











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
Root canal preparation aims cleaning and shaping the root canal by means of instrumentation and irrigating solutions (1). Disinfection and complete cleaning of the root canal system is a complex procedure (2), and an improper cleaning may result in treatment failure (3). The evolution of endodontic instruments using nickel-titanium alloys (NiTi) and heat treatment allowed greater resistance to cyclic fatigue and greater flexibility (4) providing centralized preparation in curved root canals (5,6).
ProDesign Logic (PDL) (Easy Equipamentos Odontológicos, Belo Horizonte, MG, Brazil) is a rotary NiTi instrument system (7) composed by glide path files (taper .01) and shaping files (taper.05 or .06) (Pinto et al., 2019). The heat treatment Control Memory (CM) of these files provides flexibility and improves their flexural resistance (4), promoting centralization for curved root canal preparation (5,6). Hyflex EDM (HEDM) (Coltène/ Whaledent, Allstätten, Switzerland) instruments have also CM heat treatment, however, these files are produced via electro-discharge machining (EDM) (8). This manufacturing process improves the mechanical properties of HEDM (9). These files maintain its integrity after multiple uses, and they are associated with high resistance to cyclic fatigue (10).
Micro-computed tomography (micro-CT) has been used to evaluate root canal preparation using different NiTi instruments (5,11,12). However, these analyzes can be influenced by many factors, such as different scan settings, images resolutions and misinterpretation of ring artifacts (13). For analysis of root canal preparation, different micro-CT acquisition parameters are used, with scanning voxel size of 9 µm (6,14,15), 14 to 15µm (5,16,17), 16 to 18µm (11,12,18), until 30µm (19). The different approaches for image acquisition, image evaluation, and reporting of outcomes make difficult the interpretation of reported results and comparation of different studies (13).
Up to now there are no studies that assessed the influence of micro-CT voxel size on root canal preparation evaluation, as well as no study assessed this influence at 5µm. Therefore, the aim of this study was to assess the influence of micro- CT voxel size on analysis of increase in volume, debris, and uninstrumented root canal surface, after instrumentation with PDL or HEDM. The null hypotheses were that there would be no differences between the voxel sizes, and between the different systems to root canal preparation.
Materials and methods
Sample size calculation
For sample calculation, G Power 3.1.7 for Windows program (Heinrich-Heine-Universität Dusseldorf, Dusseldorf, Germany) was used. T test for 2 independent groups was used with an alphatype error of .05 and a beta power of .95 for all the variables. Previous studies that used micro-CT imaging for evaluating root canal preparation with similar morphology were used to determine the specific effect size for volume of root canal, 2.723 (15); debris, 3.432 (14); and untouched surface, 1.451 (20). Twelve specimens per group were indicated as being the ideal size required.
Specimen selection
All procedures were approved by the Faculty's Ethics Committee(CEPno.10411219.9.0000.5416). The roots were inspected under a stereomicros- cope at ×12 magnification to exclude those with any external dentinal defect and the roots with immature apices.
Human mandibular first and second molars previously stored in 0.1% thymol solution at 5°C were used. The inclusion criteria included two independent mesial root canals according type IV Vertucci's classification (21), angle of curvature between 25° and 35° in accordance with the Schneider method (22) and radius of curvature smaller than 10mm, following the Pruett's method (23), besides complete apical formation, absence of root fractures, calcifications or internal resorptions. For this purpose, a digital radiographic system (RVG 6100; Kodak Dental Systems, NY) was used to select teeth according to inclusion criteria. Image J program (National Institutes of Health, Bethesda, MD, USA) was used to assess the degree of curvature in radiographic images. All selected teeth were scanned using a micro-CT device (SkyScan 1276; Bruker-micro-CT, Kontich, Belgium) at a low-resolution (35µm voxel size) under the following settings: copper and alumi- num filters, 87-millisecond exposure time, frame averaging of 3, 180° rotation around the vertical axis, rotational step of 0.5° at 80 kV and 300µA.
The mesial root canals of the specimens were divided into two experimental groups randomly (n=12), considering the preoperative volume of the root canals. The root length was standardized at 18mm, with a tolerance of ±1mm of discrepancy. The specimens were embedded in condensation silicone (Oranwash, Zhermack SpA, Badia Polesine, Italy) to simulate the periodontal ligament.
