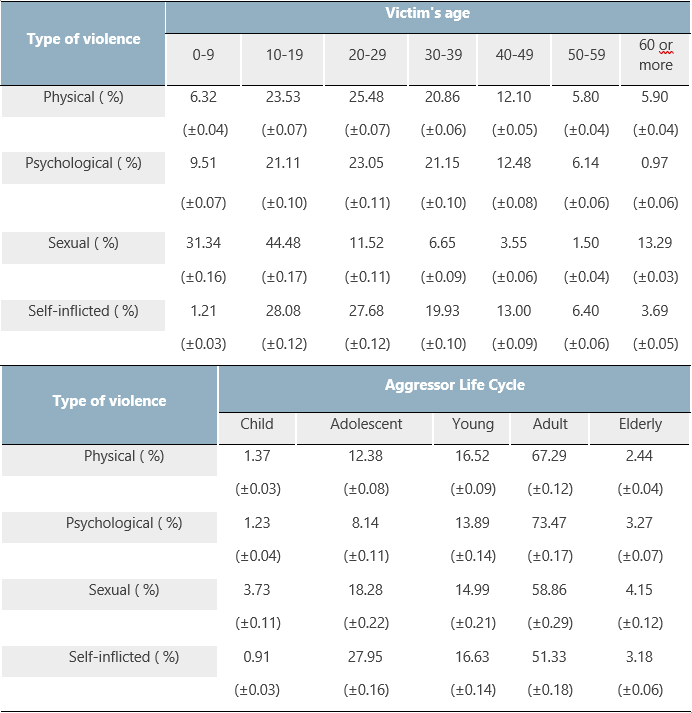
The authors, 2022
The MCA of the study variables generated a result composed of 17 categories, of which the two that managed to capture the largest portions of inertia of the system were used for the construction of a two dimensional perceptual map. The organization of the influencing factors according to the total inertia explained by the most important dimensions can be seen in Figure 3.
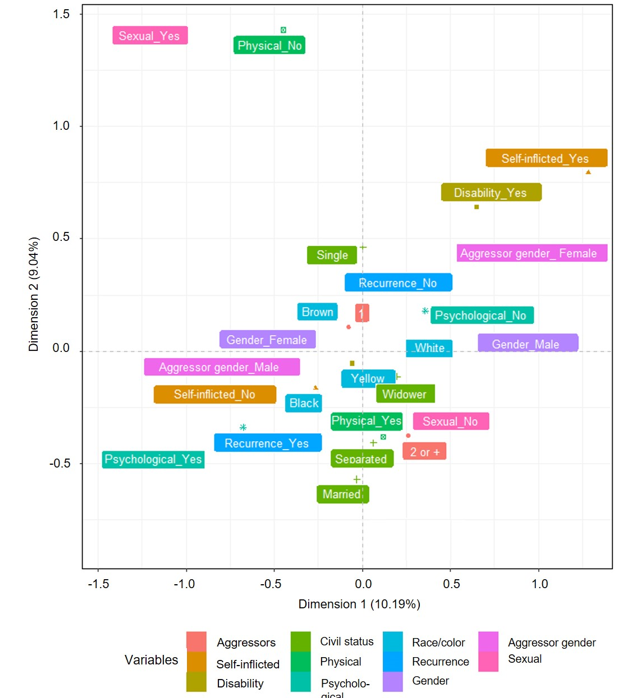
The authors, 2022
Figure 3 Perceptual map of cases of violence in Brazil, reported in the Notifiable Diseases Information System (SINAN)
In order to consider the totality of the inertia explained through the results of the ACM, we used the hierarchical clustering technique based on the Euclidean distance of the variables according to the data recorded in the 17 dimensions. The results of the clustering performed can be seen in the dendrogram represented in Figure 4.

4. Discussion
The present study exposes violence as a chronic Brazilian public health problem and reinforces the need for constant updating on the characterization of the epidemiological profile of victims and aggressors to guide the establishment of timely mitigation measures.
Regarding the forms of aggression, the physical modality stands out on the national scene (46.4 %), which can be related to the greater ease of recognition of victims due to the direct impact on individual physical integrity, a context different from other forms of violence, such as psychological and sexual, which can be practiced by close individuals in presumably safe environments without leaving physical marks, contributing to underreporting (de Sousa et al., 2016).
Notoriety can also be attributed to psychological violence, a modality that is difficult to recognize and that can manifest itself in different ways, such as blaming the victim for various events, threats, lack of support, abandonment, restriction of freedom, insults and humiliations (Pires et al., 2017). The high prevalence of this form can be explained by its close association with everyday interpersonal relationships, a fact that creates a veiled environment for the perpetuation of these aggressions, sometimes associated with other types of violence (Mascarenhas et al., 2021; Pires et al., 2017).
As for geographic distribution, the highest number of notifications was observed in the Southeast region. This result can be partially explained by the disproportionate Brazilian demographic distribution, after all, according to estimates, this region has 89,012,240 inhabitants, which represents 42.0 % of the national population (Instituto Brasileiro de Geografia e Estatística [IBGE], 2020).
