Etiología de la insuficiencia mitral pura en Costa Rica.
Estudio ecocardiográfico
]]>
Dra. Esquivel M. Lidieth, Dr. Romero Luis, Dr. Vásquez Gerardo, Dr. Gutiérrez Oswaldo*
Resumen
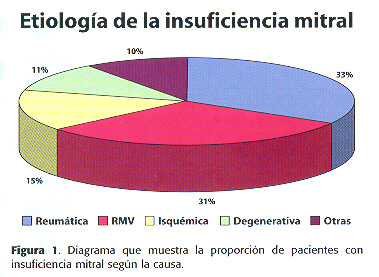
Introducción: Estudios internacionales recientes han mostrado que en la actualidad la insuficiencia valvular mitral se debe principalmente a degeneración mixomatosa de la válvula o a enfermedad arterial coronaria. Este estudio ecocardiográfico tiene como objetivo establecer la prevalencia ]]>
Metodología: Se incluyeron a todos aquellos pacientes referidos a nuestro laboratorio de eocardiografía en el período comprendido entre el mes de julio de 1998 y julio del 2000 en quienes se detectó insuficiencia mitral de causa orgánica. Se realizó la exploración en modo M, bidimensional y con las técnicas de mapeo con doppler ]]>
Resultados: Se incluyeron ]]>
]]>
Conclusión: En esta serie encontramos prevalencia similar de la causa reumática y el prolapso de la valvula mitral mixoide, las más frecuentes de insuficiencia mitral pura a diferencia de otras series internacionales. La causa isquémica ocupó el tercer lugar. La mayoría de los casos fueron leves a moderadas y de los casos con insuficiencia mitral severa, se dió la misma proporción.
]]>
Palabras Claves
Insuficiencia Mitral Pura, Costa Rica.
]]>
Abstract
Introduction: International studies have demonstrated that mitral valve mixoid degeneration and coronary ]]>
Methods: We included all patients referred to our institution since July 1998 to July 2000 in whom was detected organic pure mitral regurgitation. We performed M-mode and bidimensional imaging and pulsed, continuous and colour flow mapping ]]>
Results: We studied 82 patients, 48 females (59.7%) and 34 males (37.8%) between 14 and 87 years ]]>
]]>
Conclusion: In this study we find a similar prevalence of rheumatic disease and mixoid degenerative disease as most frequent causes of mitral regurgitation, a fact different from international series. Coronary artery disease was the third cause. Most cases were mild or moderate and severe cases had a similar distribution.
]]>
Key word
Pure Mitral Insufficiency.
]]>
Introducción
El cierre sistólico normal de la válvula mitral depende de la función integrada de las valvas mitrales, las cuerdas tendíneas, los músculos papilares y el miocardio izquierdo subyacente. El fallo de cualquiera de estos componentes puede llevar a cierre valvular incompleto y la consiguiente insuficiencia valvular mitral. Las causas de insuficiencia mitral producidas por alteraciones ]]>
Estudios recientes han mostrado que en la actualidad la enfermedad reumática valvular ya no es la principal causa de insuficiencia mitral aislada (1 ,2 ), como consecuencia de la mejoría en las condiciones socioeconómicas ]]>
3 ,4 ) y la enfermedad coronaria se encuentran entre las causas actualmente más prevalentes (1 ,2 ,5 ) y la enfermedad degenerativa ]]>
5 ). Otras causas incluyen las secuelas de la endocarditis bacteriana, enfermedades del colágeno como el lupus eritematoso sistémico, el síndrome carcinoide y fármacos como la combinación de fenfluramina y fentermina (anorexígenos). También se presenta como consecuencia funcional de miocardiopatías como la hipertrófica y la restrictiva o por dilatación del anillo como en la dilatada (6 ).
