Introducción
Desde la década de los años 60 y debido al desarrollo de técnicas para el soporte de los pacientes en estado crítico, han aparecido lesiones consecuentes a dicha invasión del cuerpo humano por catéteres y drenajes. La traquea no está exenta de tal invasión, y el efecto mecánico del Tubo Endotraqueal (TET) sobre la mucosa traqueal puede causar lesiones epiteliales debidas a la presión directa (14,18) y a la isquemia secundaria generada por la compresión del plexo submucoso (44,45,47). La expresión más grave de este tipo de lesiones es la estenosis traqueal que podría amenazar la vida del paciente ya de por sí comprometida por las enfermedades que indujeron su situación crítica. El monitoreo y control de los pacientes es trabajo rutinario en las Unidades de Cuidado Intensivo (UCI); sin embargo en nuestra institución son manejados, en algunas ocasiones, pacientes intubados en los salones de internamiento que permanecen así por largo tiempo debido a diferentes circunstancias, unas inherentes al paciente otras dependientes de la limitada infraestructura y de personal, que inclinan la balanza de la oferta y la demanda de servicios hacia la carencia. Sumado a esto se halló la ausencia de lineamientos estandarizados para el manejo de la vía aérea de tales enfermos. A causa de ésta situación llevamos a cabo este trabajo para demostrar las lesiones causadas por el TET y definir claramente los estándares para el manejo de pacientes intubados en nuestro hospital.
]]>
El propósito de este estudio es observar la relación de las lesiones traqueales, el tiempo de intubación y la presión del balón del TET y definir el tiempo máximo que se debe esperar para realizar la traqueostomía.
Pacientes y Métodos
Se tomaron en cuenta dos series de pacientes colectadas entre 1995 y 1997: la primera de 17 casos y la segunda de 18 pacientes, todos los cuales requirieron traqueostomía por intubación prolongada. Al segundo grupo le fue controlada la presión del balón del TET pre y postoperatoriamente. De todos los pacientes fueron tomadas biopsias traqueales de espesor total del 4o. anillo traqueal, justo en el momento de efectuarse la traqueostomía. Durante este procedimiento se observó y anotó la posición del balón del TET como sigue: Zona A: área subglótica. Zona B: área ístmica. Zona C: área infraístmica.
Para la evaluación de los resultados se tomaron en cuenta como factores de exposición más de 14 días de intubación y más de 30 cmH2O en la presión del balón del TET.
Todas las biopsias fueron procesadas en forma estandard, teñidas con Hematoxilina-Eosina y analisadas con microscopía de luz. Con el fin de obtener un valor cuantitativo de las lesiones traqueales se diseñó la siguiente tabla de calificación:
]]>
| | |
| CARACTERISTICA | |
| Ulceración | |
| - del epitelio superficial | |
| - de la submucosa | |
| - del pericondrio | ]]> 3 |
| - ulceración profunda con exposición del cartílago | |
| - necrosis o degeneración del cartílago | |
| Epitelio adyacente a la ulceración | |
| - regeneración epitelial mínima | |
| - metaplasia escamosa focal | |
| - metaplasia escamosa extensa | |
| - ausencia de epitelio por necrosis extensa | |
| Vasos sanguíneos | |
| - vacíos o dilatados | |
| - dilatación con congestión superficial | ]]> 2 |
| - dilatación con congestión profunda | |
| - trombosis | |
| Estroma | |
| - edema | |
| - necrosis + edema | |
| - proliferación de tejido de granulación | |
| - proliferación de fibroblastos | |
| Respuesta inflamatoria | |
| - perivascular | |
| - limitada a la submucosa | ]]> 2 |
| - submucosa con extensión | |
| Mínima intraepitelial | |
| - submucosa + intraepitelial extensa | |
| Colonización por bacterias | |
| - ausente | |
| - presente | |
| Colonización por hongos | |
| - ausente | |
| - presente | |
| Puntaje mínimo posible: 5 - Puntaje máximo posible: | ]]> 23 |
| | |
Debido a que el rango de lesiones de todos los pacientes estuvo entre 7 y 19 puntos con una media de 13; se tomó valor representativo de lesión histológica signigficativa un grado de lesión igual o mayor de 13. Los resultados fueron analizados usando el programa estadístico de Epi-info.
