










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkActa Médica Costarricense
versão On-line ISSN 0001-6002versão impressa ISSN 0001-6012
Acta méd. costarric vol.54 no.4 San José Out./Dez. 2012
Original
Epidemiological
behavior of cases of suspected leptospirosis
in five health regions
of Costa Rica
Jorge Sequeira-Soto1 y Juan José
Romero-Zúñiga2
Authors’
Memberships:
Abbreviations: CNRL,
Correspondence:
Abstract
Background
and aim: The prevention and control of leptospirosis
depends on the knowledge about the exposure of people to possible risk
factors,
which are reported in the national surveillance system for this event.
This
study describes the epidemiologic behavior of the cases of suspected leptospirosis, which were researched using the
protocol in
force in the country.
Methods:
Across-sectional study that describes the epidemiologic behavior of the
cases
of suspected leptospirosis using the data
of the case
investigation forms of the surveillance system for this event.
Laboratory data
was obtained from the INCIENSA´s National Leptospirosis Reference Center. The period of
study was
between 2004 and
Results:
498 case investigation forms were analyzed. The most frequent
occupations are
those described as “without risk” (37.3%), students (23.2%) and
agricultural (22.1%). The exposure to domestic animals prevails
(67.6%), of
this 92% were dogs. The presence of rodents is reported in 52.6% of the
cases.
A 29.5% had contact with ponds or swimming pools and 28% with stagnant
waters,
both with a prevalence of 1, 88 and 1, 71(p<0,05).
Conclusion:
The frequency of cases in groups “without occupational risk”
indicates that the case investigation form must be redesigned to
incorporate
other variables that include recreational ones.
Keywords:
Leptospirosis, epidemiological
surveillance, risk
factors
The
clinical presentation of the disease in the human
being starts with a feverish first stage, 2 to 20 days after infection.
Once
the immune system phase starts, a second stage occurs which coincides
with the
elimination of the leptospira organisms in
urine, in
the case of humans, the elimination is reduced because of the acid pH.4
The
most common clinical presentation is an anicteric
leptospirosis, as a subclinic
form or of moderate severity in where the presence of a sudden onset
fever is
notable. 4,5 The icteric
form is more uncommon (5-10% of all cases), but it is usually of much
greater severity
and mortality, associated with pulmonary hemorrhage involvement in some
cases,
presenting a high mortality.5.9 The clinical presentation
of the
disease, being so broad, results in its confusion with other similar
diseases,
complicating its diagnosis when this other diseases are endemic in
regions
where leptospirosis is common. This occurs
in
diseases like dengue, yellow fever, malaria, rickettsiosis,
influenza and, when there are hemorrhagic manifestations, it can be
confused
with other hemorrhagic viral diseases such as hantavirus.5,10
For a long
time, leptospirosis
has been considered a worldwide zoonotic
disease,
given its epidemiological characteristics. This spirochaete
has been found in every mammal including aquatic mammals.2
However,
from a anthropocentric point of view, the
most important natural hosts are of domestic or wild character, that
are
related to household environment or peridomiciliary,
such as dogs, cattle and rodents.5,11-14 When leptospira
organisms colonize the proximal renal tubules, their elimination is
possible
during the lepstopiuric phase, altogether
with their
great ability of survival in wet environments,15 makes
infection
possible when entering through the mucosa and skin wounds.4,16 The
human being gets infected directly through the urine of an infected
host or
indirectly through infected solutions, including puddles, rivers and
lakes,
that keeps the organism viable, penetrating through a lacerated skin,
allowing
the entrance of the organism into the blood circulation.
Epidemiologically an
occupational transmission has been reported; identified in the
beginnings of
the disease, especially in workers like veterinarians, ranchers, rice,
corn and
sugarcane farmers; and more recently a household and recreational
transmission
has become important.4,17,18 There is evidence that the
behavior of
the disease vary between ecological niches;19 thus it is
necessary
to characterized this behavior with the purpose of identifying the
possible
risks factors to intervened to control and prevent new cases.