]]>
La evolución natural de la enfermedad es variable y depende de la causa subyacente, el volumen de reflujo y el estado del miocardio. En pacientes con insuficiencia mitral leve asintomáticos la enfermedad permanece estable durante muchos años; la insuficiencia mitral grave representa un pequeño porcentaje del total, en algunos casos precipitada por endocarditis infecciosa adicional o a rotura de las cuerdas tendinosas. La insuficiencia mitral tiende a avanzar más rápidamente en pacientes con enfermedad ]]>
En las últimas décadas, ]]>
Metodología
]]>
Pacientes: se incluyeron a todos aquellos pacientes referidos a nuestro laboratorio de eocardiografía en el período comprendido entre el mes de julio de 1998 y julio del 2000 en quienes se detectó insuficiencia mitral de causa orgánica. Se excluyó a todos los pacientes en quienes el hallazgo estuviera asociado a estenosis mitral u otras lesiones valvulares o secundaria a otras condiciones como miocardiopatías (hipertrófica o restrictiva) ]]>
Se utilizó un equipo ATL Ultramark 9 HDI y se les realizó la exploración en modo M, bidimensional y con las técnicas de mapeo con doppler pulsado, continuo y color. Se recolectó la información concerniente a las características estructurales ecocardiográficas de las válvulas, que permitiera clasificar los casos según la ]]>
Definiciones
]]>
Se definió como insuficiencia mitral la presencia de un flujo sistólico turbulento de alta velocidad dirigido hacia el atrio izquierdo. Se estimó la severidad por mapeo con doppler-color según el ancho del flujo regurgitante y el área comprometida en el atrio izquierdo.
]]>
Se utilizaron criterios convencionales para calificar la etiología de la dolencia como reumática, isquémica, mixomatosa, degenerativa u otra.
Se consideró reumática cuando se observó en el ecocardiograma bidimensional pérdida de tejido valvar por fibrosis con acortamiento, deformación a predominio ]]>
Se consideró insuficiencia mitral causada por válvula mixoide a aquella con engrosamiento y redundancia uni o bivalvar, con o sin prolapso, definido éste como desplazamiento del cuerpo de la valva o las valvas de 2 mm o más ]]>
Se consideró como insuficiencia mitral degenerativa a la que presentó engrosamiento, esclerosis y datos indicativos de fibrosis y/o calcificación de la válvula y/o del anillo mitral.
]]>
Se consideró como secundaria a endocarditis a la que presentó pérdida de tejido o ruptura del aparato subvalvular, vegetaciones, definidas como masas irregulares adyacentes a la estructura valvular y que oscilan a alta frecuencia, además de un cuadro clínico compatible. Como isquémica o necrótica si existeron hallazgos indicativos de necrosis o isquemia miocárdica como alteración de la motilidad parietal o del engrosamiento sistólico de los segmentos relacionados a la inserción de los músculos ]]>
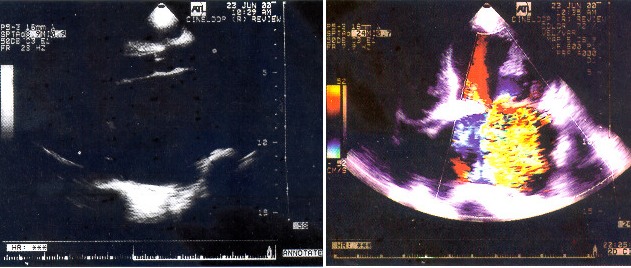
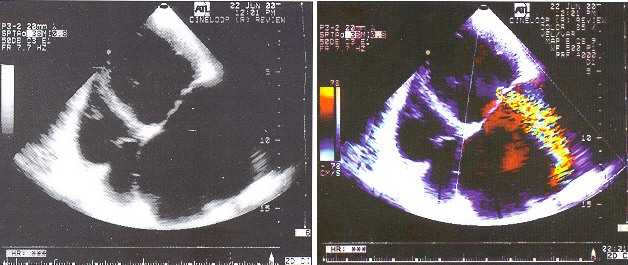
Sesenta y dos casos presentaron insuficiencia mitral leve a moderada (76.7%) y 18 severa (21.9%). De estos 18 pacientes, la mayoría (77%) corresponden a causa reumática o mixoide en igual proporción (9 de cada grupo), ( figuras 2 y 3 ).
]]>
Sesenta y un pacientes presentaban función sistólica ventricular izquierda normal (75.6%) y 21 con algún grado de deterioro.
Discusión
]]>
El hallazgo más notable y esperable de esta serie es la mayor prevalencia de causa reumática y mixoide, a diferencia de lo que se reporta en series norteamericanas y en otros países industrializados. En un estudio patológico publicado por Waller (1 ) y colaboradores la causa principal de insuficiencia mitral en los Estados Unidos en un alto porcentaje (66% de los casos) fue el prolapso de válvula mitral por degeneración mixoide. Un 27% fue por cardiopatía isquémica un 5 % por endocarditis y solamente un 1 % de los casos de ellos fueron atribuibles a enfermedad reumática.
