Introducción: La disfunción endotelial es un marcador temprano de la enfermedad arterioesclerótica, y su detección nos permite determinar cuáles pacientes son potenciales sujetos de tratamiento para revertir la progresión del padecimiento vascular. Dado que el paciente diabético es un paciente con alta prevalencia de complicaciones arterioscleróticas, la detección de éste fenómeno en el mismo, es de capital importancia.
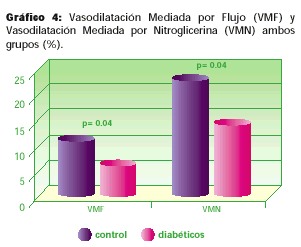
Métodos y Resultados: Mediante Doppler braquial en estado basal, isquemia y post-itroglicerina, se determinó la capacidad vascular de aumentar el flujo sanguíneo en 10 pacientes sanos y 20 pacientes diabéticos, con el objetivo de correlacionarlos con su HbA1c y perfil lipídico. La vasodilatación mediada por endotelio (VMF) y la vasodilatación mediada por nitroglicerina (VMN) expresadas en porcentaje de cambio del diámetro vascular, se encontraron reducidas en forma estadísticamente significativa en el grupo de diabéticos, (5.57% vs. 9.97% para el grupo control p= 0.04, y 21.49% vs. 12.64% para el grupo control p = 0.04 respectivamente) éstas alteraciones correlacionaron con los años de evolución de la enfermedad y los niveles de colesterol total, LDL y triglicéridos en éstos pacientes. ]]>
Conclusión: El estudio doppler braquial es un instrumento útil para determinar mediante la disfunción endotelial, las fases tempranas de la arterioesclerosis en pacientes de alto riesgo para ésta, y los factores potencialmente reversibles que alteran este fenómeno podrían ser intervenidos en aras de mejorar el pronóstico de estos pacientes.Palabras Claves: Disfunción Endotelial, Diabetes Mellitus.
Summary
Introduction: Endothelial dysfunction is a common accepted surrogate marker of atherosclerotic disease. Its early detection allows us to determine which patients need attention in order to stop the progression of the vascular disease. Since diabetic patients have a high prevalence of cardiovascular complications, the early detection of this phenomenon is of capital importance for their prognosis.
Methods: Using brachial Doppler during rest, ischemia and post- nitroglycerin ischemia, the vascular reactivity of the vessel was obtained in 10 healthy patients and 20 type 2 diabetic patients. This data was correlated with their glycosilated hemoglobin levels and lipid profiles. Their endothelium derived vasodilatation and their nitroglycerin derived vasodilatation were expressed as the percentage of change in the luminal diameter of the vessel and both of them were reduced in the diabetic patients with a statistical significance (5.57% vs. 9.97% for the control patients p =0.04, y 21.49% vs. 12.64%, p= 0.04 for the diabetic patients). These alterations correlated with the years of evolution of the disease and the total colesterol levels as well as the LDL and tryglicerides levels.
Conclusion: The Brachial Doppler study is a useful tool to detect endothelial dysfunction as an early stage of atherosclerosis in high risk patients and allows the treatment of the factors that might influence this phenomenon in order to improve their prognosis.
Introducción
La Diabetes Mellitus(DM), está asociada a una mayor prevalencia de enfermedad arterial coronaria. La prevalencia de la enfermedad coronaria es del 35% en pacientes con DM comparada con 2.4% en la población general. (1) A la vez, la morbilidad asociada a los accidentes cardiovasculares, también es de mayor consideración en el paciente diabético. (2) La disfunción endotelial, (3) las anormalidades de la coagulación (4) y el trastorno metabólico, (5, 6) juegan un papel importante en el desarrollo temprano y la aceleración del proceso arterosclerótico de estos pacientes. La disfunción endotelial probablemente sea uno de los eventos iniciales en el desarrollo de la arteriosclerosis, y su rol es determinante en las manifestaciones isquémicas de la enfermedad coronaria. (7) La liberación vascular local de mediadores vasoactivos tales como óxido nítrico, endotelina, angiotensina II y factor hiperpolarizante se encuentra severamente distorsionada en presencia de ése fenómeno. (8)
Celermajer y cols. Han descrito la determinación de la dilatación mediada por flujo (DMF) en la arteria braquial o femoral, (9) como método indirecto del grado de disfunción endotelial de los pacientes así como la utilización de la vasodilatación mediada por nitroglicerina (VMN) como método para demostrar la capacidad vasodilatadora intrínseca del músculo liso vascular ante el estímulo exógeno. La naturaleza no invasiva de éste test y la capacidad de poder realizarle múltiples tests al mismo paciente, han favorecido que este método sea hoy en día el más utilizado para determinar la disfunción endotelial. (10)
El presente estudio describe la presencia y grado de disfunción endotelial en pacientes diabéticos tipo 2 sin enfermedad coronaria manifiesta, en una población hispánica. ]]>
Materiales y MétodosDiseño del estudio:
Pacientes: Para el presente estudio, se organizaron dos grupos de pacientes. El primer grupo consiste de 10 pacientes adultos, no diabéticos, voluntarios.