The
disease is distributed along all
In this
study, the epidemiological behavior of the
suspected cases of leptospirosis in the
five more
prevalent health regions in
Materials
and Methodology
Units of
Analysis: The information in the leptospirosis
cases research files (FIC) was used as an unit of analysis, that were
detected
by the Leptospirosis National Surveillance
System in
the regions of North Huetar, Central
Pacific, East
Central, Atlantic Huetar and Brunca
between 2004 and 2008.
Case:
For the purpose of this study, suspected cases were those found in the
FIC.
Data and
Analysis Detection: The information of the
FIC was obtained from the Ministry of Health’s Heath Areas, between
2004
and 2008. The complementary information of the results of the sent
samples for
the diagnosis of leptospirosis was
compiled in a
database of the CNRL of INCIENSA in the same period of time. The
database was
made with the Epiinfo 3.5.1 program. The
prevalence
ratio and intervals of confidence were calculated at 95%, of the
occupational,
exposure and protective measures variables. The information analysis
was made
through Epiinfo 3.5.1, Epidat
3.1 and Win Episcope 2.0 programs. 21.22
Type of
Study and Variables:
Descriptive (Statistical) Study,
through analysis of demographics, environmental, occupational and
laboratory
variables, contained in the FIC.24 Age variable was stratified in age
groups
with 20 years intervals. Occupational variable was stratified depending
on the
reported risks of acquiring the disease: students, housewives,
agricultural and
livestock activities, “other no-risk occupations” (office workers,
operators, drivers, security guards, etc) and “other risk
occupations” (slaughter line operators, tourist guides and
topographers,
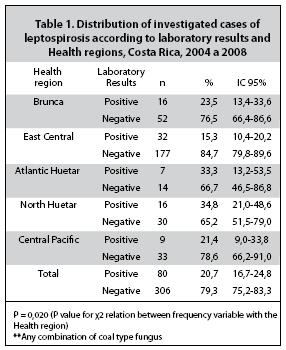
etc). Table 1
Laboratory
Diagnosis: Positive
samples are those with a title of ≥1:320
in MAT analysis. Using Dri-Dot® (Biomerieux) technique, positive samples were
classified,
detecting total anti-Leptospira antibodies;
or were
positive samples in the culture. In the other hand, negative samples
were those
that resulted as negative by some or all diagnostic techniques mention
above.
Results
The
information was compiled from a total of 498
cases, distributed as follows: 80 from Brunca
region
(16.1%), 258 from East Central region (51.8%), 39 from Atlantic Huetar region (7.8%), 59 from North Huetar
region (11.8%) and 62 from Central Pacific region (12.4%). According to
data
from health regions and the Ministry of Health, in the period of study,
1339
suspected cases were notified, and should be investigated and each FIC
should
go to its respective Ministry of Health area in its Health region. When
asked,
representatives of Health Surveillance Teams of the Ministry of Health,
in
relation to what was the cause of the lack of information available,
the
response was that the information
was lost
because of flooding in the facilities, and lost of data caused by
computer
damaging without backups, and also problems to send the information
compiled by
the staff of the CCSS (Caja Costarricense
de Seguro Social –
24.9% of
the compiled FIC, correspond to the latest
approved and current edition by the Ministry of Health (2002).16 The
rest 75.1%
were researched through another type or version of the ballots, from
the
1998’s epidemiological surveillance protocol (10.6%) and the 2000’s
leptospirosis prevention and management
protocol
(58.2% and respective ballots from other events (i.e. Hantavirus) or
another
type of documentation like letters or non standardized administrative
reports
(6.2%).
