











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Weiner et al. (1998) hypothesized that people with HIV/AIDS are perceived as being in control of their infection and thus blamed for it. It is most likely the social fabric that sustains such perceptions and HIV-related stigma. Stigma is defined as the social process of identifying a person or a group of people as inferior or less valuable based on specific features (Link & Phelan, 2001). Getting infected with HIV may prompt this type of social rejection. People living with HIV are regarded by most as, if not at fault, being at least responsible for getting infected. Consequently, they are subject to reprimand, anger, and hostility.
Nevertheless, researchers have found that people react differently to individuals infected with HIV depending on how they contracted the infection. For example, Graham et al. (1993) found that people who became infected due to drug use and needle sharing evoked considerably more anger and less sympathy than those who got infected through blood transfusions. The attribution model can explain those different reactions (Heider, 1958; Dela Coleta, 1982). When people attribute the cause of a disease to external factors - i. e., factors that the individual cannot control - they tend to feel sympathy for the person. Nonetheless, when people perceive a disease as being caused by an individual’s direct actions, they tend to blame them and feel anger towards them (Mantler et al., 2003). In a recent Brazilian study, researchers tried to investigate such attributional differences. An experiment was conducted on a sample of university students from the healthcare field and healthcare professionals from Porto Alegre (Brazil) to identify if causal attributions changed in different infection scenarios (Azevedo, et al., 2020). The present study aims to replicate the Brazilian experiment in a German sample. We aim to investigate if blame still plays a role in the perception of HIV-infected people according to the attributional model and to analyze the association between causal attribution, willingness to help, and emotional reactions. Moreover, one of the objectives of this study is to compare control, responsibility, blame attributions, emotional reactions, and the willingness to help heterosexual, homosexual, and transgender women in scenarios of HIV infection due to blood transfusion and unprotected sex.
Attributional Theories
According to attributional theories, people tend to find explanations for what they see. An attribution is an explanation about something (Heider, 1958). By finding meaning for the events that occur, people feel they can foresee what will happen (Dela Coleta, 1982). If someone’s attribution for skin cancer is “people get skin cancer because they do not wear sunscreen”, they will most likely think that wearing sunscreen prevents skin cancer. However, while individuals may seek reasoning for their and others’ behaviors, their explanations are not always logical. Attributions have a biased logic. They are generally based on an individual’s own experiences (Dela Coleta & Dela Coleta, 2006; 2011).
As conceived by Weiner, seeing people as judges and life as a courtroom is a guiding metaphor in attributional theories. This notion conforms to the central thesis of Weiner’s attributional framework, in which the perceived causes of a given event, especially locus and controllability, are associated with moral beliefs, inducing inferences about an individual’s responsibility for the event. The perception of responsibility is related to moral emotions, such as anger or sympathy, and associated with willingness to help versus aggression. Thus, Weiner (2006, p. 43) states that moral beliefs are significant guiding judges of events, prompted by concepts such as “sickness versus sin” and “good versus evil”.
Attribution of responsibility is usually influenced not only by an individual’s personal thoughts and emotions but also by cultural features (Steins & Weiner, 1999). Therefore, responsibility attribution differs within collectivist and individualist cultures. In contrast to individualist countries, such as Germany, in collectivist countries, such as Brazil (Hofstede, 2001), compassion tends to play a more significant role in responsibility attribution (Levine et al., 2001).
The attributional framework has been applied for study in different areas, such as school-related issues, marital distress, communication with consumers, and reactions to others with physical health problems - as is the case in the present study. Weiner (2006) hypothesizes that the dissemination of such a framework may help reduce discrimination against ill patients. If healthcare professionals do not see their patients as responsible for getting sick, they will sympathize with them rather than reject them (Weiner, 1995; Crandall & Moriarty, 1995).