However, according to Mascarenhas et al. (2021), another justification would be the fact that the search for care and the complaint after the aggression are significantly higher in the Southeast region, that is, the probability of notification and arrival of these cases to public databases is higher in this part of the country. This could be evidenced by Taveira & de Oliveira (2020), who showed that the highest number of complaints on Dial 100 between 2011 and 2015 came from the Southeast region (42.27 %).
Regarding the sex of the victims, there was a significant predominance of females in all forms of violence studied here. Also noteworthy is the proximity in the dendrogram between this factor and the male category for the sex of the aggressor. The genesis of this scenario maintains a strong relationship with the socioeconomic, political and cultural structures that, historically, reinforce and perpetuate gender inequality and male supremacy (Mascarenhas et al., 2021).
Traditionally, gender relations assume an asymmetrical and discriminatory character, where the male figure carries a strong symbology of power, domination and submission, alien to their desires and interests (Souto et al., 2017). Thus, the patriarchal and sexist predetermination of social roles naturalizes the perpetuation of violence against women, often associated with blaming the victim, passivity of justice bodies and, consequently, underreporting (Souto et al., 2017; Teixeira & Paiva, 2021).
Also, with regard to female victims, the relationship observed in the dendrogram with the modality of self inflicted violence is remarkable. The understanding of this type of occurrence is endowed with great complexity and there are strong influences of psychosocial determinants in these contexts that should not be neglected. Not necessarily, in cases of this nature, the objective is death, however studies estimate relapse rates between 20 and 30 %, of which death is observed in 10 % (Souza et al., 2014; Sinimbu et al., 2016).
This situation is responsible for undeniable damage to women's health, such as physical sequelae, psychological disorders, suicide attempts, drug abuse and unemployment, with direct repercussions on their autonomy, self-esteem and family structure (Netto et al., 2014; Teixeira & Paiva, 2021). In this way, the need for training of multidisciplinary health teams to recognize these cases of violence, welcoming victims, promoting active listening, offering physical and psychological care, as well as case notification is reinforced (Teixeira & Paiva, 2021).
As for ethnicity, there was a predominance of cases among white and brown individuals, a scenario justified by the Brazilian ethnic composition in which 42.7 % and 46.8 % of the population declare themselves, respectively, white and brown (IBGE, 2019). However, it is important to be careful when interpreting racial data from public databases, after all, they come from self-declarations, which may disagree with the individual's true ethnic origin (da Mata, Daltro, & Ponde, 2020).
There was also a relationship between the low schooling of victims and cases of violence in this study and in the literature (Mascarenhas et al., 2021; Guimarães & Villela, 2011), however the discussion about this association is still controversial. The lower level of education may reflect structural violence, characterized by social inequality, exclusion and deprivation of citizenship, which implies financial difficulties, family breakdown and, in turn, aggressive behavior (Dossi et al., 2008; Gomes et al., 2006; Guimarães & Villela, 2011). Even the low level of education of parents also showed a strong relationship with hospital admissions of adolescents due to violence, and is therefore considered a risk factor among disadvantaged families (Remes et al., 2019).
However, the higher prevalence of violence in this population with less education can only be justified by the fact that less disadvantaged individuals tend to report more problems that are usually hidden among more favored classes (Dossi et al., 2008). Furthermore, the low level of education may reflect only the young age group of the victims.
When evaluating the profile of the aggressor, alcohol use was found in a large number of cases, which allows us to recognize this practice as an important modifiable risk factor for violence (Souto et al., 2017). This substance, through its psychoactive and disinhibitory effect, corroborates the loss of critical sense, increased aggressive behavior, cognitive distortion, attention deficit and neurochemical changes, a fact that contributes to the genesis and maintenance of violent behaviors (Queiroz et al., 2021).
It is also worth noting that, in the long term, chronic alcohol consumption can lead to sleep deprivation, withdrawal crises and impairment of neuropsychic functioning, a conjuncture favorable to the perpetuation of aggressive and unpredictable behavior (Queiroz et al., 2021). This situation reinforces the need for a partnership between government, education and health sectors to implement actions aimed at mitigating the risks and losses, whether individual or collective, of alcohol consumption (Priotto & de Moura, 2020).
In the dendrogram, the relationship and proximity between recurrence and cases of psychological violence are notorious. According to Mascarenhas et al. (2021), the recurrence of violence presupposes close contact with the aggressor, who can be a family member, a resident of the household and even the intimate partner.
By characterizing psychological violence as any action that threatens or harms an individual's self-esteem, identity or development, it is understood that it can be considered as part of everyday interpersonal relationships (Mascarenhas et al., 2021; Pires et al., 2017). Therefore, everyday facts, such as cleaning and organization of the house or the divergence regarding the distribution of domestic activities, may be enough to trigger psychological aggressions among those involved (Dossi et al., 2008).
