Introducción
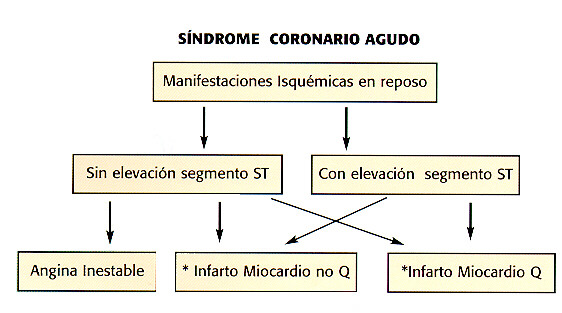
La angina inestable, el infarto del miocardio con o sin onda Q constituyen el denominado Síndrome Coronario Agudo (SCA).Estas entidades tienen una relación fisiopatológica común y representan estadíos diferentes de fisura, ruptura y formación de un trombo en la placa aterosclerótica (1,2). De no tratarse agresivamente la angina inestable progresa hacia la muerte en el 5 a 10% de los pacientes y al infarto no mortal en el 10 a 20%, ocurriendo estos eventos en los primeros días a semanas del inicio de los síntomas (12).
Una vez iniciado el proceso la manifestación clínica dependerá de: ]]>
1. La rapidez de la oclusión.
Son muy útiles en pacientes que presentan dolor isquémico y sin cambios importantes del electrocardiograma. Permiten obtener un diagnóstico, dan información sobre pronóstico y ayudan a seleccionar el tratamiento adecuado (35).
La Creatin-fosfokinasa y la fracción MB han sido los marcadores más utilizados en el SCA hasta hace unos pocos años. Presentan algunas limitaciones, sobre todo que se encuentran niveles bajos de CK-MB en personas sanas y también pueden estar elevados cuando hay daño severo al músculo esquelético. Existe en una forma CK-MB 2 en el tejido cardíaco y es convertida por una lisina-carboxipeptidasa a CK-MB1 cuando es liberada al suero. Cuando esto ocurre rápidamente la conversión de CK-MB 2 no se realiza inmediatamente por lo que la relación CK-MB 2 / CK-MB1 se eleva. Una relación de CK-MB 2 a CK-MB 1 mayor de 1.5 y una CK-MB 2 mayor de 1 U/lt es indicativo de una necrosis en evolución (36,37,38).
Mioglobina. Es una proteína de bajo peso molecular presente en el músculo esquelético y cardíaco, muy sensible para detectar daño miocárdico pero poco específica. Es rápidamente liberada del miocardio necrótico y rápidamente eliminada por los riñones. Niveles elevados de mioglobina se detectan también en pacientes con angina inestable (39).
Troponinas: han sido estudiadas extensamente y fueron aprobadas para uso clínico por la Food and Drug Administration en 1994. Las troponinas cardíacas se encuentran ausentes en el plasma de personas sanas, es por esta razón que aún pequeñas elevaciones indican necrosis miocárdica. En el documento en conjunto de la Sociedad Europea de Cardiología y el Colegio Americano del Corazón (40) han recomendado que la elevación de la troponina sea parte de la definición del IAM. Es muy claro en la actualidad que cualquier nivel de daño miocárdico, detectado por elevación de las troponinas implica un factor evolutivo de mal pronóstico. Esta condición no sólo es cierta para los eventos espontáneos sino también para aquellos que ocurren en las intervenciones de revascularización. En la actualidad no existe un umbral en la elevación de las troponinas que se pueda considerar seguro. De tal manera que toda necrosis miocárdica que se detecte por elevación de las troponinas debe ser considerada un infarto del miocardio (40). Por lo tanto pacientes que se presentaban con un SCA que eran CK-MB negativo pero troponina positivo eran considerados angina inestable, con la nueva definición se consideran IM no Q. Los pacientes que se presenten con dolor isquémico típico deben ser clasificados como portadores del SCA ya sea con o sin elevación del segmento ST y luego reclasificados horas más tarde en pacientes con troponina y CK-MB positiva o negativa (41,42,43).
Establecer tempranamente si hay evidencia de daño miocárdico en los SCA sin elevación del ST es muy importante ya que son pacientes que en la mayoría presentan enfermedad coronaria severa, lesiones complejas y trombosis visible en la angiografía coronaria (44).
Los estudios PRISM (46),CAPTURE (47),EPIC (48), y FRISC-I (49) mostraron que pacientes con el SCA sin elevación del ST con aumento de la troponina se benefician con el tratamiento con los inhibidores de la glicoproteina IIb/IIIa y/o con el uso de Heparinas de Bajo Peso Molecular (50). Este efecto del tratamiento dirigido a controlar la agregación plaquetaria y la formación de trombina en los pacientes que presentan elevación de troponinas corrobora la hipótesis de que la embolización de micro trombos es la explicación de la elevación de la troponina en los SCA sin elevación del ST (51). Sin embargo el estudio GUSTO-IV ACS presentado en Amsterdam recientemente en la reunión de la Sociedad Europea de Cardiología evaluando el tratamiento con Abciximab asociado a heparina y aspirina en pacientes estratificados por medio de troponina sorprendentemente no mostró beneficio de este esquema terapéutico. El 60% de los pacientes tenían troponinas alteradas y la mortalidad a los treinta días fue de sólo 8% en el grupo placebo y el grupo tratado con Abciximab no mostró ningún beneficio adicional. Por estas razones es que en la actualidad para algunos autores no es conveniente recomendar el uso rutinario de los bloqueadores de la glicoproteina IIb/IIIa en los SCA solamente por el aumento de las troponinas cardíacas.
