Introducción: La importancia del análisis de la variabilidad de la frecuencia cardíaca (VFC) está bien establecida como marcador pronóstico en pacientes que han tenido infarto agudo de miocardio y en otras cardiopatías. El objetivo de este estudio es establecer la correlación entre las variables de VFC y los índices pronósticos tradicionales en angina inestable
Materiales y Métodos: Se reclutaron prospectivamente pacientes con diagnóstico de angina inestable. Se consignaron indicadores de riesgo cardiovascular clínicos (angor de reposo refractario, hipotensión arterial, insuficiencia cardíaca), presencia de cambios dinámicos en el ST-T, fracción de eyección =40% y los hallazgos angiográficos (2 ó más vasos), conformándose entonces dos grupos, de alto riesgo y de bajo riesgo. A todos los pacientes se les realizó un registro electrocardiográfico de 5 minutos y se analizaron diversas variables de VFC en dominio de tiempo y de frecuencia mediante un programa de computadora.
Estas variables se compararon entre ambos grupos.
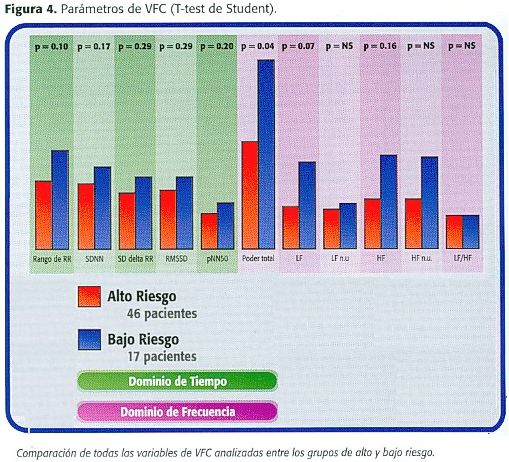
Resultados: Se reclutaron 63 pacientes (44 hombres, 70%) con edad promedio de 63 + 10.4 años (35-90); 46 se consideraron de alto riesgo por cambios electrocardiográficos dinámicos y la fracción de eyección disminuida y 17 de bajo riesgo. En el primer grupo, el poder espectral total fue significativamente menor que en el grupo de bajo riesgo (p=0.04). La banda de baja frecuencia mostró diferencia pero sin alcanzar significancia estadística (p=0.07) y otras variables como el SDNN, el NN50 y la banda de baja frecuencia, mostraron sólo tendencia de ser menores en el grupo de alto riesgo. ]]>
Conclusión: En pacientes con angina inestable de alto riesgo, la presencia de indicadores pronósticos tiene correlación con una menor VFC en dominio de frecuencia.Palabras Clave: Variabilidad, frecuencia cardíaca, angina inestable.
Abstract
Introduction: The usefullness of heart rate variability (HRV) analysis is well known in myocardial infarction as in other cardiac diseases as a prognostic tool. The primary goal of this study is to determine HRV relationship with other prognostic markers in unstable angina patients.
Materials and methods: We studied prospectively patients with diagnosis of unstable angina. We considered predictors of cardiovascular risk (unresponsive rest angina, hipotension, heart failure, dynamic ST changes, ejection fraction less than 40% and angiographic features (2 or more vessels), conforming two groups, high risk and low risk. In every patient was made a 5 minute electrocardiographic recording and we analysed HRV variables in time domain and frequency domain. All this variables were compared between both groups
Results: We included 63 patients (44 males, 70%) with mean age 63 + 10.4 years old (35-90); 46 were considered of high risk because dynamic ST changes and depressed ejection fraction and the remaining 17 were considered at low risk. In the first group, total spectral power was statistically different (p=0.04) compared with low-risk group. Low frequency band (LF) was also different but without statistic significance (p=0.07) and other variables like SDNN, NN5 0 and low frequency showed only a trend to be less in the high-risk group.
Conclusion: Clinical high-risk patients with unstable angina have low HRV variables. This feature could be predictive of poor survival in follow-up prospective studies.
Key words: .