This frequent coexistence as a result of habitual relationships, added to the desire to maintain the marital relationship in favor of family cohesion and the education of children, causes, for example, the perpetuation of psychological violence suffered by women who are exposed to verbal and emotional abuse of their partners (Mascarenhas et al., 2021; Sediri et al., 2020). In fact, this study reinforces this relationship due to the proximity between psychological violence and married individuals.
Regarding sexual violence, the victim's house is pointed out in the literature as a preferred place for the practice of abuse, especially when the victims are children. This fact demonstrates that the aggressors have free access to the interior of the residence or are family members, who, for the most part, are dominant male figures in the family dynamics (Guimarães & Villela, 2011; Walker-Descartes et al., 2021). In some cases, the fear that the complaint may negatively affect the well-being of the home and the child itself makes them remain silent, also facilitating the recurrence of aggression (Walker-Descartes et al., 2021).
On the other hand, self-inflicted violence has a higher occurrence among adolescents and adults. An example of this is self-mutilation, which can be conceptualized as an intentional act of tissue destruction with the objective of materializing emotional pain into physical pain. This practice is quite prevalent among adolescents, which can symbolize from an adaptation to the changes experienced at this stage of life, to mental disorders with possible reflections on the development of these individuals (Rissanen et al., 2011). Regarding the reasons that motivate self-harm in adults, emphasis is given to financial difficulties, affective reasons such as relationship breakup, as well as causes related to profession and family pressure (da Silva et al., 2021).
It is worth mentioning the importance of the work of health professionals in terms of recognizing patients with self-destructive profiles, in order to offer necessary interventions and comprehensive care to the individual to prevent the recurrence of violence. This is because, as in the present study, national findings indicate that approximately one third of suicide attempts are repeated within a year (da Silva et al., 2021).
Violence affects one in five Brazilian adults (Mascarenhas et al., 2021) and the victims are mostly adults and adolescents, however, when stratified by type of violence, children are also an important part of the victims of sexual violence. This demonstrates the vulnerability and greater susceptibility to violations of the rights of this group, since they depend on basic care (Lugarinho et al., 2017).
Children are at risk in the community, in schools, in technology, and even within their own home. Some family factors such as stress attributed to poverty, absent or single parents, low parental education, alcohol or toxic substance abuse are risk factors for child sexual violence. Furthermore, the introduction of technology in the daily life of this public maximizes the opportunities for exploitation by the aggressors, as it facilitates contact with children, at the same time, it is configured as a means of accessing explicit sexual content (Walker-Descartes et al., 2021).
Adolescence is characterized as a more critical and stressful period of an individual's life due to physical, psychological and social changes, in addition to the transition to high school, conflict with parents and the polarities between fear and courage (Lugarinho et al., 2017). In addition, the present study demonstrated that Brazilian adolescents are subject to all types of violence which, in turn, can cause biological, emotional and cognitive damage and, therefore, impact the development of these individuals (Lugarinho et al., 2017).
An association has even been observed between chronically altered hormone levels during a stressful situation and deficits in brain structures, damage to the autoimmune system, in addition to a greater vulnerability to the development of mental and physical diseases. This scenario makes this issue a social problem that needs to be studied and prevented not only in this age group, but in the population as a whole (Lugarinho et al., 2017).
Finally, the profile of aggressors is still little explored, but no less important than understanding the characteristics of the victim and the consequences arising from violence (Kadiani et al., 2020; Minayo & Mariz, 2021). Most of the aggressors are men, young people and adults, black and brown and with low education (de Souza et al., 2021; de Souza Melo et al., 2021; Kadiani et al., 2020; Minayo & Mariz, 2021). Generally, factors such as alcohol dependence, psychiatric comorbidities, diverse and traumatic experiences in childhood, make people more susceptible to becoming perpetrators of violence, however, this subject is trivialized and the aggressors are only called “bad people” (Kadiani et al., 2020). Findings of the present study corroborate the literature, since the male sex as aggressor predominates in most types of violence that occur in the country.
Among the limitations of the study, we highlight the use of secondary data that may not fully reflect the Brazilian reality due to possible underreporting or incorrect and incomplete filling of information, in addition to not allowing to extrapolate certain more detailed analyzes on the investigated topic.
5. Conclusion
Violence is characterized as a complex and multicausal phenomenon, which results not only in high public spending, but mainly in the reduction of social cohesion due to the immeasurable damage caused to the
population involved. In the present study, the violence is mostly of the physical type, affecting adult males, with low schooling and white or brown. Recurrence occurs mainly when the violence is psychological and sexual. As for the aggressor, they are usually adults, male, and the use of alcohol is common.
This characterization of the epidemiological profile of victims of violence provides subsidies to guide the planning and implementation of measures to prevent and cope with this chronic Brazilian public health problem. Also, the discussion of this theme, based on the quantitative and qualitative analysis of the notifications registered in SINAN, puts in vogue the magnitude and severity of the problem that must be investigated regionally and in a segmented way according to the type of violence. Thus, it infers that spending on violence prevention can mitigate economic, social and psychological problems in Brazil.