Resultados
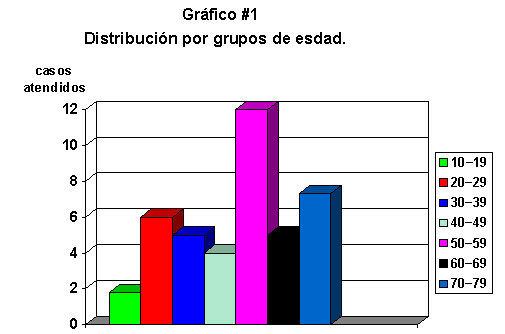
El total de la muestra de 35 pacientes tuvo representación etaria en todos los grupos, con una predominancia del grupo de 50 a 59 años; con un promedio de edad de 50,45 años, con una mínima de 14 y máxima de 76 años, con una mediana de 53 y moda de 54 años. En general predominaron los pacientes mayores de 50 años, como se ve en el gráfico #1.
Todos los pacientes estuvieron intubados por periodos significativos con un rango de 5 a 55 días, con un promedio de 17,34 días y una mediana de 14 días. La posición del balón del tubo endotraqueal se observó así: 6 pacientes lo tenían localizado en el área A, 7 en el área B y 22 lo tuvieron en el C.
Los 18 pacientes de la segunda serie a quienes se les midió la presión del balón del tubo endotraqueal tuvieron un rango de 25 a 34 cm de presión de agua (cmH2O), con un promedio de 28,67cmH2O y una moda de 25,0cmH2O.
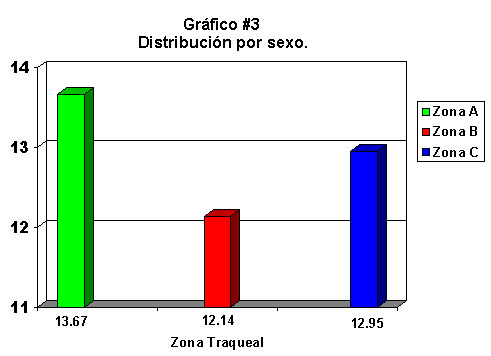
El grado de lesión promedio en los pacientes que tenían localizado el balón del tubo en la zona subglótica (zona A) fué de 13,67, en los que estuvo ubicado en el área istmica (zona B, de la biopsia y traqueostomía) de 12,14 y en los que se ubicó en el área infraistmica (zona C) fué de 12,95.
La relación entre los días de intubación y el grado de lesión histológica muestra que a mayor periodo de intubación la lesión tiende a ser mayor. Cuando se analiza los enfermos expuestos al riesgo de permanecer más de 14 días intubados con el hecho de tener una lesión histológica significativa (mayor o igual a 13 puntos), se encuentra un riesgo relativo de 1,89 ( Límite de Confianza 95% - serie de Taylor -); con un valor Chi=3,35 y valor p= 0,067.
La relación de los pacientes expuestos a presiones en el balón del TET iguales o mayores de 30 cmH2O, se encontró que el riesgo relativo de éstos de tener una lesión histológica significativa (> 13 puntos) es de 3,93 (Límite de Confianza 95% -serie de Taylor); con un valor de Chi de 4,82 y p=0,028.
El riesgo relativo de los pacientes que no tuvieron control de la presión del balón de tener una lesión significativa es de 1,66 (Límite de Confianza 95%-serie de Taylor), con un valor Chi=2,27 y p=0,132.
