Resumen
Presentamos aquí la experiencia quirúrgica en el tratamiento de la coartación aórtica acumulada a lo largo de 30 años en el Hospital México. Se intervinieron un total de 81 pacientes, cuyo promedio de edad es de 20.3 años, dado que inicialmente nuestro Centro contaba con un Servicio de Pediatría, existen 8 niños en la serie. Clínicamente los menores de un año se presentaron con insuficiencia cardíaca y los demás con sintomatología secundaria a hipertensión arterial o claudicación intermi tente. Durante los primeros 10 años se realizaron 27 resecciones y posteriormente se emplearon otras técnicas, pero a partir de 1984, se ha utilizado casi exclusivamente la aortoplastia con parche de duramadre.
Ochenta y cuatro por ciento del grupo se tornaron normotensos, 10% mejoraron y un 6% no cambiaron. Dieciseis por ciento tuvo morbilidad postoperatoria, presentando condiciones comunes a este tipo de intervención y que se resolvieron fácilmente.
]]> La aortoplastia con parche nos ha dado buenos resultados, es técnicamente sencilla puesto que se ejecuta en el plano frontal y se hace mejor hemostasia, permite el crecimiento de la aorta en los niños y al dejar un diámetro adecuado reduce sustancialmente el gradiente.Palabras Clave
Coartación de aorta, aortoplastía, parche de duramadre.
Summary
Eighty two patients with aortic coarctation have been operated upon at the Hospital Mexico during the last 30 years. The median age is 20.3 years and since at the beginning our center also cared for children, 8 of them are here included. The clinical presentation in those below 1 year was heart failure, and the rest manifested signs and symptoms related to arterial hypertension or distal ischemia such as intermittent claudication of the lower extremities. During the first 10 years 27 resections were performed and later on other techniques were adopted, but since 1984 dura mater patch aortoplasty has been exclusively employed.
Eighty four percent of the patients became normotensives, 10% improved and 6% did not change. Sixteen percent had common complications to this type of interventions which resolved with appropriate management. Two patients died (2.4%), one a 4 months old baby with heart failure and bronchopneumonia and the other a 23 year old with recoarctation who was reoperated for recurrent postoperative bleeding and developed multisystemic organ failure.
The patch aortoplasty technique has given us very good results, it is easy to perform since it is done right in front of the surgeon and better hemostasis can be achieved, the remaining aortic tissue can and it will grow and allows for a wider luminal diameter reducing or abolishing pressure gradients across the coarcted segment.
key Words
Aortic coarctation, aortoplasty, duramater patch. ]]>
Introducción
La coartación de la aorta es una malformación congénita que se presenta clínicamente por lo general a edades tempranas y que produce la muerte si no es tratada (4,14). Se ha reportado esporádicamente individuos de más de 70 años. (19) Representa de un 5 a un 10% de las patologías congénitas cardiovasculares y se observa en 1 de cada 4000 a 5000 necropsias (11,18 ) sigue siendo una patología de suma importancia debido a lo limitante del padecimiento para el enfermo(4,5,6,12). Cuadro clínico (4,6) 1. HTA que puede producir al paciente cefalea, visión borrosa, hemorragias retinianas (30), muerte súbita por ruptura de aneurismas intercostales (20) o de la aorta (12,13 ) y hemorragia subaracnoidea por ruptura de aneurismas del polígono de Willis (29). 