Of 498
FIC, 386 (77.5%) had a first initial laboratory
sample, in which 68 were positive (17.6%) and 318 were negative
(82.4%). A
total of 107 had a second sample (21.5%) in which 29 were positive
(27.1%) and
78 were negative (72.9%). As shown in table 1, when analyzing the
suspected
cases in a global manner, with both samples and without taking into
account if
the time defined by protocol was fulfilled between both of them,24 a positivity of 20.7%
was
reported. In the analysis of sample-taking time, only 9.5% of all cases
fulfilled the first sample-taking time (7-10 days of the onset of
symptoms) and
of the second sample (10-20 days of the first sample), without a
significant
difference between analyzed regions (p= 0.75). % of investigated cases
Epidemiological
Behavior in Cases Investigated
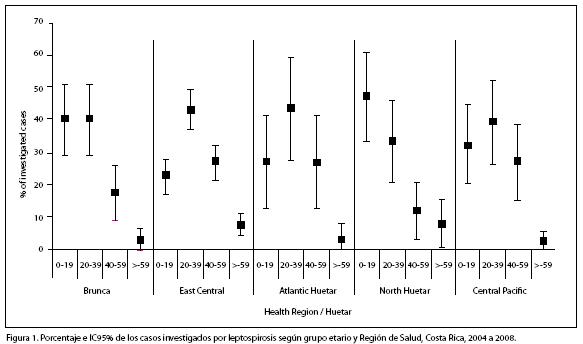
A total of
498 FIC were compiled between 2004 and
2008, with age information in 469 cases. 29.4% of this cases belong to
the age
group between 0 and 19 years old, 41.2% belong to the ages between 20
and 39
years old, 23.7% between 40 and 59 years old and 5.8% were 60 years old
or
more. Nonetheless, a significant difference (p<0.05) was found on
the
distribution according to health regions, thus for example, in the Brunca and North Huetar,
the age
group of 0-19 years old contributed to a important percentage of cases (figure
1). In general, 83% of cases were man, without significant
difference between
regions (p=0.33).
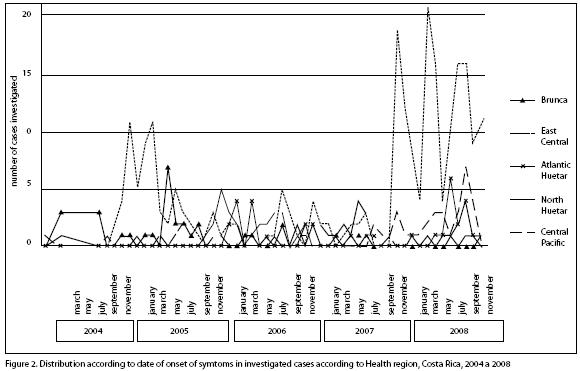
Through
time, date distribution of the onset of
symptoms of suspected cases of leptospirosis,
were
similar in five regions, with the exception of East Central region,
where the
reported cases increased irregularly between 2005 and 2008
(figure
2).
Evaluation
of Exposure and Protective Factors
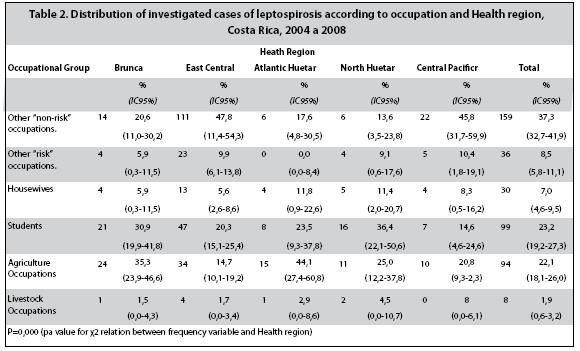
When
analyzing the behavior of exposure variables that
were traditionally reported in the literature as risk factors for
acquiring the
disease, activities classified as low risk for acquiring the disease
represent
the highest percentage of the investigated group (table 2). However,
when
analyzing the prevalence ratio, this group presents the lowest
probability of
positivity on the laboratory (RP<1, IC95%: 0.49-1.24) altogether
with
housewives group (RP<1, IC95%: 0.141.66). The student group was
placed
second, followed by people related to agricultural activities. It’s
noticeable, that less than 2% of the cases, performed livestock
activities that
were related traditionally to higher risk of acquiring the disease.
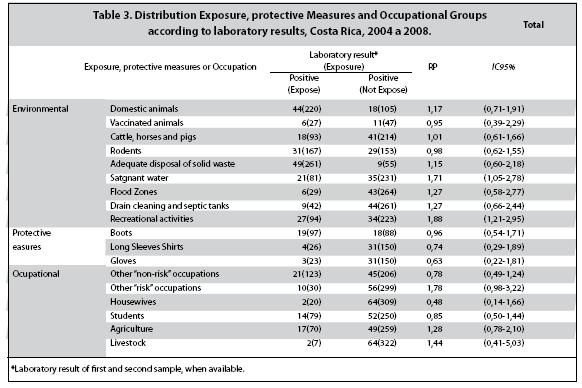
When
prevalence ratio of positive cases by laboratory were analyzed, in
different
occupational groups, agricultural and livestock activities and also
other
“risk” occupations, showed a slightly higher prevalence in
comparison with other activities. However, none can be
interpreted
as a possible significant association, because IC intervals include the
unit
(table 3).