Los pacientes de bajo riesgo con SCA y troponina normal son un grupo con una incidencia muy baja de eventos cardíacos futuros (54). No ocurre así con la evolución de pacientes de riesgo intermedio con troponina negativa que pueden desarrollar poste-riormente complicaciones cardíacas.
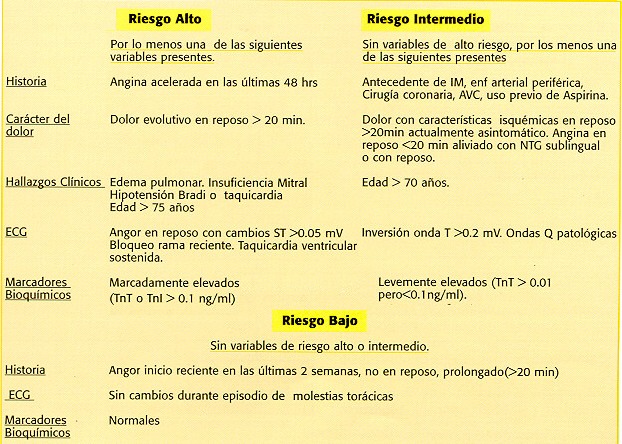
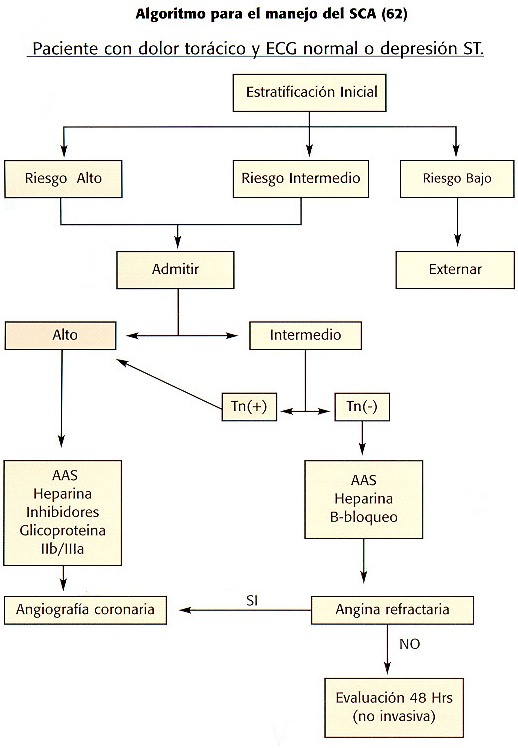
Grupos de bajo, intermedio y de alto riesgo pueden ser identificados usando las variables clínicas, electrocardiográficas obtenidas en admisión y con un período de observación de 6 a 12 horas durante el cual se analizará la presencia de daño miocárdico. Pacientes de bajo riesgo que no tienen evidencia de necrosis miocárdica y que no mostraron complicaciones en el período de observación pueden ser externados y controlados posteriormente. Por el contrario pacientes de riesgo intermedio o alto deben ser admitidos a pesar de que no exista evidencia de daño celular (41,55,56).
]]>
Diferentes grupos entre ellos el Dr Maseri han demostrado que los pacientes con angina inestable y con infarto del miocardio sin elevación del ST que presentan elevaciones de marcadores de inflamación como son la proteína C reactiva, fibrinógeno, una proteína en suero parecida al amiloide A, y la interleukina 1 y 6 por lo general tienen una mayor incidencia de complicaciones cardiovasculares que los pacientes con marcadores normales (57,58,59,60,85,86.).
Estudio muy útil para obtener información sobre función sistólica y alteraciones de la contractilidad segmentaria. Debe recordarse que se requiere una lesión que comprometa más del 20% del grosor de la pared miocárdica para que se detecte una alteración de la contractilidad segmentaria por Ecocardiografía. Esta técnica no distingue isquemia de infarto, ni lesiones recientes de antiguas.
Estratificación de riesgo.
La historia clínica, el examen físico, el electrocardiograma y los marcadores de daño miocárdico pueden ser integrados para valorar el riesgo de infarto o muerte en pacientes que se presentan con el SCA (61).
El manejo del SCA se ha vuelto multifactorial debido a quela terapia va dirigida a los diferentes estadíos fisiopatológicos que desencadenan este Síndrome, desde la activación de la placa, la isquemia hasta la necrosis celular. En los pacientes que presentan IM con elevación del ST, la restauración del flujo al miocardio con la disolución del trombo por medio de la trombolísis es de suma importancia. En los pacientes con angina inestable o IM sin elevación ST la estabilización de la placa para prevenir la progresión de la enfermedad, la recurrencia de la trombosis y de la vasoconstricción son mandatorias. (63).