Root canal preparation
Conventional access cavities were perfor- med, and the root canals were explored by using a size #10 K-file (Dentsply Sirona Endodontics, Ballaigues, Switzerland). The working length was established 1mm shorter from the apical foramen of each specimen. In the sequence, a trained operator instrumented all the specimens with the aid of an operating microscope (MC-M1232, DF Vasconcellos, Valença, RJ, Brazil) at 13X magni- fication, using an endodontic motor (VDW Silver, VDW GmbH, Munich, Germany).
PDL Group: Instrumentation with PDL. The 30/.01 file was used in continuous rotation at 350rpm speed and 1 Ncm torque, using in-and- out movements up to the working length. Then, the 30/.05 file was used at 600rpm speed and 4 Ncm torque.
HEDM Group: Instrumentation with HEDM. The 10/.05 file was used in continuous rotation at 300rpm speed and 1.8 Ncm torque, using in-and- out movements up to the working length. Then, the HEDM 25/.08 file was used at 500rpm speed and
2.5 Ncm torque.
The root canal irrigation was performed with 5mL of 2.5% sodium hypochlorite (NaOCl), using a 30G side-vented needle (NaviTip, Ultradent Products, South Jordan, UT) adapted to a 5mL syringe (Ultradent Products), which was placed 2mm short of the working length. As final irrigation, 2mL of 17% EDTA followed by 5mL of distilled water were used.
MICRO-CT Analysis
The specimens were rescanned at a high- resolution (5µm voxel size) before and after instrumentation in a micro-CT device (SkyScan 1272; Bruker-microCT, Kontich, Belgium) under the following settings: copper filter, 180° rotation around the vertical axis and rotational step of 0.2° at 100kV and 100µA. The images were reconstructed using NRecon software (V1.6.10.4; Bruker, Belgium), and superimposed with geometric alignment using the DataViewer software (V.1.5.1, Bruker, Belgium). The qualitative analysis was performed using the CTAn software (V.1.14.4, Bruker, Belgium). Images at 5,10 and 20μm were used for quantitative analysis (Figure 1). For this purpose, the previously scanned 5μm images were resized by 2 and 4, respectively using the CTAn software (24,25,26).
Analyzes were performed in the middle and apical thirds of the roots, being considered 3mm for each third. Preoperative volume, volume of prepared canal, surface area after preparation and volume of debris after preparation were obtained.
Based on these values, the percentage of volumetric increase (% Volumetric increase), percentage of debris (% Debris) and percentage of uninstrumented surface (% Uninstrumented surface) were calculated using the following formulas:
% Volumetric increase = 100 - Volume of prepared canal x 100 / Preoperative volume
% Debris = Volume of debris x 100 / Volume of prepared canal
% Uninstrumented surface = Uninstrumented surface area x 100 / Surface area after preparation
Statistical analysis
The data obtained for each of the parameters evaluated were submitted to the Shapiro- Wilks normality test, and all data presented normal distribution. For analysis between groups and between the middle and apical thirds was use no-paired t-test. For analysis among images with different voxel size was used ANOVA test. The level of significance was 5% for all the analysis.
Results
No differences were observed for percentage of volume increase, debris and uninstrumented surface between the root canals prepared by PDL and HEDM in the middle and apical thirds at all voxel sizes (5,10 and 20μm) (p>0.05) (Figure 2). Both systems promoted higher percentage of debris in apical third compared with middle third (p<0.05). The comparison of uninstrumented surface of root canal showed similar results between thirds for both groups at 10 and 20μm (p>0.05). However, after instrumen- tation with PDL the percentage of uninstrumented surface was higher in the apical third than middle third at 5μm (p<0.05). When comparing images with different voxel sizes (5,10 or 20µm), both groups showed different means for the variables without significant difference (p>0.05) (Table 1).
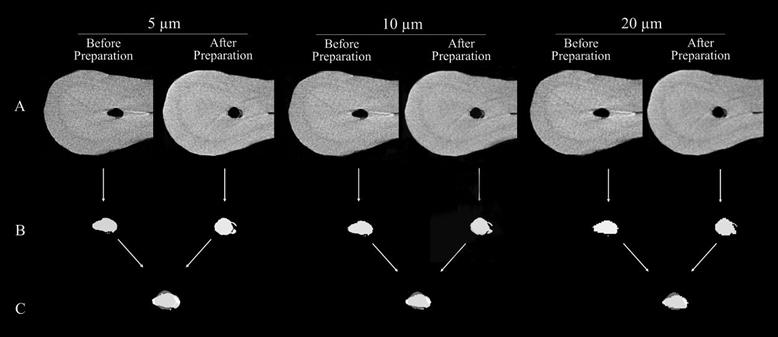
Figure 1 Representative micro-CT images at different voxel sizes showing original transversal slices of the roots canals (A), segmented root canals (B) and the superposition of the segmented root canal before and after instrumentation for volumetric analyses (C).