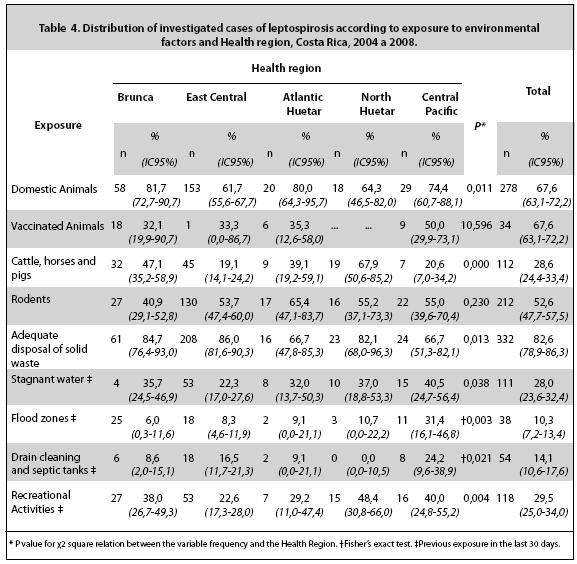
As seen in
table 4, more than
67% reported an exposure
to domestic animals, of these less than 40% have nonspecific
vaccination or
vaccine specificity (valid FIC lack of reports of this information).
The
exposure to domestic animals represents more than 80% of the Brunca region. The main domestic animal reported
were dogs,
representing 95% of the cases of domestic animals.
Almost 83%
of cases presented an adequate management
of solid waste, with significant difference between regions
(p<0.05);
however, more than half of this reports reported the presence of
rodents,
without a significant difference between regions (p>0.05).
A little
less than 30% of cases, reported contact with
stagnant water, recreational activities in wells and pools in the last
30 days,
a significant difference between regions was found (p<0.05), with
the
exception of North Huetar, where almost
50% reported
contact with wells and pools, 30 days prior to the onset of symptoms. These two
variables
showed
a significant association when analyzing the prevalence ratio (table 3). On the
other hand, Central Pacific region, points a higher percentage of
cases,
related to flood
regions (31.4%), higher than the country’s average
(10.3%).
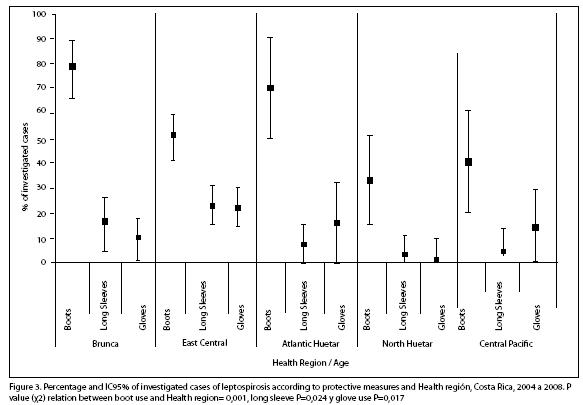
The FIC
compiled information about the use of three
protective measures against leptospirosis:
use of
boots, long sleeve shirts and gloves during workday. More than half of
the
cases investigated (58.8%) used boots during workday, however; the use
of
gloves and long sleeves shirt were found only in 15.7% and 16.2%
respectively;
variables with significant difference in regional distribution
(p<0.05)
(figure 3). In
those occupations related to agricultural or livestock
activities, when analyzing the protective measures, 88.3% of cases used
boots,
29.3% used long sleeves shirts and 20.5% used gloves.
Discussion
Epidemiological
Behavior of Cases Investigated
The study
findings about the epidemiological behavior
of cases, according to age and genre, are congruent to previous reports
of the
Ministry of Health between 2002 and
The lack
of the existence of standardization and systematicity
in the process of investigation in suspected
cases is noticeable, mostly because the majority of FICs
are outdated. An important part of the problem resides in the
differences
between FICs versions of some variables.
