Original
La institucionalización de la política universal de salud en Costa Rica y sus retos actuales
The Institutionalization of Universal Health Policy in
Jorine Muiser, MSc
*Dirección para correspondencia:
Abstract
Objective: To analyze the role of the Ministry of Health in Costa Rican public policy.
Methods: The analysis is a case study comparing two periods (1950 – 1990 and 1990 - 2010) using qualitative data collection instruments, including review of literature and institutional documents as well as in-depth interviews and focus group discussions, all with data triangulation.
Results: The analysis found important differences between two periods: before the 1990s,consecutive governments were strongly committed to the pursuit of universal health coverage (UHC); afterwards, resources moved to the Caja Costarricense de Seguro Social (CCSS) and the private sector, causing a chain of effects that complicated the search for financial sustainability.
Discussion: The 1990s health system reforms were a turning point in
Key words: Health Policy, Health Insurance, Public Policy (source: MeSH, NLM)
Resumen
Objetivo: Analizar el papel del Ministerio de Salud en la política pública costarricense.
Métodos: El análisis es un estudio de caso que compara dos periodos (1950 – 1990 y 1990 -2010) utilizando instrumentos de recolección de información cualitativos, incluyendo la revisión de literatura y documentos institucionales, además de entrevistas a profundidad y grupos focales, todo con triangulación de datos.
Resultados: El análisis encuentra diferencias importantes entre los dos periodos: antes de los 1990s, gobiernos consecutivos estaban fuertemente comprometidos para lograr la cobertura universal de salud (CUS); después, los recursos de poder se movieron hacia la Caja Costarricense de Seguro Social (CCSS) y el sector privado causando una cadena de efectos que complicó la búsqueda de sostenibilidad financiera.
Discusión: La reforma de salud de los 1990s fue un punto de cambio en el proceso hacia la CUS en Costa Rica. Buscando más eficiencia y sostenibilidad, la red de salud primaria se integró en el esquema de la CCSS lo que desencadenó un auge implícito en la actividad del sector privado, relacionado también con cambios en el contexto político-económico. El plan de fortalecer el papel de rectoría por parte del Ministerio de Salud no se efectuó. La CUS en Costa Rica cuenta con fuerte apoyo popular lo que le da cierto grado de sostenibilidad política, pero para garantizar la sostenibilidad financiera se requiere acción concertada del gobierno para mejorar la coordinación inter-institucional, sectorial e inter-sectorial.
The guard […] did not have social guarantees, so he never felt like a Costa Rican. ‘El vigilante (…) no tenía garantías sociales, por lo tanto no se sintió nunca un costarricense’ (1).
The population of
The analysis presented here describes not so much what the country has achieved, as thatis documented in previous studies (3-6), nor does it provide a historic actor centered analysis that was the focus of a paper complementary to this one (7). This study explores more in depth the role of the Health Ministry in the achievement and sustenance of UHC since the creation of the CCSS in
Concept definitions and methodology of research
This health policy analysis is part of a larger research project that aims to unravel the policy process of UHC in
Following the WHO definition, stewardship is considered ‘arguably the most important’ health system function that should primarily be exercised by the Health Ministry. The latter‘must oversee and guide the working and development of the nation’s health actions on the government’s behalf’. On top of that, the government-as-a-whole should assume the tasks that go beyond the Health Ministry’s mandate, including affecting the behavior of actors in other sectors of the economy. Stewardship at the level of government means guaranteeing coherence and consistency in the health policy process; at the level of health care purchasers and providers it implies guaranteeing that resources are used efficiently and equitably (8).
