Original
Predictores de parto pretérmino en la población adolescente
(Predictors of preterm delivery in adolescents)
Manrique Leal-Mateos1* y Loretta Giacomín-Carmiol2*
Objetivo: identificar los principales factores de riesgo que inducen un parto pretérmino en pacientes adolescentes.
Métodos: se realizó un estudio observacional de corte transversal, mediante el análisis secundario de la base de datos del estudio original “Características del control prenatal de pacientes adolescentes atendidas en la consulta de obstetricia. Hospital Rafael Ángel Calderón Guardia, 2010”. Las variables relacionadas con el control prenatal se categorizaron según la dicotomía Sí/ No, y mediante una regresión logística, se estimó la razón de probabilidades ajustada en cuanto a la presencia de parto pretérmino.
Resultados: la edad promedio de las pacientes fue de 16,6 años (DE + 1,6). El parto pretérmino se presentó en el 13,3% de los casos (n = 48, IC 95% 10,1- 17,4). Las enfermedades médicas asociadas al embarazo (OR 3,5, IC 95% 1,3-9,6), la multiparidad (OR 3,6, IC 95% 1,3-10,3) y la falta de un control prenatal adecuado (OR 10,1, IC 95% 3,2-32,3) fueron las principales variables independientes para la presencia de un parto pretérmino.
Conclusiones: las enfermedades médicas asociadas al embarazo, la presencia de 2 o más embarazos y la falta de un control prenatal adecuado, fueron las principales variables independientes para la predisposición a un parto pretérmino en la población de adolescentes.
Descriptores: embarazo, adolescentes, control prenatal, parto pretérmino
Abstract
Aim: To identify the risk factors for preterm delivery in pregnant adolescents during their prenatal care.
Methods: An observational cross-sectional study was conducted through secondary analysis of the data base from the original study “Characteristics of prenatal care of pregnant adolescents, Obstetrics Department of the
Results: The mean age of the patients was 16.6years (SD±1.6). Preterm delivery occurred in 13.3% of the cases (n= 48, 95% CI 10.1 to 17.4). The medical illnesses associated to pregnancy (OR3.5, 95% CI 1.3 to 9.6), two or more pregnancies (OR3.6, 95% CI 1.3 to 10.3) and the lack of adequate prenatal care(OR 10.1, 95% CI 3.2 to 32.3) were the main independent variables for preterm labor.
Conclusions: Medical illnesses associated to pregnancy, two or more pregnancies and the lack of adequate prenatal care are the main independent variables in preterm labor in the adolescent population.
Keywords: Pregnancy, adolescent, prenatal care, preterm delivery.
El embarazo en adolescentes es considerado factor de riesgo para un parto pretérmino. La mayoría de la evidencia muestra que el bajo peso al nacer y el parto antes de las 37 semanas, son las posibilidades más frecuentes en la madre adolescente.1-4
En 2012 se publicaron las estadísticas de la Clínica de Adolescentes del Servicio de Obstetricia del Hospital “Dr. Rafael Ángel Calderón Guardia” (HCG), en las cuales se mostraba que el 16,5% de las madres adolescentes eran hospitalizadas durante su embarazo, y que la principal causa de hospitalización era la amenaza de parto pretérmino. Asimismo, indicaron que, a pesar del esfuerzo del personal de salud, el 62,5% de las pacientes internadas por esta causa, ingresaron al Servicio en la fase activa de su labor y tuvieron su parto antes de las 37 semanas.5
Por tanto, el estudio tiene como objetivo principal identificar la presencia de algunos factores de riesgo reconocidos durante el control prenatal, que ayuden a identificar, predecir o establecer pronóstico de forma temprana a las pacientes con posibilidad de un parto pretérmino.
Se realizó un estudio observacional de corte transversal, mediante el análisis secundario de la base de datos del estudio original “Características del control prenatal de pacientes adolescentes atendidas en la consulta de obstetricia. Hospital Rafael Ángel Calderón Guardia, 2010”. 5 La investigación contó con la aprobación del Comité de Ética del Hospital (Oficio CLOBI-47-12-2013).
Los factores de riesgo históricamente establecidos para un parto pretérmino en la paciente adolescente, y que pudieron ser identificados mediante el control prenatal fueron: edad menor de 15 años, estado civil, riesgo familiar, embarazo planeado, índice de masa corporal (IMC) pregestacional, tabaquismo, paridad, anemia, enfermedades médicas asociadas o inducidas por el embarazo, bacteriuria asintomática, infección urinaria, control prenatal inadecuado y falta de recibo del curso de preparación para el parto.