Mantler et al. (2003) made another elaboration on the attributional model. The authors address some concepts introduced in Alicke’s (2000) culpable control model regarding blame. Mantler et al. (2003) stress inconsistent results concerning distinctions between controllability, responsibility, and blame. According to these authors, it was unclear whether controllability, responsibility and blame judgments differ systematically in response to negative events. They assumed sequence judgments varied between controllability-responsibility-blame, guiding a decision-stage model impacted by pre-existing attitudes, as formulated by Heider (1958), Weiner (1995), or Shaver (1985).
To investigate the sequence proposed and the influence of pre-existing attitudes regarding this sequence on emotions, willingness to help, and social contact, the authors studied the self-reported behavior of male students. Vignettes displaying “William” as a target varied between two types of disease (lung cancer and HIV) and two levels of agency: active (smoker, infected due to drug use, infected due to gay unsafe sex) versus passive (non-smoker, infected by blood transfusion, due to mother-to-infant contamination). Participants were asked several questions to measure their attributions (judgments of controllability, responsibility, and blame), their behavioral intentions (personal willingness, support for institutional help, social distance), their emotions (anger, sympathy), and their social attitudes (authoritarianism, hostility towards homosexuals, belief in a just world, and their concern for equality and social justice). The authors found support for the controllability-responsibility-blame judgment sequence. Ratings were higher for the active vignettes; however, there was no difference depending on the disease. Using a regression path model, Mantler et al. (2003) revealed that pre-existing social attitudes may have a determining impact on blame, and blame influences behavioral intentions. Here, Mantler et al. (2013) are referring to Alicke’s culpable control model of blame (Alicke, 2000). In this model, pre-existing attitudes are associated with judgments of blame, independently from the cognitive and rational sequences advanced in the decision-stage models.
Attributional Framework and HIV
In addition to research that measured attributional tendencies in serious diseases in general (Crandall & Moriarty, 1995; Mantler et al., 2003), some studies focused on the attributional framework of HIV/AIDS. Dooley (1995) tested attributions regarding an AIDS diagnosis with a sample of 255 sociology students. The experiment involved a man that had just been diagnosed with AIDS. There were five possible scenarios for the HIV infection: homosexual partner, heterosexual partner, blood transfusion, injected drug use, and unspecified cause. Results showed that sexual transmission (both heterosexual and homosexual), transmission via drug use, and unspecified transmission produced higher attributions of control and higher feelings of anger. The blood transfusion scenario resulted in fewer attributions of control and increased sympathy. Information about the transmission seems to be a significant factor in the attributional process. Drug users may be more stigmatized in comparison to individuals in need of blood transfusions (Anderson, 1992; Weiner et al., 1988).
In another study, it was found that gender is also an important factor in attributional processes. Cobb and De Chabert’s (2002) experiment involved a person who sought counselling for their recent HIV diagnosis. Gender was the only variable that changed. The attributions of responsibility were significant for both women and men. However, participants displayed a higher willingness to help women (Cobb & De Chabert, 2002).
Further, Seacat et al. (2007) tested the attributional framework of control-responsibility-blame with HIV scenarios that also accounted for differences between heterosexual and homosexual men. The results of this experiment indicate significant attributions of control, responsibility, and blame for all scenarios of infection. Control and responsibility attributions were higher if the person was homosexual (Seacat et al., 2007).
Therefore, there is sufficient scientific evidence to support the investigation of these attribution tendencies. Negative attributions may make people feel uncomfortable accessing health services (Costa et al., 2018), which can worsen the HIV epidemic. Blame, for instance, is an obstacle to HIV serological status disclosure, which is often important for HIV-infected people as it increases their quality of life (Paxton, 2000). Blame can be associated with the misconception of preventive programs (Maes, 1994). Self-blame and blame attributions in general may hinder self-care and helping behaviors (Cobb & De Chabert, 2002). Control-blame-responsibility attributions most likely still influence how these patients are perceived by healthcare staff. However, at the time former studies about attributional frames regarding HIV were conducted, there were no effective medications to treat the disease. Nowadays, there are different treatment possibilities, and the infection is no longer necessarily fatal. Thus, considering the detrimental implications that attributions may have on the health of individuals and the new context of the HIV/AIDS epidemic, it is important to conduct scientific investigations about the controllability-responsibility-blame attributional sequence. This is the aim of the present study.