A. Medidas Generales:
1. Reposo
1.Aspirina. Excelente medicamento en el tratamiento de los SCA. Debe utilizarse de inmediato ante cualquier manifestación de enfermedad coronaria y continuarse por tiempo indefinido en pacientes que no presenten contraindicaciones. Numerosos estudios han demostrado su utilidad en la angina inestable y el IM no Q, con una reducción mayor del 50% en el riesgo de muerte o de IM (73-74). En el estudio ISIS-2 redujo la mortalidad por más del 25% y la posibilidad de re- infarto en más del 40% (75).
Actúa inhibiendo irreversiblemente la ciclo oxigenasa 1 de las plaquetas, previene la formación de tromboxano A2, disminuyendo la agregación plaquetaria por esta vía (84).
2.Ticlopidina y Clopidogrel. Son dos antagonistas del Difosfato de Adenosina aprobados para uso como terapia antiplaquetaria (80). Se utilizan en pacientes que no pueden usar aspirina ya sea por alergia o por intolerancia gástrica. El estudio CAPRIE (76) comparó el uso de aspirina versus clopidogrel en pacientes con riesgo de eventos isquémicos. Este último demostró ser igual o levemente superior a la aspirina, pero con una incidencia un poco mayor de efectos adversos.
D. Terapia Anticoagulante:
1.Heparina. Ejerce su efecto anticoagulante acelerando la acción de la antitrombina circulante, una enzima proteolítica que inactiva el Factor IIa (trombina), el Factor IXa y el Factor Xa. Previene la propagación pero no lisa al trombo ya establecido. El Dr Oler (77) en un meta-análisis de la literatura mostró una reducción del 33% en muerte o en IM en pacientes tratados con heparina y aspirina versus la aspirina sola, éste estudio y otros (78) soportan el uso de la combinación de la terapia antiplaquetaria y anticoagulante en los SCA.
Un gran avance en el tratamiento anticoagulante ha sido el desarrollo de las Heparinas de Bajo Peso Molecular que son una combinación de inhibidores de la Trombina y el Factor Xa. Tienen un peso molecular de 400 a 500 Da en comparación con la Heparina no Fraccionada que es de 12.000 a 15.000. Presentan ciertas ventajas sobre la heparina estándar que las han hecho más populares. Inhiben al Factor Xa y bloquean la actividad y generación de la trombina. Inducen una mayor liberación del inhibidor de la vía del Factor Tisular y no es neutralizada por el Factor Plaquetario 4 (79). No aumenta la permeabilidad capilar (lo cual lleva a tener menos complicaciones de sangrado) y tiene menor incidencia de trombocitopenia. Además de la facilidad de la administración subcutánea y el no tener que realizar monitoreos de anticoagulación. Hay evidencia convincente que las Heparinas de Bajo Peso Molecular son más efectivas que placebo y por lo menos tan efectivas como la Heparina no Fraccionada en reducir la muerte y el infarto recurrente en pacientes con angor inestable o con IM no Q. Entre estos están el estudio ESSENCE(81) y TIMI-IIB (82) y el meta análisis de ambos (83) que demostraron una mayor eficacia de la Enoxaparina sobre la Heparina no Fraccionada.
2. Antagonistas de los receptores de la Glicoproteína IIb/IIIa. Los receptores GP IIb/IIIa son específicos de las plaquetas y codificados por diferentes genes en el brazo largo del cromosoma 17. Cada plaqueta tiene de 50.000 a 80.000 receptores. Estos son muy importantes porque es la vía final común en la agregación plaquetaria que lleva a la formación del trombo (87,88).
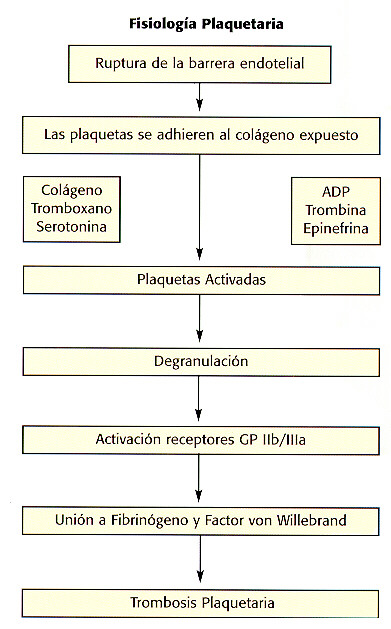
La identificación de estos receptores ha llevado al desarrollo de bloqueadores específicos. Estos actúan ocupando un sitio en los receptores con lo cual previenen la unión al fibrinógeno y evitan la agregación plaquetaria. ]]>
Clasificación de los Inhibidores de la GP IIb/IIIa| Forma | Inhibidor | |
| 1. Anticuerpo Monoclonal | Abciximab | |
| 2. Antagonista Natural GP IIb/IIIa | Veneno serpiente | |
| 3. Antagonista Sintético GPIIb/IIIa | ||
| Eptifibatide Tirofiban | |
Contrariamente a lo que ocurre con la terapia IV, la vía oral no ha demostrado ningún beneficio tal y como como se reporta en los estudios con Sibrafiban, Xemilofiban y Orbofiban (99,100).
Contraindicaciones:
1. Plaquetopenia < 100.000.
Ejercicio regulado, disminución de peso, manejo adecuado del estrés.