El segundo grupo consiste de 20 pacientes diabéticos tipo 2 controlados en forma ambulatoria en el Departamento de Medicina Interna del Hospital México, quienes asistían en el momento de su selección, a la consulta externa. A ambos grupos de pacientes se les explicó el procedimiento y se les solicitó su participación en el estudio. Todos dieron su aprobación y consentimiento antes de incluirlos en el protocolo. Al momento de realizarles los estudios, todos los pacientes tenian 12 o más horas de ayuno.
Protocolo: A todos los pacientes se les tomaron sus antecedentes, los cuáles incluían: edad, antecedentes heredofamiliares, antecedentes personales de inicio de su enfermedad diabética, años de duración de la misma, complicaciones micro y macrovasculares, tabaquismo, tratamiento para su DM, peso, talla, tensión arterial y pulsaciones. Posteriormente se les tomaron las muestras para análisis de laboratorio clínico y se les realizó el procedimiento ultrasonográfico.
Análisis de muestras sanguíneas: A los dos grupos de pacientes se les realizaron las siguientes pruebas en estado de ayuno, en el laboratorio clínico del Hospital México:
Glucosa: La glucosa plasmática se determinó mediante un autoanalizador, con el método de la glucosa oxidasa (Beckman / Coulter, corporation USA.)
La Hemoglobina glicada (HbA1c) se determinó mediante el método de electroforésis de Hemoglobina (Beckman / Coulter Corporation, USA.)
El colesterol total, HDL, LDL y los triglicéridos se determinaron mediante el metodo de colorimetría utlizando el autoanalizador Synghcon CX9 (Beckman / Coulter Corporation USA.)
Estudio Doppler sonográfico: El estudio Doppler se realizó de acuerdo al protocolo descrito por Celermajer y cols. (9) Todos los pacientes se encontraban con 12 o más horas de ayuno y tenían 30 o más minutos de encontrarse en reposo. A cada paciente se le realizaron tres estudios ultrasonográficos diferentes: ]]>
1. El diámetro y la vasodilatación mediada por flujo (VMF) de la arteria braquial derecha fue medida utilizando un transductor linear ultrasonográfico de 7.5 Mhz (SSHP-140A, Toshiba, Japan). En el primer estudio se les determinó previamente tensión arterial y pulso, posteriormente el diámetro braquial vascular basal se determinó mediante doppler pulsado a un angulo de 60º con respecto al vaso, el cuál fue localizado a no menos de 7 cm. de la fosa antecubital, y abordado de forma longitudinal. El diámetro del vaso se midió desde la linea M (unión íntima/media) anterior a la posterior y durante sístole. Se realizaron tres mediciones y el reporte final es el promedio de las mismas. La velocidad del flujo se determinó de acuerdo al análisis de la onda de flujo. Luego de 5 minutos de reposo, se inició el segundo estudio.2. En éste estudio, el brazo del paciente se somete a isquemia mediante la insuflación del manguito del esfingomanómetro 100 mmHg por encima de la tensión arterial sistólica basal del paciente y se mantiene de éste modo durante cuatro minutos. Luego de ser liberada la presión, se toman de nuevo tres mediciones del diámetro vascular, la velocidad de flujo y los signos vitales. Estas determinaciones se realizan en un periódo no menor a 70 segundos después de liberado el vaso. El reporte final del diámetro corresponde a la media de las 3 mediciones hechas. El porcentaje de vasodilatación mediada por flujo se calcula a partir de la fórmula: (%VMF =(DIAMETRO POSTISQUEMIA DIAMETRO BASAL) / DIAMETRO BASAL x 100). Luego de 5 minutos de reposo se realiza el tercer procedimiento.