In previous researches, the attributional theory was tested through data analysis techniques that require a priori input of the model structure. Linear regression was the most used technique; it requires a priori specification of independent and dependent variables. Even though linear regression provides an effective method for testing hypotheses, it hinders the possibility of finding alternative attributional paths that have not yet been established. In the present study, we attempted to use a novel data analysis technique that does not require a priori input of the model structure to analyze the relationship between attributions of causality (blame, responsibility, and control), willingness to help, and emotional reactions (anger and sympathy). We aimed to assess whether the structure developed without a priori inputs on independent and dependent variables from a Bayesian network associates controllability, responsibility, blame, and positive and negative emotions with behavioral intentions.
Method
The original study (Azevedo, 2000) used the experimental vignette from the study by Seacat et al. (2007), which was translated into Brazilian Portuguese and German (from the Brazilian Portuguese version). The vignette depicted a situation of HIV infection. The person in the scene was either a heterosexual man, a homosexual man, or a trans woman, and the infection necessarily occurred in a situation of unprotected sex or blood transfusion. The six possible scenarios were: (1) heterosexual man, unprotected sex; (2) heterosexual man, blood transfusion; (3) homosexual man, unprotected sex; (4) homosexual man, blood transfusion; (5) trans woman, unprotected sex; and (6) trans woman, blood transfusion. The scenarios with the heterosexual man can be considered a control group, while the rest are the experimental groups. For this study, variations were not considered in terms of sexual orientation and gender identity, nor the forms of exposure. A validation question asked for basic information about the vignette to exclude participants who did not understand or read the text provided.
Participants
The participants were undergraduate students from the medicine, nursing, dentistry, psychology, and physical education courses, and health professionals from the city of Porto Alegre, Brazil, and students from the nursing, psychology, social pedagogy courses and medical professionals from the city of Essen, Germany. In regard to the Brazilian participants, the course coordinators from Universidade Federal do Rio Grande do Sul (UFRGS) sent e-mails to the students to invite them to participate in the research. The same process was carried out by the district offices of the Municipal Health Department of Porto Alegre regarding the health service staff. The sample of German participants was obtained through convenience sampling. Participants accessed the research website through advertisements posted on social networks or leaflets distributed at the Universität Duisburg-Essen.
Nine individuals did not consent to the study. Thus, they did not take part in data collection. One hundred and two individuals left incomplete protocols, and forty-nine were excluded because they did not respond correctly to the manipulation-check questions. Therefore, the data analysis included three hundred and fifty-eight individuals from 18 to 75 years old (M = 26.12; SD = 8.91). 82.4% of them were female, 71.23% (n = 255) from Brazil, and 28.77% (n = 103) from Germany.
Instruments
The original study (Azevedo, 2000) used the experimental vignette from Seacat et al.’s (2007) investigation. The vignette was translated into Brazilian Portuguese and German (from the Brazilian Portuguese version). The vignette depicted a situation of an HIV infection. The person in the scene was either a heterosexual man, a gay man, or a trans woman, and the culprit of the infection was either unprotected sex or a blood transfusion. The six possible scenarios were as follows: (1) heterosexual man, unprotected sex; (2) heterosexual man, blood transfusion; (3) gay man, unprotected sex; (4) gay man, blood transfusion; (5) trans woman, unprotected sex; and (6) trans woman, blood transfusion. The scenarios that included the heterosexual male can be considered a control group, while the others are the experimental groups. For this study, neither variations in terms of sexual orientation and gender identity nor the routes of exposure were considered. A validation question requested basic information about the vignette with the aim of excluding participants who had not understood or read the provided text.
Sociodemographics
Participants answered sociodemographic questions about gender, age, sexual orientation, profession, and religion.