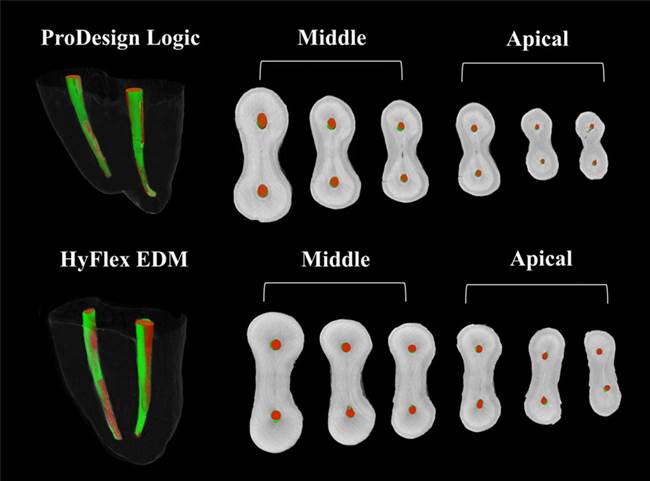
Figure 2 3D reconstructions and cross-sectional views of images with 5µm of voxel size of middle and apical thirds of mesial roots od mandibular molars prepared by ProDesign Logic or HyFlex EDM. Root canal before preparation (red), root canal after preparation (green).
Table 1 Means and standard deviations of volume, volume increase (%), debris (%) and uninstrumen- ted surface (%) of root canals in different voxel sizes after preparation.
| - | - | ProDesign Logic | - | - | HyFlex EDM | - | - |
|---|---|---|---|---|---|---|---|
| - | - | 5µm | 10µm | 20µm | 5µm | 10µm | 20µm |
| Pre-operative canal (mm³) | Middle | 0.4 ± 0.1ª | 0.4 ± 0.1ª | 0.4 ± 0.1ª | 0.4 ± 0.1ª | 0.3 ± 0.2ª | 0.4 ± 0.2ª |
| - | Apical | 0.20 ± 0.07ᵇ | 0.20 ± 0.07ᵇ | 0.19 ± 0.06ᵇ | 0.2 ± 0.1ᵇ | 0.2 ± 0.1ᵇ | 0.2 ± 0.1ᵇ |
| Prepared canal (mm³) | Middle | 0.5 ± 0.1ª | 0.5 ± 0.1ª | 0.6 ± 0.1ª | 0.7 ± 0.2ª | 0.7 ± 0.2ª | 0.7 ± 0.2ª |
| - | Apical | 0.30 ± 0.07ᵇ | 0.27 ± 0.05ᵇ | 0.27 ± 0.05ᵇ | 0.31 ± 0.04ᵇ | 0.3 ± 0.2ᵇ | 0.3 ± 0.1ᵇ |
| Volume Increase (%) | Middle | 60 ± 30ª | 60 ± 30ª | 60 ± 30ª | 90 ± 50ª | 80 ± 50ª | 90 ± 30ª |
| - | Apical | 60 ± 50ª | 50 ± 30ª | 60 ± 50ª | 70 ± 60ª | 70 ± 40ª | 70 ± 50ª |
| Debris (%) | Middle | 3 ± 2ᵇ | 3 ± 2ᵇ | 2 ± 2ᵇ | 4 ± 2ᵇ | 3 ± 2ᵇ | 3 ± 2ᵇ |
| - | Apical | 5 ± 3ª | 5 ± 2ª | 4 ± 3ª | 6 ± 3ª | 6 ± 3ª | 5 ± 3ª |
| Uninstrumented surface (%) | Middle | 30 ± 20ᵇ | 29 ± 20ª | 28 ± 20ª | 40 ± 10ª | 30 ± 20ª | 30 ± 10ª |
| - | Apical | 54 ± 20ª | 50 ± 20ª | 40 ± 20ª | 50 ± 20ª | 40 ± 20ª | 30 ± 20ª |
There was no statistically significant difference among the columns. Different superscript lowercase letters in the same column indicate statistical difference between the thirds of the same preparation (P<.05).