3. En esta oportunidad se le administran al paciente 0.5 mg de Nitroglicerina sublingual y luego se somete el brazo de nuevo a isquemia por un período de 4 minutos. Finalmente se toman 3 mediciones del diámetro vascular y se reporta la media de éstas mediciones, se determina velocidad de flujo y signos vitales, el porcentaje de vasodilatación mediada por nitroglicerina (VMN) se estima utilizando la fórmula previamente descrita.
Análisis estadístico: Para el análisis estadístico de los datos se utilizó el paquete estadístico SPSS para Windows 98 versión 8.0, se calcularon las medidas de frecuencia de cada variable y mediante Tstudent de medidas únicas se compararon los grupos control y de diabéticos.
Las correlaciones entre la HbA1c, colesterol, HDL, LDL y triglicéridos con el DMF y la VMN en el grupo control y de diabéticos, se determinaron mediante correlación multivariada de Pearson. La significancia estadística se definió como una p=0.05
Resultados
Todos los pacientes toleraron el estudio en forma adecuada, en ningún paciente hubo cambios importantes en la tensión arterial sistólica o diastólica (> 10 mm Hg). Ninguno de los pacientes tenía antecedentes de enfermedad coronaria al momento del estudio, un paciente del grupo de diabéticos tenía el antecedente de un accidente vascular cerebral previo.
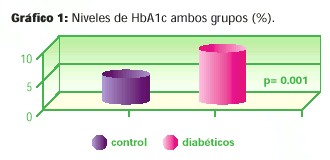
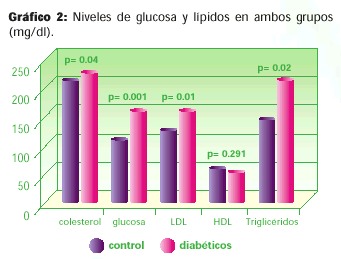
Controles: En los 10 pacientes del grupo control, el diámetro promedio vascular fue de 4.1 mm. El diámetro promedio post-isquemia fue 4.48 mm, La vasodilatación mediada por flujo promedio fue de 9.97%, el diámetro promedio post-nitroglicerina fue de 4.89 mm. y la vasodilatación mediada por nitroglicerina promedio fue de 21.49%. Ninguno de los controles era tabaquista, y los valores promedio de HbA1c, glicemia, colesterol, LDL, HDL y Triglicéridos, estuvieron dentro del rango normal. En el análisis multivariado la VMF correlacionó en forma inversa y significativa, con el nivel de triglicéridos séricos ( r =-0.892 p =0.001) y con el índice de masa corporal (r = -0.688 p = 0.038)
Diabéticos
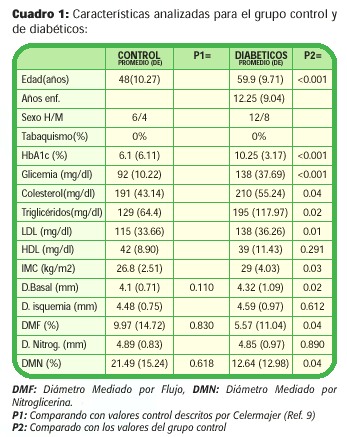
Se estudiaron 20 pacientes diabéticos, 40% mujeres y 60% hombres, 10 pacientes (50%) controlados con insulina, 9(45%) controlados con hipoglicemiantes orales y 1 (5%) con dieta. En éstos pacientes, los niveles de HbA1c, glicemia, colesterol, LDL, Triglicéridos, IMC y el diámetro basal fueron más altos que en el grupo control (estadísticamente significativo) (Cuadro 1 y Gráficos 1-4), el nivel de HDL, fue menor, pero no estadísticamente significativo. El diámetro post-isquemia y post-nitroglicerina fue menor (no estadísticamente significativo) pero los valores de VMF y VMN fueron considerablemente menores (estadísticamente significativo) con respecto al grupo control. En el análisis multivariado, el diámetro postisquemia correlaciona en forma significativa con el diámetro basal (r =0.830 p < 0.0001). ]]>
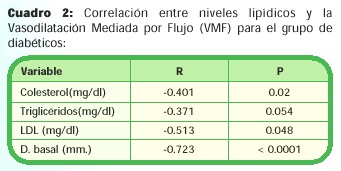
En cuanto a la VMF con respecto a las otras variables, se establecieron correlaciones moderadas (< 0.6) para, el colesterol total, el LDL y los niveles de triglicéridos. (Cuadro 2). ]]>
Discusión