Attribution of control, blame, and responsibility
The scale that measured participants’ attribution to the vignette had a total of 13 items (e. g., “The person in the scene is responsible for his disease”; Mantler et al., 2003), answered in a five-point Likert scale. The answers could range from 1 (totally agree) to 5 (totally disagree). The items assess the extent to which the participant attributes the possibility of control, responsibility, and blame for the disease to the person in the scene. Seacat et al. (2007) found acceptable internal consistency indices for the subscales responsibility (α = .91), control (α = .88), and blame (α = .84). For this study, Cronbach’s alpha values were .88, .90, and .79, respectively. The three-factor model showed good adjustments in the CFA with the DWLS estimator: CFI = .99; TLI = .99; RMSEA = .04 (90% C.I. (.03, .06)).
Emotional reactions
The eight-item scale of emotional reactions was also developed by Mantler et al. (2003). Of the eight items in the scale, four pertain to the extent to which each participant feels angry at the person in the scene (e. g., “I feel angry at the person in the scene”); the remaining four items measure sympathy (e. g., “I feel compassion for the person in the scene”). Answers range from 1 (totally agree) to 5 (totally disagree). In its original development sample, this scale had an acceptable internal consistency of α = 0.71 (Seacat et al., 2007). The current study had an internal consistency of .60 for positive emotions and .50 for negative emotions. The scale had an overall internal consistency of α = .56, 95% C.I. = (.50, .62). By conducting the CFA using the DWLS estimator, we found good adjustment for this sample in a two-factor solution: CFI = .99; TLI = .98; (RMSEA = .04 (90% I.C. (.01; .07)).
Willingness to help
Willingness to help the user was evaluated by using a 10-item scale developed by Dooley (1995). The 10 items on the scale (e. g., “I would help the person in the scene to walk,” “I would go to the pharmacy to fill a prescription for the person in the scene”) specifically assess the willingness to help people living with HIV or AIDS in a five-point Likert scale. Answers range from 1 (totally agree) to 5 (totally disagree). The scale had an internal consistency of α = .88 (Seacat et al., 2007). For the present study, Cronbach’s α was .92. The CFA conducted by using the DWLS estimator for a single-factor solution showed good fit indices: CFI = .99; TLI = .99; RMSEA = .03 (90% C.I (.00, .05)).
Procedures
The Portuguese-German adaptation of the instruments was conducted by an expert native Brazilian translator who is fluent in German. Subsequently, a German social psychologist and a Brazilian social psychologist fluent in German evaluated the translation considering its comprehension, format, and instructions. Relevant aspects pertaining to the cross-cultural validation of psychological instruments, such as conceptual and idiomatic equivalence, were taken into consideration. As content validity evidence, the translators agreed that all aspects assessed were clear.
Data collection was conducted between April 2017 and October 2018 by using online forms. Before completing the questionnaire, participants signed an Informed Consent Form. Anonymity was guaranteed, and only the researchers had access to data. The instruments were presented in the following order: 1) emotional reactions; 2) attribution of control, blame, and responsibility; and 3) willingness to help. The average time for completion was @ 17 minutes.
Data Analysis
The three scales were calculated using mean scores. We used a two-step approach: firstly, the equivalence class was estimated using the EBICglasso; subsequently, the alternative models were fitted. The present technique consists of a Bayesian network visualized as a Directed Acyclic Graph, which is a method that suggests one structure of path connections based on the robust associations between all variables inserted in a model (Nagarajan et al., 2013).
Zero-order Pearson Correlations and gLasso Network
Zero-order Pearson correlations were calculated between all variables to assess the magnitude of their associations. Afterward, a partial correlation network was conducted with the R software version 1.1.442, using the package “qgraph” (Epskamp et al., 2012). In a partial correlation network, each node represents one of the variables inputted, and each edge represents partial associations between variables. The model is known as Pairwise Markov Random Fields, estimated through L1-regularized neighborhood regression. The regularization is obtained through the Least Absolute Shrinkage and Selection Operator (LASSO; Friedman et al., 2008) that controls model sparsity. This network allows visualization of the partial correlations between variables. Positive correlations are represented by blue edges, while negative correlations are represented by red edges. The strength of the associations is represented by the thickness of the edges - thus, the thickest the edge, the stronger the association. The inputted variables were the mean scores of the instruments, which assess the constructs “Willingness to help,” “Emotional reactions” (Sympathy and Anger), and “Attribution of control, blame, and responsibility.” The Expected Influence of the inputted variables was also provided - i.e., the cumulative expected role of each node in the activation, persistence, and remission of the network (Robinaugh et al., 2016). We decided to assess Expected Influence as the measure of centrality because it considers negative associations among nodes to indicate the importance of each node in a network (Robinaugh et al., 2016). Other centrality measures, such as Strength, do not take the negative associations into account, providing a limited metric instead.