2. Endarteritis y endocarditis bacteriana por anomalías valvulares asociadas (25). 3. Disminución de flujo arterial a miembros inferiores con la consecuente claudicación intermitente(4,10). Compromete en sus distintas variedades un estrechamiento del lumen de la aorta mayormente en situación periductal, pero que puede involucrar el área itsmica y en diferentes sitios del arco aórtico inclusive la aorta abdominal ( 27 ). Desde el punto de vista funcional tiene importancia la situación con respecto al ductus arterioso, reconociéndose una variedad preductal o del recién nacido, con un ductus permeable, una circulación del hemicuerpo superior arterial y del hemicuerpo inferior venosa que lleva a la insuficiencia cardíaca y muerte tempranamente relacionada a la permeabilidad del ductus (11,25), y una variedad postductal o del adulto, con los cambios tróficos, hipertensión arterial y una gran circulación colateral ( 4,6,25 ). Por lo general la coartación está en relación con el ductus arterioso, con una proliferación de tejido ductal proveniente del desarrollo del sexto arco aórtico que ocluye el lumen en forma de membrana incompleta por lo cual se ha denominado coartación yuxtaductal (11). El diagnóstico se reliza generalmente al exámen clínico del paciente con desarrollo del hemicuerpo superior y con hipotrofia del hemicuerpo inferior, en pacientes hipertensos con un gradiente brazo - pierna de más de 20 mm hg. Existe un soplo en el espacio interescapulo vertebral y signos radiológicos como la "E invertida " y el de Roessler ( 25 ). El diagnóstico apropiado se realiza con eco transesofágico, resonancia magnética nuclear y/o cateterismo (20,21 ) y el mismo puede realizarse desde estadios fetales in útero. (26). Tratamiento: La reparación quirúrgica fue realizada por vez primera por Crafoord en 1944 ( 22 ) con una resección del segmento coartado y anastomosis término terminal . Posteriormente Vosschulte en 1966 (23) describió la aortoplastía con parche de dacron dados los índices de reestenosis. En 1966 Waldhaussen (8) describe la aortoplastía con flap de subclavia izquierda. Recientemente se ha descrito la angioplastia con balon y colocación de stents autoexpandibles con buenos resultados sobre todo en recoartación (24 ).
Material y Métodos.
Se analizaron retrospectivamente los archivos clínicos de ochenta y un pacientes operados con el diagnóstico de coartación de la aorta en el Hospital México, San José, Costa Rica, en un período comprendido entre Enero de 1969 y Diciembre de 1999, anotándose hallazgos clínicos, radiológicos y los estudios hemodinámicos con aortograma y ecocardiograma. Se utilizaron diferentes técnicas de reparación a través de una toracotomía posterior izquierda, como son la resección con anastomosis termino terminal y la interposición de prótesis tubular de dacron. A partir de 1984 se ha usado la aortoplastía descrita por Vosschulte modificado con un parche de duramadre.
Postoperatoriamente se determinaron gradientes transaórticos y se controlaron valores de PA, además de complementar con estudios radiológicos y ecográficos en un período que osciló entre 0.2 y 30 a.
Hallazgos.
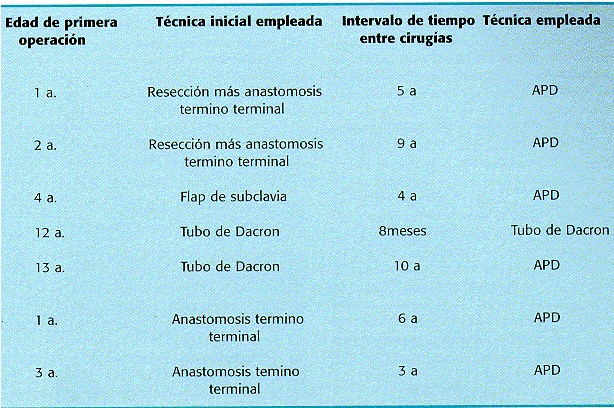