]]>
Esto denota que la fiebre reumática sigue ocupando un lugar importante como causa productora de valvulopatía mitral en nuestro país, por lo que la experiencia adquirida en este tipo de afección valvular es amplia y variada. Es sabido que la prevalencia de fiebre reumática es paralela a las condiciones socioeconómicas, de manera que en los países no industrializados, las clases sociales de menos recursos son las que generalmente se ven más afectadas ]]>
7 ,8 ). Cabe anotar que también en el subgrupo con disfunción valvular severa, se mantuvo similar proporción ]]>
La enfermedad arterial coronaria que causa isquemia o lesión de los músculos papilares es una causa común en la actualidad debido a su alta prevalencia en países desarrolados (9 ,10 ). Aunque también lo es en nuestros países latinoamericanos, de igual forma es muy prevalente aún la fiebre reumática, ]]>
Respecto a los datos obtenidos, es de notar la mayor proporción de mujeres, hallazgo más frecuente en estenosis mitral. Y con respecto a la edad, aunque algunos pacientes son muy jóvenes, el promedio de edad (51 años) es indicativo de la evolución lenta de esta valvulopatía por sobrecarga de volumen, a diferencia de las por sobrecarga de presión de causa reumática en que habitualmente se espera un inicio de síntomas más temprano.
]]>
El hallazgo de función ventricular preservada en la mayoría de los pacientes también refleja la evolución relativamente lenta y benigna de esta condición, pero es bien conocida también la controversia respecto al momento quirúrgico en pacientes asintomáticos dada la posibilidad de progresión y síntomas incapacitantes (8 ).
]]>
Los hallazgos obtenidos son extrapolables al país, ya que se trata de un centro de referencia cuya área de atracción abarca alrededor del 40% del territorio nacional.
]]>
Conclusión
En esta serie se encontró prevalencia similar de la causa reumática y el prolapso de la valvula mitral mixoide, las más frecuentes de insuficiencia mitral pura. La isquémica ocupó el tercer lugar. La mayoría de los casos fueron leves a moderadas y de los casos con insuficiencia mitral severa, se dió la misma proporción.
]]>
Figura 2. Un caso de insuficiencia mitral severa por valvulopatía reumática. En el recuadro izquierdo, eje largo paraesternal, se obser dilatación severa del atrio izquierdo. En el derecho, el mapeo con doppler color demuestra un flujo retrógrado hacia el atrio izquierdo indicativo de disfunción valvular grave.
]]>
Figura 3. Insuficiencia mitral por degeneración mixoide de la válvula mitral. En el recuadro izquierdo, vista de cuatro cámaras, dilatación severa del atrio izquierdo comprimiendo al derecho, se observa una válvula mitral redundante y engrosada. En el derecho, el mapeo con doppler color permite estimar la regurgitación como severa.
Referencias
1- Waller BF, Howard J, fess S. Pathology of mitral valve stenosis and pure mitral valve regurgitation:Part II. Clin Cardiol 1994;17(7):395-402
2- Kalangos A, Beghetti M, Vala D,et al Anterior mitral leaflet prolapse as a primary cause of pure rheumatic mitral insufficiency. Ann Thorac Surg 2000;69(3):755-61
5.- Penther P, Boschat J, Etienne Y, Jobic Y. Current anatomical and etiological aspects of chronic or subacute, surgical, pure mitral valve insufficiency in adults. Apropos of 75 medicosurgical cases. Ann Cardiol Angeiol (Paris) 1991 Apr;40(4):181-5
6- Roberts WC Morphologic features of the normal and abnormal mitral valve. Am J Cardiol 1983 Mar 15;51(6):1005-28
7- Falco A, Sante P, Renzulli A, et al. Etiology and incidence of pure mitral insufficiency: a morphological study of 926 native valves. Cardiologia 1990 Apr;35(4):327-30
8- Delaye J, Beaune J, Gayet JL, Fatayri W, Silvestre A. Current etiology of organic mitral insufficiency in adults. Arch Mal Coeur Vaiss 1983 Sep;76(9):1072-6
9- Pizzarello RA, Turnier J, Goldman MA, Dworkin P, Oka M, Tortolani AJ, Padmanabhan VT. Clinical and echocardiographic features of isolated severe pure mitral regurgitation. Clin Cardiol 1984 Nov;7(11):565-71
10- Di Chiara A, Plewka M, Fioretti PM. Systolic anterior movement of mitral valve during acute apical myocardial infarction: An unusual mechanism of acute mitral regurgitation. J Am Soc Echocardiogr 1999;12(12):1117-21