The analysis distinguishes the periods before and after the 1990s.In line with Walt and Gilson, for both of these periods, four groups of factors were analyzed: the key actors in the health policy process, the formal or written rules that prescribe their responsibilities and duties (content),the context in which they operate, and the informal rules that explain how they actually implement those rules (process). Actors and institutions are distinguished and assumed to reciprocally influence each other depending on their relative access to power resources, perceptions, interests, past experiences and policies (9) (10) (11).The approach differs principally from traditional institutionalism that only analyzes formal rules and neglects that implementation depends on the actors and their context. Qualitative instruments used to collect data and information include a review of previous studies on Costa Rica’s health system development and reform processes; a review of literature on historic socio-economic and political developments, as well as on public administration; a review of institutional documents, in particular health legislative documents, institutional rules and regulations and institutional annual reports; 17 in-depth interviews and 2 focus group discussions with institutional and non-institutional actors selected through a snow-ball mechanism prioritizing the representation of the main institutions: the Health Ministry, the CCSS and the private health sector.
Questions focused on: 1) how was universal health coverage achieved and sustained and within what context; 2) who were the key actors and how did they coordinate their actions; 3) what implied the role of stewardship in theprocess; and 4) what are the main challengestoday. Literature review was used mainly to further explore contextual changes over time, to analyze the relevant formal rules on UHC and to collect statistics describing health and social outcomes. Data triangulation distilled out the most broadly supported conclusions. The study limitations are the relatively restricted number of in-depth interviews carried out offeringpersonal perceptions of 17 key informants only.This is particularly important given the significant differences found in the perceptions of those related to the CCSS or Health Ministry respectively, in particular since the 1990s health sector reform.
Findings
The findings of the study are presented in three sub-sections focusing on changes before and after the 1990s in: context, formal rules, and actors, their relative access to power resources and process.
After the Second World War, in 1949,the abolition of the army and the social security scheme as designed originally,were integrated into a new Constitution passed by José Figueres’ short interim government that followed a 48-days-during civil war. After handingbackpower to the legitimate President,he was elected in 1953and 1970 respectivelyto continue his socio-democratic institution building process. While applauded by many, Figueres’ intentions have also been described critically and his interim government characterizedas a political system dominated by the ‘extreme center’ … ‘witha low tolerance to the dissidence in the extremes of the ideological spectrum’ (12). Indeed, he prohibited the communist party, and health policy, among other policies, was implemented largely top-down.
During the1950-1980s, consecutive governments in
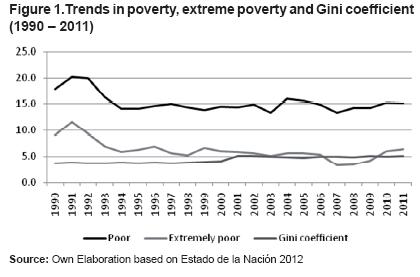
Health outcomes continue to remain favorable in
Constitutional rules
The 1949 Constitution formulates the responsibility of the state and consecutive governments for the well-being of
General rules
Improved inter-institutional coordination continues to be the goal of a series of reforms shaping Public Administration during the period 1950-
Specific health policy related rules
The 1961 Social Security Universalization Act commits consecutive governments in
It makes explicit that the definition of the national health policy, norms, planning and coordination of all public and private health related actions corresponds to the Executive Branch through the Health Ministry.The Actattributes power at times of national emergencies tothe Health Ministry to impose its authority over allpublic and private actors, but does not limit the Health Ministry’s mandate to such events (although it is sometimes interpreted as such).
The Health Ministry’s Organizational Act, also from 1973, reaffirms the leading role of the Health Ministry in health policy andconfirms that it exercises the jurisdiction and technicalcontrol over all public and private institutions that realize actions on health in all of its forms. It adds, however, that the actions of the Health Ministry in terms of service provision cannot damage those actions that are realized by other institutions, and that no other duty attributed to the Health Ministry by law or regulation can be of damage to the attributes the law gives to the autonomous institutions of the health sector. Willingly or not, the Actlimits the Health Ministry’s attributes to so-called negative coordination, implying government organizations and programs ‘merely to get out of each other’s way’ rather than to produce negative interactions among themselves (16).
The rule is one of several that limit the Health Ministry’s authority over other social actors. The same Act, for example, whileestablishing the National Health Advisory Board as an advisory organ responsible to collaborate with the Minister in the health policy formulation process, formally requiresthe CCSS and other institutions to send a representative, but not necessarily its leaders.In 1989, the National Health System is constituted by decree, positioning the autonomous institutions and private health sector once again within the Health Ministry’s domain, but without changing any of these legal imperfections.