Un total de 81 pacientes fueron operados 56 de ellos hombres y 25 mujeres. El rango de edades osciló entre los 0 y los 53 a. con un promedio de 20.3 a. . Las manifestaciones clínicas fueron : 1) En niños menores de 1 a. : ICC ( 4ptes). 2) De los 2 a los 5 a : Cefalea, ausencia de pulsos femorales y claudicación.( 4 ptes ) y 3) En el resto de pacientes: HTA y claudicación intermitente de Ms Is. (73 ptes). Como defectos congénitos asociados se documentó un ductus arterioso permeable en el 31% de los pacientes así como una válvula aórtica con doble lesión, o insuficiencia mitral en el 19%, siendo estos hallazgos de hasta un 37% en otras series ( 28 ). Con respecto a la técnica quirúrgica utilizada, se ralizó (fig. 1) Resección con anastomosis termino terminal : 29 pacientes (36%), Interposición de tubo de Dacron :1 pte (1.2%), y aortoplastía con parche de duramadre 51 ptes ( 62.8%). Reoperaciones fueron practicadas en 7 pacientes, todos operados previamente en otros centros, los cuales fueron tratados con parche de duramadre en 6 casos y con tubo de dacron en uno (cuadro 1 ). ]]>
La morbilidad quirúrgica fue de un 16%, correspondiendo a neumotórax residual, hemotórax, arritmias postoperatorias e hipertensión en el postoperatorio inmediato. La mortalidad fue de 2.4% que correspondió a dos pacientes, uno de 4 meses de edad con ICC y bronconeumonía postoperatoria y uno de 23 a. con una reoperación con tubo de dacron que sangró de la pared costal siendo reintervenido múltiples veces presentando sepsis y fallo multisistémico.
]]> Con respecto a la hipertensión arterial el 84% de los pacientes se tornaron normotensos en el postoperatorio el 10 % obtuvo mejoría, siendo controlados con antihipertensivos satisfactoriamente y el 6% permaneció sin cambios. El gradiente de presión brazo pierna en reposo fue en todos los pacientes menor de 20 mmHg, con buena evolución (15). Durante el seguimiento de los pacientes no se han presentado complicaciones tardías derivadas de la cirugía como recoartación, endarteritis o formación de aneurisma cerca del parche, no habiendo necesidad de reoperar a ningún paciente de los originalmente intervenidos en nuestro centro.Comentario.
Desde principios de los 80 , la aortoplastía con la variación del parche de Duramadre descrito por Ross (16 ) se ha implementado en nuestro Servicio, siendo desde entonces la técnica de elección por las siguientes ventajas sobre las otras: A) El diámetro de la aorta permanece amplio aún en casos de niños en crecimiento, cosa que no sucede en todos los casos de anastomosis termino terminal y de interposición de tubo (1,3,17 ) B) Está demostrado que la aortoplastía con parche es más efectiva que la resección con anastomosis T-T en la reducción del gradiente transaórtico(3,8). C) La hemostasia es óptima puesto que toda la cirugía se realiza en el plano frontal de la aorta y no manipula la cara posterior la cual es de difícil abordaje( 15 ) y desde el punto de vista técnico nos resulta más cómodo de realizar. Finalmente, no utilizamos flap de arteria subclavia por la población adulta que actualmente manejamos ademas del sacrificio de la arteria subclavia que esta conlleva (2). Es así como la aortoplastía con parche de duramadre es la técnica preferida por nosotros tanto por ser técnicamente la más sencilla, así como por los resultados a largo plazo donde no hemos tenido complicaciones relacionadas a la misma, tales como son la reestenosis o la formación de aneurismas tardíos en un período que lleva 20 a.