The gLasso network provides undirected graphs - i.e., only the magnitude of the partial correlation between variables is represented. The directionality of the associations is not estimated, and, therefore, a Bayesian Network analysis was conducted.
Directed Acyclic Graph
To compute a Bayesian network, displayed as a Directed Acyclic Graph (DAG), we inputted the same variables as in the gLasso network and ran the Tabu algorithm in the R software version 1.1.442 using the package “bnlearn” (Scutari, 2010). The direction of the associations between variables is estimated in causal probability estimates (Nagarajan et al., 2013) by using the Tabu algorithm to estimate the direction of the causal relations. A k-fold cross-validation procedure using the Tabu learning algorithm and the Robust Maximum Likelihood extraction method was conducted, and the expected loss value was considered. It is worth highlighting that k-fold is a common cross-validation method to estimate how the model is expected to perform in other datasets by shuffling the dataset randomly, splitting it into k groups, and assessing the adequacy of the model in these groups. The loss function used in the “bnlearn” package is the log-likelihood loss - i.e., the expected negative log-likelihood. Thus, the lower the expected loss value, the better.
The DAG only provides unstandardized regression weights. Therefore, a path analysis reproducing the model generated by the DAG was conducted to assess the standardized Beta coefficients of the connections discerned by the algorithm. This analysis was carried out by using the Robust Maximum Likelihood extraction method in the “lavaan” package (Rosseel, 2012).
Results
Table 1 shows the zero-order Pearson correlations between attributions of causality (control, blame, and responsibility), willingness to help, and emotional reactions (anger, sympathy). Attributed responsibility had statistically significant correlations with willingness to help (r = -.23, p < .001), sympathy toward the infected person (r = -.84, p < .001), and attribution of blame (r = .11, p = .035). Attribution of control had significant correlations with anger towards the infected person (r = .91, p < .001), sympathy towards the infected person (r = -.18, p < .001), and attribution of blame (r = .40, p < .001). Attribution of blame had significant correlations with anger towards the infected person (r = .35, p < .001) and sympathy towards the infected person (r = -.27, p < .001). Finally, sympathy towards the infected person significantly correlated with willingness to help (r = .30, p < .001) and anger towards the infected person (r = -.15, p = .004).
Table 1 Zero-order Pearson correlations between attributions of causality, willingness to help, and emotional reactions (n = 356)
| - | 1 | 2 | 3 | 4 | 5 | 6 | |
| 1. Willingness to help | - | - | - | - | - | - | |
| 2. Anger | -.09 | - | - | - | - | - | |
| 3. Sympathy | .30*** | -.15** | - | - | - | - | |
| 4. Blame | -.07 | .35*** | -.27*** | - | - | - | |
| 5. Control | -.10 | .91*** | -.18*** | .40*** | - | - | |
| 6. Responsibility | -.23*** | .03 | -.84*** | .11* | .05 | - |
Note. *p < .05, **p < .01 ***, p <.001
The thickest edge in the gLasso network is the one connecting attribution of control and anger towards the infected person - same as in zero-order Pearson correlations, i.e., the connection with the strongest magnitude. The second thickest edge connects attribution of responsibility and sympathy towards the infected person. Thus, the strongest associations found in zero-order Pearson correlations were also found in partial correlations, as depicted in the gLasso network in Figure 1. Furthermore, the expected influence of each node was also assessed and displayed in Figure 2, indicating that the attribution of control and responsibility have the highest cumulative influence in the network.