La VMF y la VMN parecieran estar deterioradas en el diabético tipo 2. Nuestros resultados muestran que ambas variables son significativcamente menores en este grupo de pacientes, que en el grupo control. Esta disminución de la VMF pareciera ser una manifestación temprana de la enfermedad arteriosclerótica, detectable antes de la aparición de eventos clínicos cardiovasculares. (11) En modelos animales, se ha demostrado, que la disfunción endotelial aparece tempranamente, antes de que se presenten los cambios estructurales arterioescleróticos (12) vasculares. La disfunción endotelial acelera la interacción entre endotelio, plaquetas neutrófilos y macrófagos que culmina con la formación de la placa. (7, 13)
La VMN también se encuentra deteriorada en éste grupo de pacientes. Previamente se ha demostrado que pacientes con DM tipo 1 también tenían una VMN disminuída con respecto a los no diabéticos, (14) lo que sugiere que los nitratos podrían ejercer un efecto vasodilatador menor en esta población. Sin embargo otro estudio posterior mostró resultados contrarios. (15) La VMN también está afectada en la DM tipo 2 según un pequeño estudio previo, (16) pero éste fenómeno debe ser estudiado en una mayor cantidad de pacientes para ser clarificado adecuadamente.
La disfunción endotelial también se asocia a hiperglicemia aguda en la DM tipo 2 y a la presencia de resistencia insulínica (17, 18) en la aparición temprana de la arteriosclerosis en pacientes con tasa de aclaramiento metabólico de glucosa disminuido.
La glicemia promedio al momento del análisis sonográfico se mantuvo en un rango adecuado, evitando que esta interacción afecte la interpretación de los datos; a los pacientes no se les realizó insulinemia, sin embargo correlacionar la resistencia insulínica con la VMF es un objetivo deseable para un próximo trabajo a realizar. ]]>
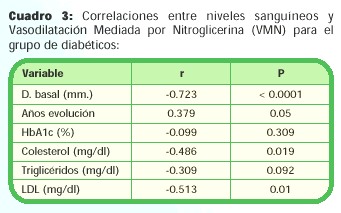
Los niveles de triglicéridos y el IMC correlacionaron inversamente con la VMF en el grupo control, Wilmink y cols, ya han descrito este hallazgo en pacientes hiperlipémicos (19) sin embargo el grupo control fué normotrigliceridémico, lo que sugiere un rol importante de los niveles de triglicéridos en el desarrollo temprano de la enfermedad arterioesclerótica.En el grupo de pacientes diabéticos, existe una correlación inversa moderada pero estadísticamente significativa entre la VMF y la VMN, con los niveles de colesterol, triglicéridos y LDL, pero no así para los niveles de HbA1c. Esta correlación entre los niveles de lípidos y la disfunción endotelial ya ha sido corroborada en otros trabajos de pacientes no diabéticos, (9) y probablemente esté relacionada al efecto inflamatorio de los remanentes lipídicos sobre la pared vascular al unirse a los receptores secuestradores endoteliales, (7) evento que también ocurre en la hipertrigliceridemia. (19)
La VMF depende de los niveles de óxido nítrico, el cuál siendo un radical por sí mismo, reacciona con radicales libres de oxígeno e interfiere con los mecanismos de oxido-reducción, inactiva la transcripción estimulada por el Facto Nuclear NFkb, el cuál estimula la transcripción de genes involucrados en la génesis arteriosclerótica. (20, 21)
La interacción del óxido nítrico con los radicales de oxígeno formados a partir de los remanentes de colesterol en la pared vascular, reduce la disponibilidad del mismo para mediar la relajación vascular. (22) En base a este tipo de observaciones, en numerosos estudios se ha intentado utilizar fármacos hipolipemiantes por períodos relativamente prolongados, para mejorar la cantidad de óxido nítrico disponible localmente y así "revertir" la disfunción endotelial, sin embargo el efecto de estas intervenciones farmacológicas sobre la morbimortalidad cardiovascular del paciente, todavía no han sido claramente dilucidadas, pues los resultados han sido variados y contradictorios. (23)