For example,
the 2000’s version asks about the exposure 15 days prior to the onset
of
symptoms; meanwhile, the 2002’s version asks about the exposure 30 days
prior. This inconvenient is worsen when using files from other events
or not
standardized documentation that does not compiled epidemiological
variables of
importance.
From the
total of investigated cases, the laboratory
was capable of identifying as less than 21% positive samples, through
serology.
This low percentage can be explained mainly because of the low capacity
of the
system to recover second samples (27.7%), and because of the limited
percentage
of samples taken in the time indicated by protocol. The non-compliance
of these
criteria causes an important subdiagnosis
by the
laboratory and therefore, the inability of the system to identify
adequately
the confirmed cases of leptospirosis.
Analyzing
the pattern of occurrence of the disease in occupationalgroups,itisnoticeablethatthemostrepresentative
group are those individuals that performed activities that
epidemiologically
(in other literature) has not been related with an increased risk for
acquiring
the disease occupationally, such as drivers, office workers and
merchants, etc.
The student group and individuals working in agricultural activities
group came
second. However, despite the higher frequency of this groups, the
activities
“without risk”, the students and housewives presents a prevalence
ratio that could suggest a lowest risk in presenting a positive sample,
since
the IC 95% limits, are close to the statistical significance. So, there
is a
necessity of developing a different epidemiological approach from the
traditional one, framed by a paradigm as seen the leptospirosis
as a mainly occupational disease.
It draws
attention, the low percentage of suspected
cases investigated that performed livestock activities, while a
prevalence
ratio is slightly higher, such activities are strongly related to the
disease,
with the increased risk of acquiring the disease as described by many
authors.4, 26, 27 This conditions is particularly important in areas,
like
North Huetar region, where the livestock
activity is
very important, and where a high percentage of cases, associated with
cattle,
horses and pigs are reported.
With the
compiled information by the case investigation
ballot, we can conclude that the most frequent exposure factor in
suspected
cases is the exposure to domestic animals, primarily dogs. The
investigated
cases, indicate that involved domestic animals where 35% vaccinated;
however,
the instrument at present is incapable to identify the type of
vaccination or
at least if they received a vaccine against leptospirosis
and when did they received it, making this information useless when
trying to
direct the efforts to control and prevent the disease.
It is
necessary, that efforts must delve in the
identification of the behavior of this disease in peridomiciliary
animal groups, and especially if associated with positive cases. This
way, the
intervention of organisms and institutions, such as the Ministry of
Agriculture
and Livestock (Ministerio de Agricultura
y Ganadería – MAG) are essential, into
identifying suspected cases or confirmed cases of leptospirosis,
with the purpose of initial identification of sources of infection in
animal
groups of zoonotic importance, like
canines, cattle,
pigs, horses and old world rats and mice (Murinae).
Precisely, the exposure to rodents, are the same in all regions
equally. In a
lower percentage the contact with stagnant water and recreational
exposure to
wells and pools, showed a higher probability of obtaining a positive
sample in
the laboratory in a significant manner.
The
observations made, suggests that epidemiological
behavior differ in some regions, for example, North Huetar
region, presents a high incidence of cases, related to animals and
recreational
activities, Central Pacific region reports a higher number of cases
related to
floods, however, further studies should be made, that involves the
analysis of
the zoonotic epidemiological behavior and
analytic
studies of risk factors.
Utility of
the Case Investigation Ballot
The
investigation of suspected cases represents an
important step in the epidemiological surveillance process. The system
compiled
the information needed to identify possible points of control and
prevention of
the disease. In accordance to the compiled information in this study, a
higher
frequency to identify the possible risk factors incorporated in FIC
(identified
now on the literature). It is necessary to identify other predisposing
factors
of the dissemination of rodents that were reported in half of the
cases, even
if 80% of these cases have an adequate solid waste management,
resulting in a
reduction of predisposing factors for the presence of rodents.
In the
other hand, representation of the students and
low risk of acquiring the disease occupations groups, suggest the
possibility
of a recreational relation for the transmission to humans, like rivers,
lakes
or any humid zone that allow the organism to survive. However, the only
question asked in the FIC refers to a 30 days contact to pools or wells
prior
to the onset of symptoms, not taking into account other sources of
infection
such as fishing activities, canopy, climbing, or other sports as soccer
without
the use of footwear,3, 28-32
such
data can be used with the purpose of identifying possible asymptomatic
or mild
symptomatic cases.