Fumado. Suspenderlo a través de programas especiales y educación. ]]>
Genética, de gran interés para el futuro (118).Hipertensión bien controlada, preferiblemente con inhibidores de ECA.
Artículo interesante (119) Deben ser los Inhibidores de ECA terapia estándar en los pacientes con enfermedad aterosclerótica. J Am Coll Cardiol 2001;37:1-8.
1.Fuster V,Badimon L,Badimon J J,Chesebro J H. The pathogenesis of coronary artery disease and the acute coronary syndromes ( Part I ).N Engl J Med 1992; 326: 242-50. [ Links ]
2.Fuster V, Badimon L, Badimon J J, Chesebro J H. The pathogenesis of coronary artery disease and the acute coronary syndromes ( Part II ) N Engl J Med 1992;326:310-318. [ Links ]
3.Fuster V,Badimon L, Cohen M,Ambrose JA.et al. Insights into the pathogenesis of acute ischemic syndromes. Circulation 1988;77:1213-20. [ Links ]
4.Dalager - Pederson S,Morre Pederson E,Ringgaard S,Falk E. Coronary Artery Disease: Plaque Vulnerability,Disruption and Thrombosis.From Fuster V. The Vulnerable Atherosclerotic Plaque.American Heart Association.Monograph Series.1999:1-23. [ Links ]
5.Dlavies M J, Thhomas A C. Plaque fissuring the cause of acute myocardial infarction,sudden ischemic death, and crescendo angina. Br Heart J 1985;53:363-73. [ Links ]
6.Plutzky J. Atherosclerotic Plaque rupture: emerging insights and opportunities. Am J Cardiol 1999;84:15J-20J. [ Links ]
7.Libby P. Molecular bases of the Acute Coronary Syndromes.Circulation 1995;91:2844-50. [ Links ]
8.Moreno P R,Falk E,Palacios JF,Neewell JB,Fuster V,FallonJ.Macrophage infiltration in Acute Coronary Syndromes: implications for plaque rupture.Circulation 1994;90:775-8. [ Links ]
9.Hamm CW,Lorenz RL,Bleifeld W,Kupper W et al.Biochemical evidence of platelet activation in patients with persistent unstable angina.J Am Coll Cardiol 1987;10:998-1004. [ Links ]
10.Falk E, Shah PK,and Fuster V.Coronary Plaque Disruption.Circulation 1995;92:657. [ Links ]
11.DeWood MA, Stiffer WF, Simpson CS,et al.Coronary angiografic findings soon after non Q wave myocardial infarction.N Engl J Med1986;315:417-23. [ Links ]
12.Cannon C.Curr Probl Cardiol.1999;24:683-744. [ Links ]
13.Falk E.Unstable Angina with fatal outcome:dynamic coronary thrombosis leading to infarction and/or sudden death.Circulation 1985;71:699-708. [ Links ]
14.Sullivan E,Kearney M ,Isner J,Topol E,Losordo D.Pathology of unstable angina:analysis of biopsies obtained by directional coronary atherectomy. J Throm Thrombolysis.1994;I:63-71. [ Links ]
15.Sherman CT,Litvack F,Grundfest W,LeeM et al. Coronary angioscopy in patients with unstable angina pectoris. N Engl J Med 1986;315:913-9. [ Links ]
16.MizunoK,Satumo K,Miyamoto A, Arakawa E,et al.Angioscopic evaluation of coronary artery thrombi in acute coronary syndromes. N Engl J Med 1992;326:287-91. [ Links ]
17.The TIMI III A investigators. Early effects of tissue-type plasminogen activator added to conventional therapy on the culprit lesion in patients presenting with ischemic cardiac pain at rest. Results of the Thrombolysis in Myocardial Ischemia (TIMI IIIA) trial.Circulation 1993;87:38- [ Links ]
18.AmbroseJA,HjemdaMosenCE,BorricoS,GorlinR,FusterV.Angiographic demostration of a common link between unstable angina and non Q wave myocardial infarction Am J Cardiol 1988;61:244-7. [ Links ]
19.Fitsgerald DJ,RoyL,Catella F, Fitzgerald GA.Platelet activation in unstable coronary disease.N Engl J Med 1986;315:983-9. [ Links ]
20.Alexopoloulos D,Ambrose JA, Stump D,Borrico S et al.Thrombosis related markers in unstable angina. J AmColl Cardiol 1991;17:866-71. [ Links ]
21.Oler A,Whooley MA,Oler J,Grady D.Adding heparin to aspirin reduces the incidence of myocardial infarction and death in patients with unstable angina.A Meta Analysis.JAMA 1996;276:811-5. [ Links ]
22.A definition of advanced type of atherosclerotic lesions and a histological classification of atherosclerosis: a report from the Committee on Vascular Lesions of the Council on Atherosclerosis,American Heart Association.Circulation 1995;92:1355-1374.