Note. “Help” corresponds to “Willingness to help”, “Responsibility” to “attribution of responsibility”, “Blame” to “Attribution of blame”, and “Control” to “Attribution of control.”
Figure 1 DgLasso Network

Note. “Help” corresponds to “Willingness to help”, “Responsibility” to “attribution of responsibility”, “Blame” to “Attribution of blame”, and “Control” to “Attribution of control.”
Figure 2 Expected Influence of each variable in the network
Table 2 provides the partial correlation values between all variables in the network. The partial correlations support the strong association between attribution of control and anger against the infected person (r = .89), as well as between attribution of responsibility and sympathy towards the infected person (r = -.84). It is important to stress that, due to the regularization method used, partial correlations whose values are not higher than the threshold estimated through EBIC computation are set to 0 (for a thorough description, see Epskamp & Fried, 2018).
Table 2. Partial correlation values represented in the gLasso network. Willingness to help, and emotional reaction
| - | 1 | 2 | 3 | 4 | 5 | 6 |
| 1. Willingness to help | - | - | - | - | - | - |
| 2. Anger | 0 | - | - | - | - | - |
| 3. Sympathy | .17 | 0 | - | - | - | - |
| 4. Blame | 0 | 0 | -.26 | - | - | - |
| 5. Control | 0 | .89 | -.06 | .16 | - | - |
| 6. Responsibility | 0 | 0 | -.84 | .16 | .04 | - |
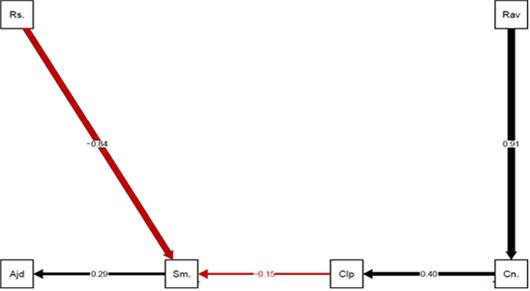
Figure 3 depicts the DAG that emerged from the algorithm. The average Markov blanket size and the average neighborhood size were 2.00, and the penalization coefficient, obtained through 133 tests in the learning procedure, was 2.94. A K-fold cross-validation for Bayesian networks procedure using 10 folds was conducted, and the expected loss value was 5.48. It is worth noting that the 10-fold cross-validation was selected since the parameter for k is between 5 and 10 (Jung, 2017).

Note. “Help” corresponds to “Willingness to help”, “Responsibility” to “attribution of responsibility”, “Blame” to “Attribution of blame”, and “Control” to “Attribution of control.”
Figure 3 Directed Acyclic Graph
Some points are notable in the DAG. Firstly, anger towards the infected person and attribution of responsibility were exogenous variables, which means that they were not predicted by any other variable but predicted third variables: anger predicted attribution of control, whereas attribution of responsibility predicted sympathy towards the infected person. Further, the willingness to help was an endogenous variable - i.e., it did not predict any variable but was predicted by sympathy towards the infected person. Attribution of control, attribution of blame, and sympathy towards the infected person were predicted by third variables but also predicted other variables. For instance, attribution of control predicted attribution of blame and sympathy towards the patient, whereas attribution of blame predicted sympathy towards the patient. Moreover, sympathy was the only predictor of willingness to help.
In regard to the standardized Beta coefficients obtained through the path analysis reproducing the model that emerged from the DAG, all paths were statistically significant (p < .01) (Figure 4). The path with the highest magnitude was anger predicting attribution of control (β = .91, p <. 001), followed by the attribution of responsibility predicting sympathy towards the infected person (β = -.84, p < .001), attribution of control predicting attribution of blame (β = .40, p < .001), sympathy towards the infected person predicting willingness to help (β = .29, p < .001), and attribution of blame predicting sympathy towards the infected person (β = -.15, p < .001).