Referencias
1 Morris G. Et al. Coarctation of the aorta with special emphasis upon improved techniques of surgical repair. J. of Thorac and Cardiovasc. Surgery, Vol 4 , Dec 1960. [ Links ]
2 Williams S.Pierceet al. Late results of the subclavian flap. Procedure in infants with coarctation of the thoracic aorta. Cardiovascular surgery 1977. Circulation suppl. 1 Vol 58, sept 1978 [ Links ]
3 Morris R. Sade et al .Aortoplasty compared with aortic resection in young children . Ann of Thor ac. Surg. Vol 28,oct 1979 [ Links ]
4 Gibbons ,Spencer .Cirugia toracica . Ed Salvat P 943-45, ed 1981. [ Links ]
5 Cowgill D. Corction of the aorta . Cardiac Surg. Vol.13 Jun 1987. [ Links ]
Litwin S.et al . Surgical resection of aortic coarctation of the aorta in infancy. Jour. Ped.Surg. 11:307, 1971 [ Links ]
7 Tawes L. Coarctation of the aorta in infants and children. Circulation ,39:173,1969. [ Links ]
8 Waldhaussen J. Repair of the coarctation of the aorta with subclavian flap. J. Thorac.Cardiovasc. Surg51:532,1966. [ Links ]
9 Palatianos G. Changing trends in the surgical teatment of aortic coarctation. Annals of thoracic surgery. Vol 40, jul 1985 [ Links ]
10 Morua E. Coartacion de la Aorta. Acta Med. Costarricense Vol.31:n2;1988. [ Links ]
11 Sabiston Textbook of surgery 16 th ed. WBSaunders Co 1996. [ Links ]
12 Findlow D. Congenital Heart disease in adults. Br J Anaesth. 1997;78(4):416-30 [ Links ]
13 Heineman NK. Extraanatomic Thoracic aortic by pass grafs. Indications ,Technics and results. Eur.J. Cardiothorac-Surg.1997;11(1):169-75 [ Links ]
14 Heger M. Aortic coarctation Long term follow-up in adults (Abstract) Z Kardiol 1997;86(1):50-5 [ Links ]
15 Guenthard J. Arm leg pressure gradients on late follow up after aortic coarctation repair. Possible causes and implications. Eur.Heart J. 1996;17(10):1572-75 [ Links ]
16 Ross D. comunicacion personal [ Links ]
17 Venturini A. Primary repair of coarctation of the aorta by patch graft aortoplasty. Eur J Cardiiothorac Surg. 1996;10(10):890-6. [ Links ]
18 Mc Connell M. Congenital diseases of the aorta. Rev Esp Cardiol 1996;49 Suppl. 4 :92-9. [ Links ]
19 Convens C. Aortic coarctation : A rare and unexpected cause of secondary arterial arterial hypertension in the elderly. CathetCardiovasc Diagn.1996 ;39(1):71-4. [ Links ]
20 Yamaguchi T. Intercostal artery aneurism associated with coarctation of the aorta: specific finding on MRI. Int J Card Imaging. 1997;13(4):357-8. [ Links ]
21 Linsay J. Diagnosis and treatment of diseases of the aorta. Curr Probl Cardiol. 1997 ;22(10): 485-542. [ Links ]
22 Crafoord S. Congenital coarctation of the aorta and its surgical management. Jthorac Cardivasc Surg, 1945 ; 14:347. [ Links ]
23 Vosschulte K. Surgical correction of coarctation of the aorta by an isthmuplastic operation. Thorax 1961;16: 338. [ Links ]
24 Descalzo-Sonorans A. Ballon percutaneus angioplasty in postoperative aortic coarctation. Rev Esp Cardiol. 1994; 47(4):247-50. [ Links ]
25 Hillis LD. Manual of Clinical problems in Cardiology, third ed. Little Brown, 1989. [ Links ]
26 Hornberger L. Antenatal diagnosis of coarctation of the aorta: a multicenter experience. J Am Coll Cardiol. 1994;23(2):417-23. [ Links ]
27 Janzen J . The disease picture of atypical aortic coarctation Helv.Chir.Acta 1993;60(1-2):291-8. [ Links ]
28 Poliakova N. Aortic coarctation and the bicuspid aortic valve. Ter Arkh. 1996;68(4) : 48-50. [ Links ]
29 Gire C. Rupture of cerebral aneurysm associated with aortic coarctation. Rev Neurol Paris .1997;153(5):357-8. [ Links ]
30 Tabandeh H. Retinal vascular abnormalities in aortic coarctation . Eye . 1996;10 (4) :525-7. [ Links ]
* Servicio de Cirugía Torácica y Cardiovascular Hospital México,
San José, Costa Rica.
e-mail:eiduni@medicos.sa.cr