23.Braunwald E:Unstable Angina:A classification Circulation1989;80:410-4 [ Links ]
24.Ahmed WH,Bittl JA ,Braunwald E.Relation between clinical presentation and angiographic findings in unstable angina pectoris,and comparison with that in stable angina. Am J Cardiol 1993;72:544-550. [ Links ]
25.Danges G,Mehran R,Wallenstein S et al.Correlation of angiographic morphology and clinical presentation in unstable angina. J Am Coll Cardiol 1997;29:519-525. [ Links ]
26.DeServiS,ArbustiniE,Marsica F et al.Correlation of angiographic morphology findings in unstable angina.Am J Cardiol 1996;77:128-132. [ Links ]
27.Owa M,OrigasaH,Saito M.Predictive validity of the Braunwald classification of unstable angina for angiographic finding,short-term prognosis,and treatment selection.Angiology.1997;48:663-670. [ Links ]
28.Lee T,Cook E,Weisberg M,Sargent RK et al,Acute chest pain in the Emergency Room:identification and examination of low-risk patients. Arch Intern Med 1985;145:65-9. [ Links ]
29.TIMI IIIB Investigators.Effects of tissue plasminogen activator and a comparison of early invasive and conservative strategies in unstable angina and non Q wave myocardial infarction.Circulation1994;89:1545-1556. [ Links ]
30.Cannon CP,McCabe CH,StoneP,et al.The electrocardiogram predicts one year outcome of patients with unstable angina and non Q wave myocardial infarction:results of the TIMI III Registry ECG Ancillary Study.J Am Coll Cardiol.1997;30:133-140. [ Links ]
31.RouanGW,LeeT,CookE,BrandDA,lWeisbergM,GoldmanL.Clinical characteristics and outcome of acute myocardial infarction in patients with initially normal or nonspecific electrocardiograms ( a report from the Multicenter Chest Pain Study ).Am J Cardiol 1989;64:1087-92. [ Links ]
32.Slater DK, Hlatky M A,Mark DB,Harrell FE,et al.Outcome in suspected acute myocardial infarction with normal or minimally abnormal admission electrocardiographic findings.Am J Cardiol 1987;60:766-70. [ Links ]
33.Patel DJ,Knight CJ,Holdright DR et al. Long term prognosis in unstable angina: the importance of early risk stratification using continuous ST segment monitoring.Eur Heart J 1998;19:240-9. [ Links ]
34.Gottlieb SO,Weisfeldt M L,Ouyang P,et al.Silent ischemia as a marker for early unfavorable outcomes in patients with unstable angina.N Engl J Med 1986;314:1214-11219. [ Links ]
35.Roberts R,Fromm RE.Management of acute coronary sindromes based on risk stratification by biochemical markers: an idea whose time has come.Circulation 1998;98:1831-3. [ Links ]
36.Puleo PR,Meyer D,Wathen C,et al.Use of a rapid assay of subforms of creatine-kinase-MB to diagnose or rule out acute myocardial infarction.N Engl J Med 1994;331:561-6 [ Links ]
37.Newby LK,Gibler WB,Ohman WM,et al.Biochemical markers in suspected Acute Myocardial Infarction.Clin Chem 1995;41:1263. [ Links ]
38.Puleo PR,Guadagno PA, Roberts R,Scheel MV,et al.Early diagnosis of acute myocardial infarction based on assay for subforms of creatine kinase-MB.Circulation.1990;82:759-64. [ Links ]
39.Adams JE,Abendschein DR,Jaffe AS.Biochemical markers of myocardial injury.Is MB creatinine kinase the choice for the 1990.Circulation 1993;88:750-63. [ Links ]
40.Antman E,Bassand JP,KleinW,et al. Myocardial Infarction Redefined.A consensus document of the Joint European Society of Cardiology/American College of Cardiology committee for the redefinition of Myocardial Infarction.J Am Coll Cardiol 2000;36:959-69. [ Links ]
41.de Winter R.Risk Stratification with Cardiac Troponin I in Acute Coronary Syndromes.J Am Coll Cardiol 2000;36:1824-6. [ Links ]
42.Hamm CW,Ravkilde J,Gerhardt W,et al.The prognostic value of serum Troponin T in Unstable Angina.N Engl J Med 1994;327:146-50. [ Links ]
43.Ohman EM,Armstrong PW,Christenson RH,et al.Cardiac Troponin T levels for risk stratification in acute myocardial ischemiaGUSTO II A Investigators N Engl J Med 1996;335:1333-41. [ Links ]
44.Heeschen C,vandenBrand MJ,Hamm CW, Simoons ML. Angiographic findings in patients with refractory unstable angina according to Troponin T status.Circulation 1999;100:1509-14. [ Links ]
45.Hanam CH,Braunwald E. A Classification of Unstable Angina Revisited.Circulation 2000;102:118-122. [ Links ]
46.Heeschen C,Hamm CW,Goldman B,Deu A et al.Troponin concentrations for stratification of patients with Acute Coronary Syndromes in relation to therapeutic efficacy of Tirofiban. PRISM Study Investigators. Platelet Receptor Inhibition in Ischemic Syndrome Management.Lancet 1999;354:1757-62. [ Links ]