Discussion
The findings of this study are consistent with previous researches that applied the attributional model in the context of HIV infection (McDonell, 1993; Dooley, 1995; Cobb & De Chabert, 2002; Mantler et al., 2003; Seacat et al., 2007). The results indicate that attributions of blame, control, and responsibility play significant but different roles in emotional reactions and in the willingness to help. It is thus worth stressing that our procedures support the robustness of our inferences by not only providing results that are consistent with previous studies on causal attribution but also by using methods that were used and pointed out as adequate in past research (e. g., McNally et al., 2017).
One of the main merits of our study in comparison to previous literature was the demonstration of the applicability of the model within a methodology in which the relationship between the variables was not assumed a priori. This finding provides further validity evidence to the theory of the association between the attribution processes (separating the cognitive components), the positive and negative emotions, and, in turn, its influence on the willingness to help. Moreover, the present research approached some unexplored issues - namely, that positive emotions directly affected the intention to help, which is influenced by the attribution processes that are, in turn, influenced by the negative emotion (anger). Therefore, a negative emotion towards a person with HIV increases the tendency to attribute less control regarding the infection, which will induce greater blame, and, therefore, leads to less sympathy and a decrease in the willingness to help. Conversely, the tendency to attribute responsibility to individuals for their HIV infection can also reduce feelings of sympathy in a different path. Hence, our study demonstrates the influence of emotions in attributions and behavior, displaying two distinct paths.
Therefore, the present study does not confirm the linear association between variables based on the control-responsibility-blame model. The cognitive processes, emotional reactions, and behaviors do not follow this linear attributional framework as well (Heider, 1958; Shaver, 1985; Weiner, 1995) - at least not in this combined sample. In contrast to Mantler et al’s (2003) findings, blame was not the final attribution in our survey. It is worth emphasizing that Mantler et al. (2003) tested the directionality of the cognitive process with a behavioral outcome, not considering the role of emotions - an aspect that may have contributed to the divergence of our results.
In Mantler et al. (2003), blame was the judgment most strongly associated with behavioral responses. Mantler and collaborators assumed that, in real-life contexts, people might not necessarily go through the stages of the decision-stage models but may instead focus on the blameworthiness of the perceived person, going backward through the stages to seek confirmatory evidence for their hypotheses and prejudices (Alicke, 2000). Also, our study raises the question of whether, under such circumstances, control on the side of the perceiver is still important and triggers the belief in a just world, victim blaming, and other processes associated with blame. According to Lerner’s hypothesis, people want to preserve their belief in a just world by demeaning or blaming victims, which presupposes that people get what they deserve (Lerner & Miller, 1978). Likewise, the Defensive Attribution Hypothesis may still explain behavior in this context - namely, that people want to keep their belief in having personal control over their own lives by considering the victims self-responsible.
By blaming victims for something that has happened to them and attributing it to faults and carelessness, people presuppose that this would not happen to them (Walster, 1966; Shaver, 1970). Moreover, a belief in immanent justice will prompt a need to blame the victim (Berrenberg et al., 1990). Conversely, our results point out that negative emotions could be an index of prejudices that were present before the cognitive-attributional process occurred. A recent systematic review involving healthcare professionals’ beliefs and attitudes towards patients who suffer from substance abuse disorders found that, in most of the analyzed studies, healthcare staff tends to have negative emotions in regard to such patients (Van Boekel et al., 2013). Thus, in our results, prejudice against an HIV-positive person could prompt anger. This is consistent with Corrigan et al (2003) study, which indicates that anger and fear were highly correlated in the context of the attributional process. Nevertheless, in both arguments, the attribution of responsibility is emotionally biased.
In Weiner’s attribution model, responsibility for a behavior plays an essential part in the interaction with sympathy, determining behavioral responses to an event. Weiner (1995) makes a clear distinction between the attribution of control and responsibility. Control is related to a person’s degree of control over a behavior; responsibility is an evaluation that involves morality. In our study, attribution of responsibility decreased sympathy that, in turn, reduced behavior intention - congruent with Dagnan and Cairns (2005), who found an association between positive emotions and the attribution of responsibility and showed that sympathy was the only independent predictor of helping behavior. In accordance with our findings, Armstrong and Dagnan (2011) found that, in the context of intellectual disability, responsibility affected willingness to help independently of anger. In addition, positive emotions are favorable in explaining helping behaviors in a specific manner. In a study conducted by Sharrock et al. (1990), optimism significantly influence the willingness to help the paramedical and nursing staff in a mental health facility that cared for people in conflict with the law. Further, there is evidence that sympathy is a significant factor in increasing the willingness to help, and it is associated with lower attributions of responsibility (Dagnan & Cairns, 2005). Considering the role that responsibility plays, it is inevitable to discuss our results within the framework of stigma as well.