The reform would reinforce the negative impact of the government’s structural avoidance since the 1980s, to timely pay its contributions to the CCSS and increase problems related to financial liquidity for the institution. After
The 1998 Des-concentration of
Notably, coordination as an instrument of public administration is not an unambiguous concept. Peters, referring to Scharpf (1964), distinguishes four degrees of coordination with an increasing investment of political capital. As mentioned above, negative coordination involves government organizations and programs to not disturb each other; positive coordination refers to working together; policy integration to different public organizations developing shared goalsto be pursued; and strategy development to having a clear vision for the future of policy and government. UHC could be an example of such a strategy and success towards achieving it may depend in a large part on the degree of coordination achieved within a certain context.
3. Actors, their relative access to power resources and process
Private health care providers, who had opposed the UHC scheme in the beginning, became neutral players by the 1970s. Health policies were reinforced by other social policies shaping apolitical and socio-economic context favorable to UHC (18). Solidaritybecamethe essence of
After the 1990s, universal social policies slowly faded out including the Health Ministry’s primary health care programs that have been considered central to
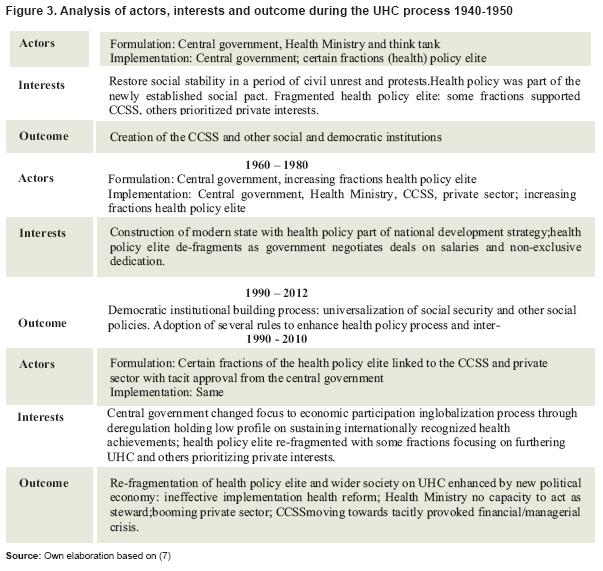
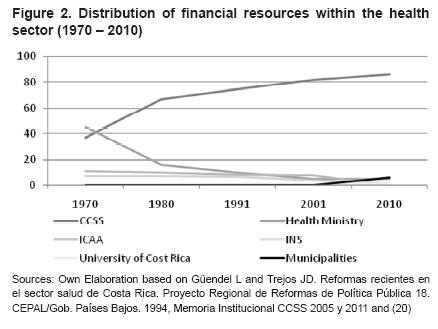
The Health Ministry lost most of its resources and leadership as the involvement of the government in health policy declined. As a result, the so-called ‘national authority’ in health ever really took control of the process. The government focused on economic policies that would allow a trend of implicit privatization on the health care market (19). Despite the fact that the Health Ministry was health system steward and resources were invested in strengthening this role, the institution never got properly equipped to direct the actions of the CCSS and other social actors. The private sector is not involved in the processes that relate to the stewardship of the Health Ministry… and the CCSS does whatever it wants ... it does exactly … what it feels like taking the luxury to not take into account anything the Health Minister says, because the Health Ministry does not have money (Key informant 2). Figure 3
Illustrative for the lack of power by the Health Ministry to impose its authority over the social actors, is how the CCSS over time started to neglect the National Health Advisory Board: Whether the Health Ministry convokes the CCSS? From a single provider and the one that had the health services, the Health Ministry transformed into steward, there was a change in the 1990s, a very big transformation at the level CCSS-Health Ministry. … It were times … with a lot of hassle and power games between those who worked in the Health Ministry and those who worked for the CCSS, because, those who have the money, strength, political power, and everything else; why would they have to sit and talk with the Health Ministry, for what reason? At that time, there was an absolute power of the CCSS, they said it is better not to go to the Health Ministry, because if I go, they will ask for money for this and for that …; so I better don’t go. So the second bosses started to go, not the Executive President, and later the third and then it died (Key informant 3).