Beyond the
variables mention above, other possible
risk factors to be intervened by healthcare services were unable to
identify.
The actual FIC present a clear slant, in search of identifying mainly
occupational exposures, for example, the protective measure variables.
The
improvement of this instrument through the incorporation of other
epidemiological variables is necessary. The current case investigation
ballot
does not contemplate the presence of wounds in skin, or its number and
location, this data has been demonstrated useful in identifying the
risk of
infection and install direct protective measures.33
The
ballot, also collects information about the
contact with floods and stagnant water zones, but does not identify the
sources
of these or the geographical region in which they are located, data
that can be
useful to install protective measures and alert the community.
It is also
advisable that the file include variables
related to water sources, open water drains, allowing dissemination of
rodents;
observation of the home environment, peridomiciliar
and occupational has evidence suggesting the presence of rodents
(nests, gnawed
food, feces presence, etc). Also, it is advisable the zoning of
suspected
cases, since there are important differences in risk factors between
rural and
urban zones.3, 4
It is
important to emphasize to the healthcare
personnel, that recollection of data of suspected cases is needed, not
only
through interview, but also the observation of the household, peridomiciliar and occupational environments
should be
performed.
We
concluded that the instrument used in the
recollection of data in suspected cases should be restructure, making
it more
flexible to new patterns of occurrence of the disease in the Costa
Rican
population; incorporating findings of new research studies about risk
factors
in the country. The data obtained showed that while many cases are
occurring in
young people with activities related to the agricultural sector, a
significant
majority are activities and risk factors related to students or
individuals
with an occupation that are not traditionally related to a high
exposure for leptospirosis. Unfortunately,
the current instrument is
incapable to identify these risk factors, as it focuses primarily in
identifying leptospirosis as an
occupational disease,
so a new perspective should be reconsidered by all healthcare
authorities.
Competing
Interest: The authors have no conflict of interest to declare.
Acknowledgements:
The results presented in this study would not have been possible
without the
support and cooperation of the staff of Health Areas of Brunca,
East Central, Atlantic Huetar, North Huetar and Central Pacific, and the Ministry of
Health’s Directorate of Health Surveillance,
References
1. Adler B, Peña A de la. Leptospira and leptospirosis. Vet Microbiol 2010; 140:287-96. [ Links ]
2. Levett PN, Smy the L. Minutes International Committee on Systematics of Prokaryotes, Subcommittee on the taxonomy of Leptospiraceae,
3. Faine S, Adlen B, Bolin B, Perolat P. Leptospira and Leptospirosis. Seg. ed. Editorial Medi Sci, 1999. [ Links ]
4. Levett PN. Leptospirosis. Clin Microbiol Rev 2001; 14:296-326. [ Links ]
5. Bharti AR, Nally JE, Ricaldi JN, Matthias MA, Diaz MM, Lovett MA, et al. Leptospirosis: a zoonotic disease of global importance. The Lancet 2003; 3:757-771. [ Links ]
6. Doudier B, Garcia S, Quennee V, Jarno P, Brouqui P. Prognostic factors associated with severe leptospirosis. Clin Microbiol Infect 2006; 12:299-300. [ Links ]
7. Dupont H, Dupont-Perdrizet D, Perie JL, Zehner-Hansen S, Jarrige B, Daijardin JB. Leptospirosis: prognostic factors associated with mortality. Clin Infect Dis 1997; 25:720-4. [ Links ]