Discusión
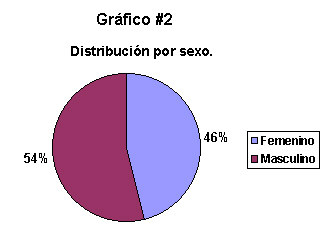
El predominio de un grupo de edad mayor de 50 años refleja en cierta forma la tendencia de la pirámide poblacional de nuestra sociedad, que con el pasar de los años se invierte y hace necesario que las políticas de salud del sistema se adecúen a tal situación; y la distribución de los pacientes por sexo indica que ambos grupos enfrentan riesgos y requieren de atención intensiva en proporciones prácticamente iguales,
A pesar de las recomendaciones dadas en 1995(45), persisten manteniendose los pacientes intubados por largos periodos (17,34 días en promedio); ésto aunado a la evidencia estadística obtenida en este estudio, de que el hecho de permanecer intubado más de 14 días representa para el paciente un riesgo real de padecer una lesión traqueal secundaria al tubo endotraqueal, hace necesario proponer y recomendar de nuevo pautas en el manejo de la vía aérea de los pacientes críticamente enfermos pues el riesgo relativo es prácticamente de 2:1.
Existe evidencia anatomopatológica de lesiones traqueales significativas en áreas de la traquea que no están en contacto directo con el balón del TET, hecho puesto en evidencia por 22 casos en que el balón se halló en la región infraístmica-distal al sitio de toma de la biopsia- los cuales tuvieron un promedio de lesión de 12,95; lo que habla de que no solamente el balón del tubo produce lesión traqueal sino que también el resto del tubo por sí; además, los hallasgos histológicos informan que gran parte de las lesiones son de origen isquémico por la compresión que ejerce el balón sobre el plexo vascular submucoso de la traquea. Al mismo tiempo llama la atención que cuando el balón se encontró situado en las zonas A y C (proximal y distal) de la traquea los promedios de lesión son notablemente más altos que cuando el balón se sitúa en la región media de la traquea, lo que hace pensar que en éstas ubicaciones el balón compromete la irrigación proporcionada por las arterias más importantes de la Arteria Longitudinal Lateral (Pedículo de Grillo) (Salassa-Pearson 1977) provenientes de la Arteria Tiroidea Inferior y de las Arterias Bronquiales.
Los hallazgos relativos a la relación existente entre la presión del balón del TET y la lesión traqueal comprueban en primer lugar que no controlar la presión del balón es exponer al paciente a un riesgo 1,66 veces mayor de sufrir una lesión traqueal significativa secundaria al TET; en segundo lugar que a mayor presión del balón, mayor es la lesión traqueal y que cuando la presión del balón alcanza y supera los 30 cmH2O el riesgo relativo es de 3,93:1, con una significancia estadística importante (Chi=4,82 y p=0,028). Esto indica que este control debiera establecerse en con caracter obligatorio y rutinario ]]>
Conclusiones y recomendaciones
1.-Existe evidencia anatomopatológica de lesiones traqueales significativas en zonas que no están en contacto con el balón del tubo endotraqueal (TET); probablemente relacionadas con el efecto mecánico del TET en sí y con la compresión del plexo vascular submucoso de la traquea por parte del balón.
2.-Permitir que un paciente pase intubado más de 14 días, sin realizarle traqueostomía, expone al paciente a un riesgo 1,89 veces mayor de sufrir una lesión traqueal significativa secundaria al TET.
3.-El hecho de no cuantificar ni controlar la presión del balón del TET expone al paciente a un riesgo relativo de 1,66:1 de tener una lesión traqueal significativa con respecto a aquellos pacientes a quienes sí se les controla.
4.-A mayor presión del balón del TET mayor es la lesión traqueal desarrollada por el paciente.
5.-Cuando la presión del balón excede los 30 cmH20 el riesgo de desarrollar una lesión traqueal significativa es 3,93:1.
6.-Se recomienda adoptar las siguientes medidas con respecto al manejo de la vía aérea en los pacientes críticos con ventilación mecánica:
a.-Se puede mantener un paciente intubado sin problema por 7 días mientras se logra estabilizar su situación crítica. Si la causa primaria de su fallo respiratorio indica que va a permanecer intubado por largo tiempo debe realizarse la traqueostomía en ésta primera semana;(ej. Lesión neurológica severa).
b.-Durante los siguientes 7 días los pacientes que aún permanecen intubados deberán evaluarse diariamente por la posibilidad de ser extubados; pero cuando la evidencia clínica indique que va a sobrepasar los 14 días de intubación, deberá realizarsele traqueostomía. Ningún paciente debería permanecer con tubo endotraqueal más de 14 días. ]]>
c.-Debe establecerse que la medición de la presión del balón del tubo endotraqueal sea obligatoria en los pacientes intubados al menos una vez al día (idealmente una vez en cada turno), y registrada en la tabla de cuidados respiratorios; ya sea que fuese medida por el médico a cargo, por la enfermera del servicio o por el técnico de terapia respiratoria. d.-La presión del balón deberá manejarse en un rango entre los 20 a los 29 cm de presión de agua. Cuando el paciente se encuentre hipotenso el límite superior deberá reducirse a 25 cmH2O.