Introducción ]]>
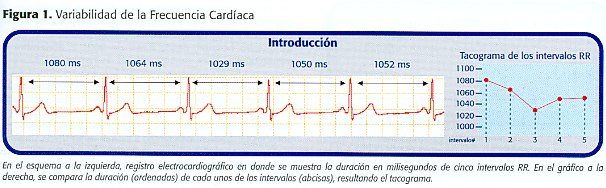
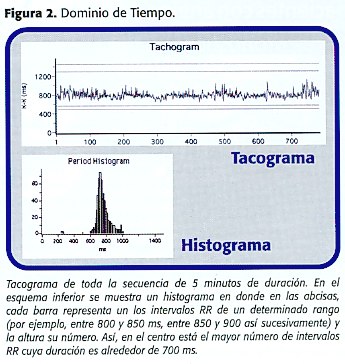
Las variaciones en la duración que hay entre latido y latido cardíacos se denominan "variabilidad de la frecuencia cardíaca" (VFC, figura 1) . Si se analiza el comportamiento de estas variaciones a lo largo del día, estas serán más notorias en el período post-prandial y en la noche, períodos en los cuales hay predominio fisiológico del tono autonómico parasimpático. Por el contrario, en situaciones en las que predomina el tono simpático ellas serán menos marcadas (1).Hay muchas formas de cuantificar la VFC. La más sencilla es medir cada uno de los intervalos RR a lo largo de un período de tiempo y calcular variables aritméticas como el RR más largo, el más corto, el promedio de todos los RR y el número de intervalos RR consecutivos que se diferencien en más de 50 ms. Otros cálculos más sofisticados son las variables estadísticas como el desvío estándar de las variaciones de todos lo RR en un período dado de tiempo o el desvío estándar de las diferencias entre los intervalos RR. Las variables aritméticas y estadísticas se denominan en conjunto, variables "en dominio de tiempo". Todos estos cálculos de pueden representar también gráficamente (figura 2).
Se ha demostrado que el estudio de la VFC tiene utilidad pronóstica al momento de dar el alta al paciente que ha tenido un infarto o una descompensación hemodinámica (2). Hay una relación directa entre VFC disminuida y la sobrevida en estas condiciones (2,7). También se ha estudiado la VFC en otras afecciones cardiovasculares como la miocardiopatía hipertrófica, el síncope neurocardiogénico, el prolapso de la válvula mitral, los pacientes con trasplante cardíaco, la miocardiopatía chagásica entre otras (8) y en situaciones no cardiológicas como la neuropatía diabética (10). Hay menos evidencia del comportamiento de la VFC en pacientes que ingresan al hospital con angina inestable. El objetivo de este estudio es establecer la correlación entre las variables de VFC y los índices pronósticos tradicionales en angina inestable.
Materiales y Métodos
Pacientes: Es un estudio prospectivo abierto en el que se reclutaron consecutivamente pacientes con diagnóstico de angina inestable: angina prolongada y/o de reposo, de reciente comienzo y progresiva, internados en la sección de medicina de nuestro hospital, desde mayo de 2001 a noviembre del mismo año.
Se excluyeron a los que durante su hospitalización se diagnosticó infarto agudo de miocardio (con o sin elevación ST), a quienes en la coronariografía (previa o posterior a su inclusión) se documentó arterias coronarias angiográficamente normales y aquellos quienes en los últimos 2 meses se hubieran sometido a procedimientos de revascularización miocárdica (cirugía o angioplastía). También fueron excluídos quienes se negaron a participar en el estudio.
Los siguientes, fueron los indicadores clínicos considerados como marcadores de riesgo cardiovascular intrahospitalario en angina inestable:
- angor de reposo refractario
- hipotensión arterial
- insuficiencia cardíaca
- presencia de cambios dinámicos en el ST-T ]]>
En todos los pacientes se consignaron estos indicadores y se agruparon en dos poblaciones: el grupo de alto riesgo si tenía uno o más de estos indicadores, y el de bajo riesgo si no cumplía ninguno de los indicadores mencionados.
Registro electrocardiográfico: A todos los pacientes se les realizó un registro electrocardiográfico de 5 minutos, en condiciones de reposo, respiración no controlada, en horas de la mañana (8:30 - 11:30 am) para lo cual se utilizó un equipo multiregistrador PowerLab 4SP con bioamplificador y una computadora iBook (Apple®), el programa de computadora Chart v 4.0.1 (ADInstruments) y su extensión "análisis de variabilidad de frecuencia cardíaca" a una velocidad de adquisición de 1000 Hertz.