Los niveles de HbA1c no correlacionaron en forma estadísticamente significativa con el grado de VMF o VMN, tal como ha sido descrito para pacientes con DM tipo 1, (14) sin embargo la escasa cantidad de pacientes diabéticos enrolados, no permite estratificarlos según sus niveles de HbA1c para realizar un análisis de mayor significancia. Los niveles de HbA1c sí se han correlacionado, aunque no en forma estadísticamente significativa con mayor morbi-mortalidad cardiovascular en la DM tipo 2, (24) sin embargo la utilizacion de inhibidores de la enzima convertidora de angiotensina (ECA) (25, 26) y de angiotensina II (AT-II) en pacientes diabéticos, (18) para revertir la disfunción endotelial, dada la capacidad de estos medicamentos de activar la sintetasa de óxido nítrico, se ha estudiado; y a éste efecto farmacológico se le han atribuido disminuciones considerables en la morbi-mortalidad cardiovascular de estos pacientes. (27, 28)
Conclusiones
El uso del Doppler braquial para detectar la disfunción endotelial en el paciente con riesgo de enfermedad cardiovascular es un método relativamente sencillo y reproducible en un laboratorio de alta calidad, que nos permite detectar a los pacientes con enfermedad arteriosclerótica temprana, a la vez convierte éstos pacientes en candidatos a recibir una intervención en sus estilos de vida y farmacológica, que permita revertir ésta condición.
Los pacientes diabéticos tipo 2 quienes tiene una función endotelial más alterada que la de la población general, son un grupo que podría resultar particularmente beneficiado de la intervención y corrección de los factores de riesgo cardiovascular.
Estudios a éste respecto, con mayor cantidad de pacientes, deben realizarse en los años por venir, que nos aclaren cuáles son los tipos de intervención de los cuales se obtendrá mayor beneficio para los pacientes.
Bibliografía ]]>
1. Fein F, Scheir J. Heart Disease in Diabetes Mellitus: Theory and practice. Rifkin H, Porte J, Editors. New York : Elsevier 1990: 821-23. [ Links ]
2. Sementovich CF, Heinecke JW. The mystery of diabetes and atherosclerosis. Diabetes 1997; 46: 327-34. [ Links ]
3. Cohen RA. Disfunction of vascular endothelium in Diabetes Mellitus. Circulation 1993; 87 Suppl V: V 67-76. (11-14) [ Links ]
4. Winocour PP. Platelet anormalities in diabetes mellitus. Diabetes 1992; 41 Suppl. 2: 26-31. [ Links ]
5. Reaven GM. Role of insulin resistance in human disease. Diabetes 1988; 37: 1595-607. [ Links ]
6. Godsland IK. Stevenson JC. Insulin Resistance: Syndrome or tendency? Lancet 1995; 346: 100-3. [ Links ]
7. Ross R. Atherosclerosis and inflammatory disease. N. Eng. J. Med.; 312: 744-45. (27-28) [ Links ]
8. Hasdai D, Holmes DR. Jr, Garret KN, et al. Mechanical pressure and stress release endothelin 1 from human atherosclerotic coronary arteries in vivo. Circulation 1997; 95 : 357-62. [ Links ]
9. Celermajer DS, Sorensen KE, Goock WM, et al. Non invasive detection of endothelial disfunction in children and adults at risk of atherosclerosis. Lancet 1992; 340: 1111-5.(32) [ Links ]
10. Celermajer D, Sorensen K, Bull C, et al. Endothelium dependent vasodilatation in the systemic arteries of asymptomatic subjects relates to coronary risk factor and their interaction. J. American Coll. Cardiol. 1994; 24: 1468-74.(35) [ Links ]