Bibliografía
1.-Arnold, W. Iatrogenic changes of the trachea. Diseases of head and neck, an atlas of histopathology. Cap 9. [ Links ]
2.-Astrachan,D. Prolonged intubation vs. tracheotomy: complications, practical, and psycological considerations. Laringoscope. 1988;98:1165-9 [ Links ]
3.-Ayes,F- J.Zafra. Estenosis traqueal. Experiencia de 15 años en el Hospital San Juan de Dios. CENDEISSS. No publicado [ Links ]
4.-Benizhak,O. Necrotizing squamous metaplasia in herpetic tracheitis following prolonged intubation: a lesion similar to necrotizing sialometaplasia. Histopathology. 1993;22:265- 269 [ Links ]
5.-Bishop, M. Mechanisms of laryngotracheal injury following prolonged tracheal intubation. Chest. 1989;96:185-90 [ Links ]
6.-Bunegin,N. Canine tracheal blood flow after endotracheal tube cuff inflation during normotension and hypotension. Anesth.- Analg. 1993;76(5):1083-90 [ Links ]
7.-Coleman,J. Traumatic lesion of the trachea. Otolaryng.Clin.N.A. August,1995 [ Links ]
8.-Colice,G. Laryngeal complications of prolonged intubation. Chest. 1989;96:877-83 [ Links ]
9.-Colice,G. Resolution of laryngeal injury following translaryngeal intubation. Am.Rev.Resp.Dis. 1992;145:361-364 [ Links ]
10.-Coppolo,DP. Self extubation; a 12 month experience. Chest. 1990;98:165-9 [ Links ]
11.-Chuzonagaishi,MD. Functional anatomy and hystology of the lung. Public University.Park Press. Baltimore,1972 pp:5-12 [ Links ]
12.-Delgado, A. Tracheal reconstruction. Rev. Laryngol.Otol.Rhinol.Board. 1993;114(1):21-4 [ Links ]
13.-Donnelly,W. Laryngotracheal damage after prolonged use of orotracheal tubes in adults. JAMA. 1969;207(4):703-708 [ Links ]
14.-Donnelly,W. Histopathology of endotracheal intubation. Arch. Pathol.1969;88 [ Links ]
15.-Dunham,M. Prolonged intubation in the trauma patient. J.Trauma. 1984;24(2):120-24 [ Links ]
16.-Eliachar,I. Imaging evaluation of laryngotracheal stenosis. J. Otolaryngol. 1993;22(4):265-77 [ Links ]
17.-Faria, V. The complicatios of tracheal intubation, a new classification with a review of literature. Anesth.- Analg.1974;53(2) [ Links ]
18.-Grillo,H. - Cooper. The evolution of tracheal injury due to ventilatory assistance trough cuffed tubes: a pathologic study.Ann.Surg. 1969;169(3):334-48 [ Links ]
19.-Grillo,H- Cooper. Experimental production and prevention of injury due to cuffed tracheal tubes. Surg.Gynecol.Obstet. 1969;129:1235 [ Links ]
20.-Grillo,H-Cooper. A low pressure cuff for tracheostomy to minimize tracheal injury-A comparative clinical trial. J.Thorac.Cardiovasc.Surg. 1971;62:898 [ Links ]
21.-Grillo,H. Surgical treatment of postintubation tracheal injuries. J.Cardiovasc.Surg. 1979;78(6) [ Links ]
22.-Grillo,H. Upper airway Compromise after inhalation injury. Complex Strictures of larinx and trachea and their management. Ann.Surg.1993;218(5):672-8 [ Links ]
23.-Grillo,H. Idiopathic laryngotracheal stenosis and its management. Ann.Thor.Surg. 1993;56(1):80-7 [ Links ]
24.-Heffner,J. Timing the tracheostomy in mechanically ventilated patients. Am.Rev.Resp.Dis. 1993;147(3):768-71 [ Links ]