Para la evaluación del riesgo familiar de cada paciente, se utilizó el test denominado APGAR familiar, el cual valora la adaptación, participación, gradiente de crecimiento, afecto y resolución familiar en cada paciente adolescente.6
El control prenatal se clasificó como adecuado si se presentó de forma precoz (primera cita de control prenatal en primer trimestre), con al menos 5 citas de control durante el embarazo y basado en un enfoque de riesgo.10
Se utilizó el programa EpiInfo 2002 para el procesamiento de los datos. Las variables cualitativas se analizaron mediante frecuencias y proporciones. Los resultados derivados de las variables cuantitativas se expresaron mediante medidas de tendencia central (promedio) y de dispersión (desviación estándar). La relación entre variables cualitativas se efectuó mediante la prueba estadística de Chi cuadrado (x2).
Posteriormente, cada una de las variables se categorizó de forma dicotómica, según su presencia (Sí/No) y se calculó la razón de probabilidades ajustada (OR), mediante una regresión logística.
Resultados
Del total de las 360 pacientes estudiadas, el promedio de edad fue de 16,6 años (desviación estándar (DE) + 1,16). El 3,1% (n=11; intervalo de confianza (IC) 95% 1,6-5,6) presentó edades menores de 15 años.
El 56,1% (n=202; IC del 95% 50,8-61,3) de las pacientes se encontraba solteras al momento de su primera cita de control prenatal. El 79,2% (n=285; IC 95% 74,6-83,2) reportó su embarazo como “no planeado”. Se identificó a 234 pacientes (65%; IC 95% 59,8-69,8) con antecedentes de riesgo familiar, siendo el más frecuente el de padres divorciados, con un 25,8% (n=93; IC 95% 21,6-30,7) de los casos. La prevalencia del consumo de tabaco fue del 18,1% (n=65; IC 95% 14,3-22,5).
En relación con su control prenatal, el 89,7% (n=323; IC 95% 86,1-92,7) de las pacientes cursaba con su primer embarazo. El periodo intergenésico de las pacientes con 2 o más embarazos fue de 11 meses (rango 6-24). El 94,4% (n=340; IC 95% 91,4-96,5) contó con un control prenatal adecuado y únicamente el 59,2% (n=213; 53,9-64,3) participó en el curso de preparación para el parto.
Únicamente el 62,6% (n=221; IC 95% 57,3-67,7) presentó un índice de masa corporal (IMC) pregestacional normal. La ganancia promedio de peso durante el embarazo fue de 12,1 Kg (DS + 4,7). El 12,2% (n=44; IC 95% 9,1-16,2) de las pacientes presentó anemia. El valor promedio de hemoglobina preparto fue de 12,3 g/dl (DS + 0,97). El 25,8% (n=93; IC 95% 21,430,7) presentó bacteriuria asintomática y el 31,1% (n=112; IC 95% 24,4-36,2) necesitó ser tratado por infecciones del tracto urinario. El 64,2% (n=231; IC 58,9-69,1) presentó alguna condición médica previa al embarazo, o inducida por este, que pudiera influir en la posibilidad de un parto pretérmino.
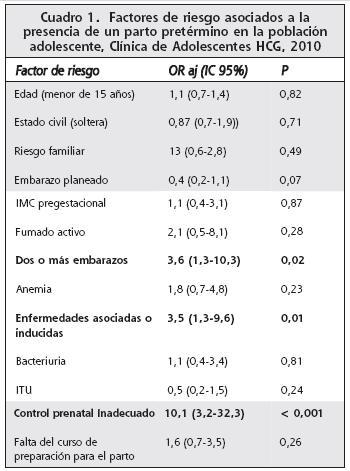
El Cuadro 1 muestra la razón de probabilidades ajustada (OR aj) para las variables de estudio.
Las enfermedades médicas asociadas o inducidas al embarazo (OR 3,5, IC 95% 1,3-9.6), la presencia de 2 o más embarazos (OR 3,6, IC 95% 1,3-10,3) y un control prenatal inadecuado (OR 10,1, IC 95% 3,2-32,3), fueron las principales variables independientes para ocasionar un parto pretérmino en la población adolescente.
Al igual que el estudio original, este muestra los resultados obtenidos en las pacientes que asistieron a la consulta de adolescentes del HCG en el año precedente a la ejecución de la investigación. Al ser un estudio de base hospitalaria y no poblacional, los resultados son aplicables únicamente a las pacientes atendidas en el HCG.