Key informants blame the lack of capacity of the Health Ministry on the Structural Adjustment Programs …: The Health Ministry had its fundamental momentum (during the 1970s) and it fellwith the crisis of the 1980s. The oil crisis, that is when everything came down, and the only way to pay the State was reducing it, and on top of that, the concept that the State should not be in everything, and that the private firm should do the work, that were the SAPs of the 1980s … the aim (of the SAPs) was to reduce the State. In health this was a disaster (Key informant 4). …
It seemsthat before the 1990s, with the government leading the health policy process, and the Health Ministry, CCSS,andprivate health sectoreachoperating in their own domain, there was a sufficient degree of coordination. The CCSS was still ‘under construction’ and the private sector small. It accommodated the interests of the population with capacity to pay to elect their preferred provider and those of the medical doctors, to practice with no exclusive dedication. The public-private mix worked well controlling waiting lines and lists for primary and secondary care, while for specialized hospital care the CCSS was the best option for all.
The 1994 reforms while successful in bringing all personal health care services under one roof had some unintended outcomes. When health areas and primary health care teams were established across the country under CCSS management, private practitioners, working for the CCSS as well, found ways to catch the demand not served by the public institutionor maybe to sometimeseven push out CCSS demand to their private clinics: They (the private sector) have benefitted from the reforms more than anyone else; that is why you always see a ‘garden’ of private practices next to the services of the CCSS. Today you open a hospital in Heredia and they already open their private practices, because the CCSS will never be able to meet all the demand. They really benefitted from the reform, and in big, and they have filled their pockets. It is good, because the people have options (Key informant 1).
The trend triggered change that was leveraged by a new macro-political context. Not thereform as formulated, but the way it was implemented with no-one pushing for coordinated action, had by-effects in terms of a shift in the distribution of power on the health care market. Not the goal changed, but the process. With a weak Health Ministry, ‘holes’ in legislation got subject to interpretation by vested interests and reformsaimed to increase the financial sustainability of the CCSS and strengthen the Health Ministry’s stewardship role, were blocked. As a result, the shift from curative to preventive care did not take off; the Des-concentration Act was implemented only partially; a project to review the 1973 General Health Act presented by the Health Ministry in the early 21st centurynever got accepted; and the 2008 Health Ministry’s new regulation mentioned above was largely neglected by the CCSS and other social actors.
The increase in private sector activity made private health expenditure grow between 1999 and 2009 from 23,7 % to 32,6 %, and out-of-pocket payments from 20,9 % to 28,6 % of total health expenditure. So far, no or little catastrophic health expenditure has beenfound in
the electrification, all the vaccination campaigns,
the campaigns of shoes for the children. The impact of these actions is something we do not lose over night, but to sustain it, the actual model demands much more substantial efforts (Key informant 2).
Conclusion and discussion
In
Lessons for other countries from
Acknowledgements
This study has been carried out in cooperation with Juan Rafael Vargas, Johan Retana, Pablo Slon Montero, Ana Casanova and Monica Acosta. We acknowledge that the study that forms the basis for this article is financially and technically supported by the