Otros exámenes auxiliares: Los electrocardiogramas se realizaron con la metodología convencional de doce derivaciones estándar. Los ecocardiogramas fueron realizados por cardiólogos no invasivos de nuestro centro en forma ciega, utilizando una valoración subjetiva para el cálculo de la fracción de eyección. Las coronariografías se realizaron con la metodología convencional por cardiólogos hemodinamistas de nuestro centro en forma ciega.
Análisis de los Registros: Se realizó mediante el programa de computadora referido, utilizando las siguientes variables en dominio de tiempo:
Variables aritméticas:
- NN promedio (promedio de todos los RR o NN)
- NN max (el máximo valor encontrado en un RR)
- NN min (el mínimo RR encontrado) ]]>
- SDNN (desvío estándar de todos los RR)
- NN50 (intervalos RR que se diferencien en 50 ms o más)
- pNN50 (el anterior expresado en porcentaje)
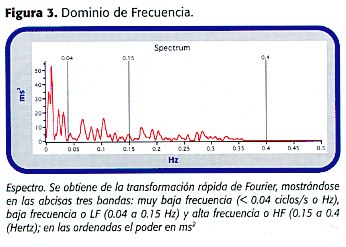
Utilizando transformación rápida de Fourier, se consideraron las siguientes variables en dominio de frecuencia:
- Poder total
- VLF (banda < 0.04 Hz)
- LF (banda comprendida entre 0.04 y 0.15 Hz)
- HF (banda comprendida entre 0.15 y 0.4 Hz)
- relación LF/HF ]]>
Resultados
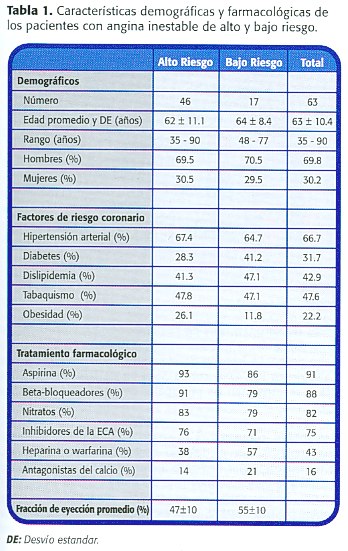
Se reclutaron 63 pacientes (44 hombres) con edad promedio de 63 + 10.4 años (35-79); 46 se consideraron de alto riesgo, todos incluidos por los criterios cambios electrocardiográficos dinámicos y fracción de eyección disminuida. Ningún paciente presentó hipotensión, insuficiencia cardíaca o angina refractaria. Los 17 pacientes restantes se consideraron en el grupo de bajo riesgo por no reunir ninguno de los criterios utilizados en este estudio. Del total de pacientes, 41 tuvieron datos de la coronariografía, 33 de los cuales se incluyeron en el grupo de alto riesgo. La fracción de eyección promedio en el grupo de alto riesgo fue 47%, contra 55% en de bajo riesgo. En la tabla 1 se consignan las principales características de ambos grupos.
Aunque los resultados demuestran que existe correlación entre los indicadores clínicos y la VFC, el poder estadístico depende en forma directa del tamaño de la muestra.
Esta población está preseleccionada ya que en nuestro hospital los pacientes críticamente enfermos se internan en áreas de cuidados críticos, sin embargo la información obtenida es útil para el sistema de trabajo del centro hospitalario.
En este estudio no se analizó si esta correlación clínica con VFC es independiente de la fracción de eyección por análisis multivariado, aunque se conoce que ésta es muy sensible pero poco específica. El análisis de VFC es un excelente complemento que puede aumentar el poder predictivo de eventos cardiovasculares, hecho que se ha comprobado en otros estudios.
Conclusión
En pacientes con angina inestable de alto riesgo, la presencia de indicadores pronósticos tiene correlación con una menor VFC en dominio de frecuencia. Este hallazgo sugiere que en estudios de seguimiento, este método podría ser predictivo de menor sobrevida. ]]>
Referencias1. Landsberg L, Young J. Fisiología y farmacología del sistema nervioso autónomo. En: Isselbacher K, Braunwald E, Wilson J D, Martin J, Fauci A, Kasper D, ed. Principios de medicina interna de Harrison. 13ª ed. España: Interamericana-Mc Graw-Hill, 1994: vol 1: 481-497.
2. Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. ATRAMI (Autonomic Tone and Reflexes After Myocardial Infarction) Investigators.Lancet. 351(9101):478-84, 1998
3. BHAT ß-Bloquer Heart Attack Trial Research Group. A Randomizad Trial of Propranolol in Patients with Acute Myocardial Infarction, I.Mortality Results. JAMA 1982;247:1707-1714 [ Links ]
4. The ISIS-1 investigators. First International Study of Infarct Survival (ISIS-1). Lancet 1986; 2 (8498):57-66. [ Links ]
5. Packer M, Coats AJS, Fowler MB, et al. for the Carvedilol Prospective Randomized Cumulative Survival Study Group. N Engl J Med 2001;334:1651-8. [ Links ]
6. Cleland JG. Beta-blockers for heart failure: why, which, when, and where. Med Clin North Am 2003; 87(2): 339-71 [ Links ]
7. Bigger JT., Fleiss JL., Steinman RC., Rolnitzky LM., Kleiger RE., Rottman JN.: Correlations Among Time and Frequency Domain Measures of Heart Rate Variability Two Weeks After Acute Myocardial Infarction. Am J Cardiol 1992;69: 891-898
8. Gutiérrez O. Variabilidad de la frecuencia cardíaca. Aplicaciones en cardiología. Cardiología al día (Bucaramanga, Colombia) 2001; 4: 11-18 [ Links ]
9. Task force Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology: Heart Rate Variability: Standard of Measurement, Physiological Interpretation and Clinical Use. Circulation 1996; 93:1043-1065) [ Links ]
10. Gutiérrez O, Putvinsky A, Padilla J, Ramírez C, Mora C. Variabilidad de la Frecuencia Cardíaca en individuos sanos costarricenses. Revista Costarricense de Cardiología 2000; 2: 4-12 [ Links ]
11. Gutiérrez O. Variabilidad de la Frecuencia Cardíaca en individuos sanos costarricenses. Revista Costarricense de Cardiología 1999; 11:3-10 [ Links ]
12. Catipovic-Veselica K, Durijancek J, Bracic-Kalan M, Amidzic V, Mrdenovic S, Kozmar D, Buri D, Catipovic B .Heart rate and heart-rate variability in patients with acute coronary heart disease classified on Bortners scale as type A and type B. Psychol Rep 1997; 80:775-84 (abstract)
13. Loricchio ML, Di Clemente D, Saccone V, Caccamo L, Borghi A, Bugiardini R. An analysis of the variability of the heart rate and its significance in the risk stratification of patients with unstable angina. Cardiologia 1994; 39:335-43
14. Huang J, Sopher SM, Leatham E, Redwood S, Camm AJ, Kaski JC. Heart rate variability depression in patients with unstable angina. Am Heart J 1995; 130:772-79
15. Manfrini O, Pizzi C, Trerè D, Fontana F, Bugiardini R.Parasympathetic failure and risk of subsequent coronary events in unstable angina and non-ST-segment elevation myocardial infarction. Eur Heart J 2003;24:1560-6
16. Catipovic-Veselica K, Durjancek J, Amidzic V, Buric D, Kozmar D, Vizner-Lovric I. Heart rate and heart rate variability in acute coronary heart disease. Acta Med Croatica 1996 50:75-9 (abstract)
17. Lanza GA; Pedrotti P; Rebuzzi AG; Pasceri V; Quaranta G; Maseri A. Usefulness of the addition of heart rate variability to Holter monitoring in predicting in-hospital cardiac events in patients with unstable angina pectoris. Am J Cardiol 1997; 80(3): 263-7
18. Wennerblom B, Lurje L, Westberg S, Johansson M, Lomsky M, Vahisalo R, Hjalmarson A. Effects on heart rate variability of isosorbide-5-mononitrate and metoprolol in patients with recent onset of angina pectoris. Cardiology 1998 89:87-93
19. Dovgalevsky PY, Rybak OK, Furman NV. Relationship between parameters of heart rate variability, angiographical severity of coronary atherosclerosis and functional class of angina in patients with ischemic heart disease. Kardiologiia 2002 42:17-20 (Abstract) ]]>
20. Wennerblom B, Lurje L, Tygesen H, Vahisalo R, Hjalmarson A. Patients with uncomplicated coronary artery disease have reduced heart rate variability mainly affecting vagal tone. Heart 2000 Mar 83:290-4 ]]>