8. Segura ER, Ganoza CA, Campos K, Ricaldi JN, Torres S, Silva H, et al. Clinical Spectrum of Pulmonary Involvement in Leptospirosis in a Region of Endemicity, with Quantification of Leptospiral Burden. Clin Infect Dis 2005; 40:343-51. [ Links ]
9. Trevejo RT, Ashford DA, Rigau-Pérez JG, McClure EM, Jarquín-González C, Amador JJ, et al. Epidemic leptospirosis associated with pulmonary hemorrhage-Nicaragua, 1995. J Infect Dis 1998; 178:1457-63. [ Links ]
10. La Rocque R, Breiman R, Ari M, Morey R, Ara F, Hayes J, et al. Leptospirosis during Dengue Outbreak, Bangladesh. Emerg Infect Dis 2005; 11:11-14. [ Links ]
11. André-Fontaine G. Canine leptospirosis-do we have a problem? Vet Microbiol 2006; 117:19-24. [ Links ]
12. Ward MP. Seasonality of canine leptospirosis in the
13. Sepúlveda A, Dimas J, Preciado F. La rata y el perro, importantes vectores de la leptospirosis en explotaciones pecuarias de Cd. Guzmán, Jalisco. Rev Cubana Med Trop 2002; 54:21-23. [ Links ]
14. Botazzo Á, Freitas JC de, Bracarense AP, Eckehardt E, Oliveira R de. Leptospirosis in slaughtered sows: serological and histopathological investigation. Braz J Microbiol 2002; 33:174-177. [ Links ]
15. Trueba G, Zapata S,
16. Vinetz JM. Leptospirosis. Curr Opin Infect Dis 2001; 14:527-538. [ Links ]
17. Keenan J, Ervin G, Aung M, McGwin G, Jolly P. Risk factors for clinical leptospirosis from
18. Belmaker I, Alkan M, Barnea A, Dukhan L, Yitzhaki S, Gross E. Risk of Transmission of Leptospirosis from Infected Cattle to Diary Workers in Southern Israel. Isr J Med Assoc J 2004; 6:24-27. [ Links ]
19. Sarkar U, Nascimento SF, Barbosa R, Martins R, Nuevo H, Kalafanos I, et al. Population-based case-control investigation of risk factors for leptospirosis during an urban epidemic. Am J Trop Med Hyg 2002; 66:605-610. [ Links ]
20.
21. Dean AG, Arner TG, Sunki GG, Friedman R, Lantinga M, Sangam S, et al. Epi Info™, a database and statistics program for public health professionals. Centers for Disease Control and Prevention,
22. Hervada X, Santiago M, Vázquez E, Castillo C, Loyola E, Silva L. Epid at 3.1, Programa para análisis epidemiológico de datos tabulados. Xunta de Galicia, Organización Panamericana de Salud, Coruña, España, 2005. [ Links ]
23. De Blas I, Ortega C, Frankena K, Noordhuizen JP, Thrusfield M. Win Episcope 2.0, improved epidemiological software for veterinary medicine. Zaragoza, España, 2001. [ Links ]
24. Costa Rica, Ministerio de Salud. Protocolo para
25. Costa Rica, Ministerio de Salud. Memoria Institucional 2002-2006. San José: Ministerio de Salud; 2006. [ Links ]
26. Valverde M, Ramírez J, Montes de Oca L, Goris M, Ahmed N, Hartskeerl R. Arenal, a new Leptospira serovar of serogroup Javanica, isolated from a patient in Costa Rica. Infect Genet Evol 2008; 8:529-33. [ Links ]
27. Giraldo G, Orrego A, Santacruz M, Yepes E. Leptospirosis. Las aguas de la explotación porcina como vehículo de
28. Sánchez RM, Sierra AP, Suárez MB, Álvarez ÁM, Hernández JM, González MD, et al. Evaluación de la efectividad de una nueva vacuna contra la leptospirosis humana en grupos en riesgo. Rev Panam Salud Pública 2000; 8:385-92. [ Links ]
29. Solano A, Boza R, Sáenz E. Leptospirosis en Humanos. Rev Costarric Cienc Med 1996; 17:41-60. [ Links ]
30. Michel V, Branger C, Andre-Fontaine G. Epidemiology of leptospirosis. Rev Cubana Med Trop 2002; 54:7-10. [ Links ]
31. Centers of Diseases Control and Prevention. Outbreak of leptospirosis among white-water rafters—
32. Vinetz JM, Glass GE, Flexner CE, Mueller P,
33. Phraisuwan P, Whitney E a S, Tharmaphornpilas P, Guharat S, Thongkamsamut S, Aresagig S, et al. Leptospirosis: skin wounds and control strategies, Thailand, 1999. Emerg Infect Dis 2002; 8:1455-9. [ Links ]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}