Discussion
Micro-CT is one of the most used analysis tool for root canal preparation assessments (5,6,27). Therefore, it is important to know the influence of scanning parameters on the outcomes of each variable associated to the instrumentation capacity. Previous study has reported no influence of voxel size on debris evaluation when analyses was performed between 5 and 20µm voxel size (25). However, other investigation, assessing the influence of voxel size on microcracks analyses showed higher accuracy for images with lower voxel size (26). Therefore, in agreement with the current literature, our results report that the influence of voxel size on analyses of root canal preparations using micro-CT is variable-dependent. Although, in the present study, the voxel size did not influence the analyses of root canal volume and debris, the root canals prepared by PDL showed higher uninstrumented surface in apical third than middle third only when the evaluation was performed at 5µm.
A high percentage of uninstrumented surface after root canal preparation have been reported by several investigations. However, their micro-CT images were obtained using different parameters of scanning, varying since 9 to 30µm of voxel size (6,11,12,16,18,19). These studies have showed conflicting results, even using similar apical preparation size (6,11,12,16,18) or similar root canal anatomy (6,11,12). In this study a different outcome was observed when the uninstrumented surface analyzes were performed at 5µm, therefore, the micro-CT voxel size must be taken into account for comparisons between studies. A voxel is the discrete unit of the scan volume that is the result of the tomographic reconstruction representing three dimensions (13). The voxel size seems to be one of the main factors that can affect the quality of the images and consequently the analyzes performed (13,24). The analysis of trabecular bone structure was significantly affected by micro- CT scanning voxel size (28,29). A previous study (30), evaluating the presence of voids in filled root canal at different voxel size, detected more voids at smaller voxel sizes (5.2, 8.1 and 11.2µm) than at 16.73.
The CM heat treatment applicated for PDL and HEDM instruments allows safe preparations in curved canals (5). Moreover, the EDM surface treatment present in HEDM files improve its mechanical properties (10). The greater taper of the first 4mm for 25/.08 HEDM file, with its progressive taper reduction until to .04 has motivated the use of PDL file with larger tip diameter, size 30/.05 in this study. The constant taper of PDL promotes similar size along the active part between the instruments evaluated. Thus, in the present study, PDL and HEDM presented similar percentage of volumetric increase and uninstrumented surface.
The presence of debris in the root canal makes it difficult to disinfect (31), and decreases sealer adhesion to dentinal tubules (27). There were no differences for percentage of debris accumulated between the root canals prepared for PDL or HEDM. However, for both instruments evaluated, there was more percentage of debris in apical third than middle third, with means of 5,07% for PDL and 5,77 for HEDM, in analysis at 5µm. Previous studies have also observed large amounts of accumulated debris in mesial roots of mandibular molars (6,14,27). These studies suggest greater apical enlargement (6) or additional cleaning protocols such as passive ultrasonic irrigation (14,25) or XP-endo Finisher (14) as methods to decrease accumulated root canal debris after root canal preparation using mechanized NiTi files.
Since the influence of voxel size on root canal preparation analyses seems to be depen- ded of the variable evaluated, it is important the planning of study design considering the choice of adequate micro-CT scanning protocol. In addition, taking account that besides voxel size, the final resolution of the images also depends on other parameters such as average absorption of the sample, detector noise, reconstruction algorithm, X-ray focal spot size and shape, detector aperture, and scanner geometry (13), a pilot study is stron- gly recommended before the scans, instead of using parameters from previous study.
Conclusion
Within the limitations of this ex vivo study, it can be concluded that voxel sizes do not have a significant impact on analysis of volume of root canals and accumulated debris. However, the voxel size should be considered as a potential factor for uninstrumented surface, since it was observed different results for images at 5µm, in compara- tion with images of 10 and 20µm of voxel sizes. Further research is necessary using lower micro- CT voxel size scans.
Author contribution statement
Conceptualization and design: J.C.P and M.T-F.
Literature review: J.C.P
Methodology and validation: J.C.P, E.L-O., T.J.B., J.M.G-T and M.T-F.
Formal analysis: J.C.P and M.T-F.
Investigation and data collection: J.C.P and M.T-F.
Resources: J.C.P and M.T-F.
Data analysis and interpretation: J.C.P, E.L-O., T.J.B., J.M.G-T and M.T-F.
Writing-original draft preparation: J.C.P and M.T-F.
Writing-review & editing: J.C.P, E.L-O., T.J.B., J.M.G-T and M.T-F.
Supervision: M.T-F.
Project administration and funding acquisition: M.T-F.