Al utilizar historias clínicas de los expedientes médicos de las pacientes como fuente de datos, el estudio no se encuentra libre de sesgos de información.
Con estas limitaciones metodológicas, se muestra como mediante un control prenatal adecuado, se pueden identificar diferentes factores de riesgo que, siendo intervenidos de forma temprana, podrían reducir la prevalencia de un parto pretérmino en la población adolescente.
Diferentes autores ya han identificado varios factores de riesgo asociados a la prematuridad en la madre adolescente. Algunos, incluso este estudio, determinaron como un control prenatal inadecuado el factor de riesgo de mayor peso, para provocar la propensión al parto prematuro y sus complicaciones.1-4
A pesar de esto, es importante resaltar que este principal factor de riesgo es sujeto de reducción o eliminación por parte de personal de salud de la CCSS. Los Equipos Básicos de Atención Primaria, mediante la visita domiciliar, podrían identificar tempranamente a las adolescentes embarazadas y remitirlas a los centros de salud para que inicien de forma oportuna su control prenatal. Lo anterior ayudaría también al reconocimiento temprano de signos y síntomas que sugieran la presencia o descompensación de enfermedades médicas asociadas o inducidas por el embarazo, y que son causa de la predisposición de las adolescentes al inicio prematuro de la labor de parto.
En relación con la paridad como factor de riesgo,7,8 estos mismos equipos básicos de atención podrían captar en el postparto a estas pacientes, para que inicien o asistan a las consulta de anticoncepción y prevengan nuevos embarazos.
Por tanto, el esfuerzo que pueda hacer el personal de salud para garantizarle a la madre adolescente un control prenatal adecuado y la prevención de un segundo embarazo, parecen ser las estrategias más importantes en la previsión de un parto pretérmino. Según la Organización Mundial de Salud, en su monografía sobre el Embarazo en Adolescentes, de 2008, y otras publicaciones,9 las medidas dirigidas al acceso oportuno al control prenatal y a los métodos de planificación familiar actuales, podrían tener un impacto positivo en los resultados adversos que presenta el embarazo en adolescentes.
Conflicto de interés: los autores declaran que no tienen asociaciones comerciales que puedan significar un conflicto de interés con el artículo sometido a valoración.
Referencias
1. Fraser AM, Brockert JE, Ward RH. Association of Young maternal age with adverse reproductive outcomes. NEJM 1995; 332:1113-1117. [ Links ]
2. Chen XK, Wen SW, Fleming N, Demissie K, Rhoads G, Walker M. Teenage pregnancy and adverse birth outcomes: A large population based retrospective cohort study. Int J Epidemiol. 2007;36:368-373. [ Links ]
3. Malabarey OT, Balaya J, Klam SL, Shrim A. Pregnancies in Young adolescent mother: A population-based study on 37 million births. J Pediatr Adolesc Gynecol. 2012;25:98-102. [ Links ]
4. Leppälathi S, Gissler M, Mentula M, Heikinheimo O. Is teenage pregnancy an obstetric risk in welfare society? A population-based study in
5. Giacomin-Carmiol L, Leal-Mateos M. Características
6. Smilkstein G. The physician and family function assessment. Fam Systems Med. 1984;2:263-278. [ Links ]
7. Blankson ML, Cliver SP, Goldenberg RL, Hickey CA, Jin J, Dubard MB. Health behavior and outcomes in sequential pregnancies of black and white adolescents. JAMA. 1993;269:14013. [ Links ]
8. Smith GC, Pell JP. Teen pregnancy and risk of perinatal outcomes associated with first and second birth: Population based retrospective cohort study. BMJ. 2001;323:1-5. [ Links ]
9. Tocce KM, Jeanelle L, Teal S. Rapid repeat pregnancy in adolescents: Do immediate postpartum contraceptive implants make a difference? Am J Obset Gynecol. 2012;206:e1-e7. [ Links ]
10. Caja Costarricense de Seguro Social. Guías de atención integral de las mujeres, niños y niñas en el periodo prenatal, parto y postparto. Caja Costarricense de Seguro Social, San José, Costa Rica, Unidad de Imprenta CCSS, 2009. [ Links ]
Afiliación de los autores:
Fuentes de apoyo: este estudio no posee una fuente de financiamiento externa a la CCSS.
Fecha recibido: 19 de marzo de 2014 Fecha aprobado: 23 de octubre de 2014
{kind=link}