11. McLenachan SM, Vita J, Fish RD, et al. Early evidence of endothelial vasodilator disfunction at coronary branch points. Circulation 1990; 82:1169-73. (39) [ Links ]
12. Osborne A, Lento PH, Sigfried MR, et al. Cardiovascular effects of acute hypercolesterolemia in rabbits, reversal with lovastatin treatment. J. Clin. Invest. 1989; 83: 465-73. (40)
13. Ross R. The pathogenesis of atherosclerosis a perspective for the 1990s. Nature 1993; 44: 406-12 (25) [ Links ]
14. Jensen-Ustar KJ, Reichard DE, Rosfors JJ, et al. Early atherosclerosis is retarded by improved blood glucose control in patients with IDDM. Diabetes 1996; 45: 1253-58 (41) [ Links ]
15. Lanbert S, Aarsen M. Denker AJM, et al. Endothelium dependent and independent vasodilatation of large arteries in normoalbuminuric IDDM. Artheriosescler. Thromb. Vasc. Biol. 1996; 16: 705-11. (42) [ Links ]
16. Goodfellow J, Ramsey MW, Luddintong LA, et al. Endothelium and inelastic arteries: and early marker of vascular disfunction in non insulin dependent diabetes mellitus. BMJ; 312: 744-45. (38) [ Links ]
17. Kawano H. Motoyama T, Hiroshima O, et al. Hyperglicemia rapidly suppresses FMD dependent vasodilatation of brachial artery. J. Am. Coll. Cardiol. 1999; 39: 146-54. [ Links ]
18. Balletshofer BM, Rittig K, Enderle MD, et al. Endothelial dysfunction is detectable in young normotensive first degree relatives of subjects with type 2 diabetes in association with insulin resistance. Circulation 2000; 101: 1780-84. [ Links ]
19. Wilmink HW, Banga JP, Hijmering MD, et al. Effect of ACE inhibition and AT-II type 1 receptor antagonism on postprandial endothelial function. J. Am. Coll. Cardiol. 1999; 39: 140-5. (43-45)
20. Kavin M, Barnes PJ. Mechanisms of Disease : Nuclear transcription factor (Kappa) b a pivotal transcription factor in chronic inflammatory diseases. N. Eng. J. Med. 1997; 336: 1066-1071. [ Links ]
21. Zeiher AM, Fisstthaler B, Scrhay- Utz B, et al. NO modulates the expression of monocite chemoattractant protein 1 in cultured human endothelial cells. Circ. Res. 115; 76: 980-86. [ Links ]
22. Zeiher AM. Endothelial vasodilation dysfunction pathogenetic link to myocardial ischemia or epiphenomenona? Lancet 1996; 348 (Suppl. 1): 510-12. [ Links ]
23. Cannon RO. Cardiovascular benefit of cholesterol lowering therapy does improved endothelial vasodilator function matter. Circulation 2000; 102: 820-22. (46-49) [ Links ]
24. Hamnoud T, Tanguay JF, Bourassa MG. Management of coronary artery disease: Therapeutic options in patients with diabetes. J. American Coll. Cardiol. 2000; 36: 355-65. [ Links ]
25. Mancini GBJ, Henry GC, Macaya C, et al. ACE inhibition with quinapril improves endothelial vasomotor dysfunction in patients with coronary artherioesclerotic disease. TREND study.Circulation 1996; 54: 258-65. [ Links ]
26. O Driscoll G, Green D, Maiorana A, et al. Improvement in endothelialfunction by angiotensin convertoing enzyme inhibition in NIDDM. J. Am. Coll. Cardiol. 1999; 33: 1506 [ Links ]
27. HOPE investigators. Effects of an angiotensin converting enzyme inhibition, ramipril, on cardiovascular events in high risk patients. N Engl J Med 2000; 342:145-53. [ Links ]
28. HOPE study investigators. Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and micro-HOPE substudy. Lancet 355: 253-259.(52-53) [ Links ]
* Departamento de Cardiología,Hospital Calderón Guardia,C.C.S.S.,San José,Costa Rica. ]]>
** Departamento de Imágenes Médicas Hospital México, C.C.S.S., San José, Costa Rica. ]]>