47.The CAPTURE Investigators:Randomized placebo controlled trial of Abciximab before and during coronary intervention in refractory unstable angina: the Capture Study.Lancet 1997;349:1429-1435. [ Links ]
48.The EPIC Investigators:Use of a monoclonal antibody directed against the platelet Glycoprotein IIb/IIIa receptor in high-risk coronary angioplasty.N Engl J Med 1994;330:956-961. [ Links ]
49.Lindahl B,Venge P,Wallentin L.The FRISC experience with Troponin T.Use as decision tool and comparison with other prognostic markers.Eur Heart J 1998;19Suppl N:W51-N58. [ Links ]
50.Boersma E,Akkerhuis KM,Theroux P,Califf RM,Topol EJ.Platelet glycoprotein IIb/IIIa receptor inhibition in non-ST elevation Acute Coronary Syndromes:early benefit during medical treatment only,with additional protection during percutaneous coronary intervention. Circulation 1999;100:2045-8. [ Links ]
51.Hamm CW. Unstable Angina: the breaktrough (editorial).Eur Heart J 1999;20:1517-9. [ Links ]
52.Wallentin L,Lagerquist B Husted S,Kontwy F,et al.Outcome at 1 year after an invasive compared with a non-invasive strategy in unstable coronary artery disease: the FRISC II invasive randomized trial.Frisc investigators. Fast Revascularization during instability in Coronary Artery Disease.Lancet 2000;356:9-16. [ Links ]
53.Bertrand ME, Smoons ML,Fox K,Wallentin L ,et al. Management of Acute Coronary Syndromes: Acute Coronary Syndromes without persistent ST segment elevation.Recommendations of the Task Force of the European Society of Cardiology. Eur Heart J 2000;21:1406-32. [ Links ]
54.Hamm CW,Goldman BU,HeeschenC,Kreyman G et al, Emergency Room triage of patients with acute chest pain by means of rapid testing for cardiac Troponin T or Troponin I.N Engl J Med 1997:337:1648-53. [ Links ]
55.Kontos M C, Anderson FP,Alimard R,Ornato JP,et al. Ability of Troponin I to predict cardiac events in patients admitted from the emergency department. J Am Coll Cardiol 2000;36:1818-23. [ Links ]
56.Johnson PA,Goldman L,Sacks D ,et al.Cardiac Troponin T as a marker for Myocardial Ischemia in patients seen at the Emergency Department for acute chest pain.Am Heart J 1999;137:1137-44. [ Links ]
57.Berck BC, Weintraub WS,Alexander RW. Elevation of C-Reactive protein in "Active coronary artery disease. Am J Cardiol 1990;65:168. [ Links ]
58.Liuzzo G,Biasucci LM,Gallimorre JR,et al.The prognostic value of C-reactive protein in severe angina. N Engl J Med 1994;331:407. [ Links ]
59.Biasucci LM,LiuzzoGkFantuzzi G et al.Increasing levels of interleukinIL-1Ra and Il-6 during the first 2 days of hospitalization in Unstable Angina are associated with increased risk of in hospital coronary events. Circulation 1999;99:2079. [ Links ]
60.Morrow DA,Rifai N,Antman EM,et al. Serum Amyloid A predicts early mortality in acute coronary syndromes: a TIMI II A substudy. J Am Coll Cardiol 2000;35:358-62. [ Links ]
61.Unstable Angina: Diagnosis and Management.May 1994. Braunwald E,MarkD,Jones R et al Unstable Angina: diagnosis and management.Rockville MD.Agency for Health Care Policy and Research and the National Heart,Lung,and Blood Institute. [ Links ]
62.Braunwald E,Joones RH,Mark D,et al.Diagnosis and managing Unstable Angina.Circulation 1994;90:613-22. [ Links ]
63.Braunwald E,Antman E, Beasley JW,et al. ACC/AHA guidelines for the management of patients with Unstable Angina and non-ST segment elevation MI: executive sumary and recommendations: A report of the American Collegue of Cardiology/American Heart Association Task Force on Practice Guideliness. J Am Coll Cardiol 2000;36:970-1062. [ Links ]
64.Gibbons R, Chatterje K,Daley J,et al.ACC/AHA/ACP-ASIM guidelines for the management of patients with Chronic Stable Angina . J Am Coll Cardiol 1999;33:2097-197. [ Links ]
65.Cheitlin MD,Hutter A,Brindis R,et al.ACC/AHA expert consensus document: use of Sildenafil(Viagra) in patients with cardiovascular disease:American College of Cardiology/American Heart Association. J Am Coll Cardiol 1999;33:273-82. [ Links ]
66.YusufS , Wittes J,Friedman L. Overview of results of randomized clinical trials in heart diseaseII.Unstable Angina, Heart Failure, primary prevention with aspirin,and risk factor modification.JAMA1988;260:2259-63. [ Links ]
67.Gheorghiade M,Schultz L,Tilley B,et al.Effects of Propanolol in non-Q wave acute Myocardial Infarction in the Beta Blocker Heart Attack Trial. Am J Cardiol 1990;66:129-33. [ Links ]
68.Gibson R,Boden WE, Theroux P, Strauss H, et al.Diltiazem and reinfarction in patients with non -Q wave myocardial infarction.Results of a double-blind,randomized,multicenter trial. N Engl J Med 1986;315:423-9. [ Links ]