25.-Heffner, J. Tracheostomy en the Intensive Care Unit. Chest. 1986;90(3) [ Links ]
26.-Holgaard,H. Complications and late sequelae following nasotracheal intubation. Acta Anaesth.Scand. 1993;37(5):475-80 [ Links ]
27.-Lester,B. Bacterial colonization profile with tracheal intubation and mechanical ventilation. Arch. Surg. 1972;104:647 [ Links ]
28.-LoCicero,J. Tracheo-carotid artery erosion following endotracheal intubation. J. Trauma. 1984;24:907-09 [ Links ]
29.-Mansour,K.Tracheal resections:lessons learned. Ann.Thorac.Surg. 1994;57(5):1120-4 [ Links ]
30.-McCafrey,T. Management of laryngotracheal stenosis on the basis of site and severity. Otolarygol.Head and Neck Surg. 1993;109(3):468-73 [ Links ]
31.-McGinnis, G. An enginnering analysis of intratracheal tube cuff. Anesth- Analg. 1971;50(4) [ Links ]
32.-Miller,D. Tracheal stenosis following prolonged cuffed intubation. Ann. Surg. 1970;171(283) [ Links ]
33.-Paegle, R. Rapid tracheal injury by cuffed airway and healing with loss of ciliate epithelium. Arch.Surg. 1973;106 [ Links ]
34.-Pearson,F. Incidence and pathogenesis of tracheal injury following cuffed tube tracheostomy with asisted ventilation. Ann. Surg. 1971;173(2)249 [ Links ]
35.-Pearson, F. Thoracic Surgery,Churchill-Livingstone. New York.1995 [ Links ]
36.-Staufer,J. Complications and consequences of endotracheal intubation and tracheostomy. Am.J.Med. 1981;70:65-76 [ Links ]
37.-Shields,T. General Thoracic Surgery. Williams & Wilkins.Baltimore. 1994. 4th.Ed. [ Links ]
38.-Schmidt,W. Inmediate mucosal effects of short-term soft cuff endotracheal intubation. Arch.Pathol.Lab.Med. 1979;103 [ Links ]
39.-Stockh. Structure of the tracheal wall after different durations of intubation.Acta Otolaryng.Suppl.1977;245:1-71 [ Links ]
40.-Tayal,V. Tracheostomies. Emerg.Clin.N.A. 1994;12(3):707 [ Links ]
41.-Whited, R. A prospective study of laryngotracheal sequelae in long term intubation. Laryngoscope. 1983;94:367-77 [ Links ]
42.-Weymuller, E. Quatification of intralaryngeal pressure exerted by endotracheal tubes. Ann.Otol.Rhinol.Laryngol. 1983;92:444-46 [ Links ]
43.-Wright, P. In vitro vs. in vivo comparison of endotracheal tube airflow resistence. Am.Rev.Resp.Dis.1989;140:10-6 [ Links ]
44.-Rodríguez,L. Estudio histológico de las lesiones traqueales en pacientes con intubación prolongada. Tesis de Graduación de Postgrado en Anatomía Patológica. CENDEISSS-UCR.1998 [ Links ]
45.-Miranda, J. Estudio clínico-patológico de las lesiones traqueales en pacientes con intubación prolongada. Tesis de Graduación de Postgrado en Cirugía General. CENDEISSS-UCR.1995 [ Links ]
46.-Salassa JR, Pearson BW et.al. Gross and Microscopical blood supply of the trachea. Ann Thorac Surg 24:100-107,1977 [ Links ]
47.-Allen,M. Surgical Anatomy of the Trachea.Chest Surgery Clinics of N.A. 6(4) November,1996 [ Links ]
*Servicio de Cirugía 2 y Tórax,
**Servicio de Anatomía Patológica
Hospital San Juan de Dios. C.C.S.S. ]]>