1. Contreras Castro F. Única mirando al mar. San José.
2. Balabanova D, McKee M, Mills A. Good Health at Low Cost 25 Years On. What Makes a Successful health System? The
3. Miranda Gutiérrez G. La Seguridad Social y el Desarrollo en Costa Rica. San José, Costa Rica. UNED: 2003 http://www.editlegado.com/miranda-gutierrezguido-seguridad-social-desarrollo-costa-rica-p-1381.html. [ Links ]
4. Herrero F, Durán F. El sector privado en el sistema de salud de Costa Rica. Serie Financiamiento del Desarrollo 109. CEPAL Unidad de Estudios Especiales. Chile: 2001. [ Links ]
5. Rosero-Bixby L. Evaluación del impacto de la reforma del sector salud en Costa Rica. Revista Panamericana de salud Pública. 2004; 15 (2):94-103. http://ccp.ucr.ac.cr/bvp/pdf/salud/Rosero%20Evaluacion %20Reforma-RPS2004.pdf. [ Links ]
6. Zúñiga-Brenes MP, Vargas JR, Vindas A. Out-ofpocket and catastrophic health expenditure puzzle; The Costa Rican experience. Financing Health in
7. Vargas JR, Muiser J. Promoting universal financial protection: A policy analysis of introducing universal health coverage in
8. World Health Report 2000. Chapter 6. How is the public interest protected? 2000: 119. http://www.who.int/whr/2000/en/whr00_ch6_en.pdf. [ Links ]
9. Walt G and Gilson L. Reforming the health sector in developing countries: the central role of policy analysis. Health Policy and Planning. 1994; 9(4):353-370 http://info.worldbank.org/etools/docs/library/122031/ bangkokCD/BangkokMarch05/Week2/4Thursday/ S2EngagingStakeholders/ReformingtheHealthSector.pdf. [ Links ]
10. Subirats J, Knoepfel P, Larrue C, Varone F. Análisis y Gestión de Políticas Públicas. Ariel. Ciencia Política: 2008. [ Links ]
11. Flores W. Los principios éticos y los enfoques asociados a la investigación de la gobernanza en los sistemas de salud: implicaciones conceptuales y metodológicas. Ethical principles and approaches to health systems governance research: conceptual and methodological implications. Revista Salud Pública. 12:1. Bogotá: 2010. http://www.scielo.org.co/scielo.php?pid=S0124-0064201 0000700003&script=sci_arttext. [ Links ]
12. Sojo C. Igualiticos – La construcción social de la desigualdad en Costa Rica, San José, Costa Rica. PNUD. 2010: 68. [ Links ]
13. Moran M, Rein M. Immergut EM. Institutional Constraints on Policy.The Oxford Handbook of Public Policy. Edited by Goodin RE. Chapter 27. 2008: 560. [ Links ]
14. Saenz Madrigal MR, Ortiz Barboza A, Gutiérrez Miranda M, Bermúdez Madriz JL, Monge Hernández C. Perspectiva epidemiológica y socio institucional del cáncer de mama en Costa Rica. Heredia. UNA: 2011. [ Links ]
15. Jiménez Castro W.Un modelo tridimensional: instituciones, sectores y sistemas, aplicable a Costa Rica. Humanitas: Revista de Investigación. 2005; 1(1):27- 52. http://www.buenastareas.com/ensayos/Un-ModeloTridimensional-Instituciones-Sectores-y/314426.html. [ Links ]
16. Bouckaert G, Peters BG, Verhoest K. The Coordination of Public Sector Organizations Shifting Patterns of Public Management.Political & International Studies Collection. Series: Public Sector Organizations. 2010. [ Links ]
17. Jaramillo Antillón J. Historia y evolución del Seguro Social de Costa Rica: su primer hospital Dr. Rafael Ángel Calderón Guardia. San José. Costa Rica. EDNASSSCCSS 2004: 113-114. [ Links ]
18. Mohs Villalta E. La Salud en Costa Rica. Universidad Estatal a Distancia. San José: 1983. [ Links ]
19. Gamboa Cáceres T and Arellano Rodríguez M. Tendencias neoliberales en la reforma de la gestión pública en América Latina. Revista Gerencia y Políticas de Salud. 2007; 6(13):46– 65. Pontificia Universidad Javeriana. [ Links ]
20. Ministerio de Salud. Análisis sectorial de salud/ Ministerio de Salud, San José, Costa Rica: 2002: 266. [ Links ]
*Correspondencia a: Associate Researcher,
Recibido: 04 marzo 2013 Aprobado: 01 julio 2013
{kind=link}
{kind=link}
{kind=link}