69.The Multicenter Diltiazem Post infarction Trial Research Group. The effect of diltiazem on mortality and reinfarction after myocardial infarction.N Engl J Med 1988;319:385-92. [ Links ]
70.The Danish Study Group on Verapamil in Myocardial Infarction.Verapamil in acute myocardial infarction. Eur Heart J 1984;5:516-28. [ Links ]
71.Yusuf S,Sleight P, Pogue J, Bosch J,Davies R, Dagenais G Effects of an angiotensin-converting enzime inhibitor,ramipril,on cardiovascular events in high risk patients. The Heart Outcomes prevention Evaluation Study Investigators. N Engl J Med 2000;342:145-53. [ Links ]
72.ISIS-4.Collaborative Group.ISIS-4:randomized factorial trial assessing early oral captopril,oral monitrate, and intravenous magnesium sulphate in 58050 patients with suspected acute myocardial infarction.Lancet 1995;345:669-85. [ Links ]
73.Lewis HD, Davis JW, Archibald D,lSteinke W,et al. Protective effects of aspirin against acute myocardial infarction and death in men with unstable angina.N Engl J Med 1983;309:396-403. [ Links ]
74.Cohen M,Xiong J ,Parry G,et al.Prospective comparison of unstable angina versus non-Q wave myocardial infarction during anti thrombotic therapy.J Am Coll Cardiol 1993;22:1338-44. [ Links ]
75.ISIS-2 (Second International Study of Infarct Survival ) Collaborative Group.Randomized trial of intravenous streptokinase,oral aspirin,both or neither among 17187 cases of suspected acute myocardial infarction:ISIS-2.Lancet 1988;2:349-60. [ Links ]
76.CAPRIE Steering Committee. A randomized,blinded,trial of Clopidogrel versus Aspirin in patients at Risk of Ischaemic Events (CAPRIE) Lancet 1996;348:1329-39. [ Links ]
77.Oler A,Whooley MA,Oler J ,et al.Meta-Analisis of the benefit of heparin plus aspirin compared with aspirin alone in unstable angina/ non-ST elevation MI. JAMA 1996;276:811-5. [ Links ]
78.Holdrigh D,PatelD,Cunningham D,et al.Comparison of the effect of heparin and aspirin versus aspirin alone on transient myocardial ischemia and in hospital prognosis in patients with unstable angina. J Am Coll Cardiol 1994;24:39-45. [ Links ]
79.Hirsh J,Fuster V.Guide to anticoagulation therapy. Part I: Heparin. Circulation 1994;89:1449-68. [ Links ]
80.Quinn M, Fitzgeral D. Ticlopidine and Clopidogrel. Circulation.1999;100:1667-1672. [ Links ]
81.Cohen M,Dermers C,Gurfinkel EP,et al.For the Efficacy and Safety of Subcutaneous Enoxaparin in Non -Q-Wave Coronary Events Study Group.A comparison of low molecular weight heparin with unfractionated heparin for ustable coronary artery disease. N Engl J Med 1997;100:1593-601. [ Links ]
82.Antman EM,Mcabe CH,Gurfinkel EP,et al.Enoxaparin prevents death and cardiac ischemic events in unstable angina/non Q wave myocardial infarction:results of the Thrombolysis in Myocardial Infarction (TIMI)IIB.Circulation 1999;100:1593-601. [ Links ]
83.Antman E M,Cohen M,Radley D ,et al.Assessment of the treatment effect of Enoxaparin for Unstable angina/Non Q wave Myocardial Infarction. TIMI-IIB-ESSENCE meta-analysis. Circulation 1999;100:1602-8. [ Links ]
84.Awtry E,Loscalzo J.Aspirin.Circulation 2000;101:1206-1218. [ Links ]
85.Shah P.Circulatin Markers of Inflammation for Vascular Risks Prediction.Circulation 2000;101:1758-1759. [ Links ]
86.Liuzzo G,Biasucci L,Gallimore R ,et al.Enhaced Inflamatory Response in Patients with Preinfarction Unstable Angina. J Am Coll Cardiol 1999:34:1696-703. [ Links ]
87.Lefkovits J,Plow EF, Topol EJ. Platelet glycoprotein II b/IIIa receptores in cardiovascular medicine. N Engl J Med 1995;332:1553-9. [ Links ]
88.Coller B S. Blockade of platelet GP IIb/IIIa receptors as an antithrombotic strategy. Circulation 1995.92:2372-8. [ Links ]
89.The EPIC investigators. Use of a monoclonal antibody directed against the platelet glycoprotein IIb/IIIa receptor in high-risk coronary angioplasty: the EPIC Investigation. N Engl J Med 1994;330:956-61. [ Links ]
90.The EPILOG Investigators. Platelet Glycoprotein IIb/IIIa receptor blockade and low-dose heparin during percutaneous coronary revascularization: the Epilog Investigators. N Engl J Med 1997;336:1689-96. [ Links ]
91.Lincoff AM,Califf RM,Moliterno DJ,et al.Coomplementary clinical benefits of coronary artery stenting and blockade of platelet glycoprotein IIb/IIIa receptors. Evaluation of Platelet IIb/IIIa Inhibition in Stenting Investigators N Engl J Med 1999;341:319-27. [ Links ]
92. The PURSUIT Trial Investigators: Inhibition of Platelet Glycoprotein IIb/IIIa with Eptibatide in patients with acute coronary syndromes. N Engl J Med 1998;339:436-443. [ Links ]