HIV-related stigma is one of the major factors associated with HIV infection (Logie et al., 2016). There is sustained evidence that the experience of stigma can reduce HIV testing rates (Turan et al., 2011), increase avoidance of healthcare services (Pachankis et al., 2015), and increase the frequency of unprotected sex (Ayala et al., 2013). Therefore, if HIV-infected people are held personally accountable, they will not get social support, which is important when coping with a serious illness (Berrenberg et al., 1990).
There are, however, strategies that can be adopted in order to reduce HIV-related stigma. Stahlman et al. (2017) and Mahajan et al. (2008) recommend that data regarding stigma should be included in the HIV/AIDS routine surveillance in conjunction with condom distribution, HIV testing, and antiretroviral therapy. According to Mahajan et al. (2008), measuring stigma with adequate, valid, and reliable instruments can help assess prevention and treatment programs and help determine the efficacy of stigma reduction interventions. In summary, to succeed in dealing with the HIV/AIDS epidemic, it is necessary to implement measures that assess stigma in the routine protocol for HIV/AIDS (Stahlman et al., 2017) and to create high-quality stigma reduction interventions with multidimensional stigma indicators (Mak et al., 2017).
Taking into consideration the main aim of this study, we conclude that the attributional process is a key aspect in the perception of HIV-positive people and that the status of the disease as curable might not have changed how HIV-infected people are perceived. Moreover, the control-responsibility-blame sequence could display different configurations in the presence of positive and negative emotions. Responsibility affects sympathy independently from anger, and anger influences control and blame. Blame attribution still plays a role in our study, affected by attribution of control - influenced by anger, but sympathy seems central to understanding willingness to help, affected by the attribution of responsibility.
In addition, we can still expect self-stigmatization from HIV-infected people. Evidence from attributional theories contributes to our understanding of how people who suffered negative life events are perceived, but it may also provide insight into their own perception of themselves, as well as other people’s perceptions of them.
Further, there is a perpetuation of subtle prejudice: even though there is a range of awareness campaigns about HIV, as well as available treatments for the disease, an HIV-positive individual is still held responsible for their infection. The findings of our study suggest that spreading information is still important, including among healthcare professionals who deal with HIV/AIDS patients.
In conclusion, it is worth pointing out some of the limitations of the present study. Our sample was mostly composed of females (82.4%), so the model developed may have a gender bias, and it was not sufficiently substantial to assess cross-cultural differences in the attributional processes - thus, it is possible that some differences were neglected. Furthermore, even though the data analysis used in this study provided novel insights into attributional processes due to its lack of a priori inputs, it is not a hypothesis-driven technique, which may hinder the replicability of the model across different contexts (although there is evidence for the replicability of networks, as shown by Borsboom et al., 2018). Furthermore, it is worth stressing that the estimated DAG may not be unique in its equivalence class. Indeed, using the criterion of d-separation, it is possible to see in Figure 3 that the relation between Anger and Control could be reversed, and the resulting causal model would be equally valid; future studies should thus assess this possibility. Another important limitation of the analysis is that the algorithm used to estimate the DAG assumes the absence of confounders as well as of faithfulness. It is recommended that future studies use sensitivity analysis as another indicator of how robust the estimation of the causal structure is. A fifth limitation concerns the lack of statistical power calculation due to the fact the techniques available in network analyses are still inconclusive and “a topic for future research” (Epskamp et al., 2018, p. 210). Despite its limitations, to the best of our knowledge, this is the first study to test attributional process models in the context of HIV infection using data analysis techniques that do not require a priori inputs to the model.