93.The Platelet Receptor Inhibition in Ischemic Syndrome Management( PRISM)Study Investigators. A comparison of Aspirin plus Tirofiban with Aspirin plus Heparin for Unstable Angina. N Engl J Med 1998;338:1498-1505. [ Links ]
94.The Platelet Receptor Inhibition in Ischemic Syndrome Management in patients limited by unstable signs and symptoms (PRISM-PLUS) Study Investigators. Inhibition of the platelet glycoprotein IIb/IIIa receptor with Tirofiban in unstable angina and non-Q wave myocardial infarction. N Engl J Med 1998;338:1488-1497. [ Links ]
95.The PARAGON Investigators: International, randomized, controlled trial of Lamifiban, Heparin or both in unstable angina. Circulation 1998;97:2386-2395. [ Links ]
96.Lincoff M, Califf R,Topol E. Platelet Glycoprotein IIb/IIIa receptor blockade in coronary artery disease. J Am Coll Cardiol 2000;35:1103-15. [ Links ]
97.Chew D, Moliterno D .A critical Appraisal of platelet Glycoprotein IIb/IIIa inhibition.J Am Coll Cardiol 2000;36:2028-35. [ Links ]
98.Scarborough R, Kleiman N, Phillips D. Platelet Glycoprotein IIb/IIIa antagonists.What are the Relevant Issues Concerning their Pharmacology and clinical use ? Circulation 1999:100:437-444. [ Links ]
99.Newby LK. A randomized comparison of Sibrafiban,an oral glycoprotein (GP)IIb /IIIa receptor antagonist,with and without aspirin versus aspirin after acute coronary syndromes (ACS): results of the second SYMPHONY Trial. J Am Coll Cardiol 2000;36:319-20. [ Links ]
100.Kereiakes DJ,Kleiman N,Ferguson JJ,et al. Pharmacodynamic efficacy, clinical safety and outcomes after prolonged glycoprotein IIb/IIIa, receptor blockade with oral Xemilofiban: results of a multicenter, placebo, controlled, randomized trial. Circulation 1998;98:1268-78. [ Links ]
101.Effects of tissue plasminogen activator and a comparison of early invasive and conservative strategies in unstable angina and non-Q-wave myocardial infarction: results of the TIMI III B trial.Thrombolysis in Myocardial Ischemia. Circulation 1994;89:1545-56. [ Links ]
102.Guidelines for coronary angiography: a report of the American College of Cardiology/American Heart Association Task Force on Assessement of Diagnostic and Therapeutic Cardiovascular Procedures. J Am Coll Cardiol 1987;10:935-50. [ Links ]
103.Ryan TJ, Amderson J L, Antman E M,et al.ACC/AHA guidelines for the management of patients with acute myocardial infarction: a report of the American College of Cardiology/ American Heart Association task force on practice guidelines(Committee on management of Acute Myocardial Infarction ). J Am Coll Cardiol 1996;28:1328-428. [ Links ]
104.Boden W E,Orourke R A,Crawford M H,Blaustein AS, Deedwania PC, Zoble RG,et al. Outcomes in patients with acute-non Q wave myocardial infarction randomly assigned to an invasive as compared with a conservative strategy. N Engl J Med 1998;338:1785-92. [ Links ]
105.Fragmin and Fast Revascularization during InStability in coronary artery disease Investigators. Invasive compared with non-invasive treatment in unstable coronary artery: FRISC II prospective randomized multicentre study. Lancet 1999;354:708-15. [ Links ]
106.Scull GS,Martin JS, Weaver WD, Every NR, for the MITI investigators. Early angiography versus conservative treatment in patients with non-ST- elevation acute myocardial infarction. J Am Coll Cardiol 2000;35:895-902. [ Links ]
107.The EPISTENT Investigators Randomized placebo- controlled and balloon-angioplasty controlled trial to assess safety of coronary stenting with use of platelet glycoprotein IIb/IIIa blockade. Lancet 1998;352:87-92. [ Links ]
108.Cannon CP,Weintraub WS, Demopoulos L Aa, Robertson DH Gormley GJ, Braunwald E for the TACTICS-TIMI 18 Investigators. Invasive versus Conservative strategies in unstable angina and non Q wave myocardial infarction following treatment with Tirofiban: rationale and study design of the international TACTIC-TIMI 18 trial. Am J Cardiol 1998;82:731-6. [ Links ]
109.Welty F. Optimal Management of Non-ST Segment Elevation Myocardial Infarction Remains Unclear . J Am Coll Cardiol 2000;35:903-906. [ Links ]
110.Andrews TC,Raby K,Barry J,et al. Effect of cholesterol reduction on Myocardial Ischemia in patients with coronary artery disease. Circulation 1997;95:324-8. [ Links ]
111.Aronow H,Wolski K, Lauer M. Marked reduction in mortality with early Lipid-Lowering after ST and non-ST elevation Acute Coronary Syndromes .[Abstract].Circulation 2000;102:II-435.
112.Hamm C, Heeschen C, Boehm M ,et al. Role of Statins in patients with Acute Coronary Syndromes.