Resumen
Los tumores de Koënen constituyen uno de los signos mayores de la Esclerosis Tuberosa y se encuentran en un 50% de los pacientes con esta enfermedad. Son proliferaciones típicas periungüeales que causan trastornos en la tableta ungüeal. Se consideran la variante hereditaria del fibroqueratoma que se origina del repliegue ungüeal proximal o del tejido conectivo de la zona. En el abordaje quirúrgico se debe pediculizar el tumor y llegar hasta su base de implantación, lo cual requiere de la reflexión del repliegue ungüeal proximal. Se describe e ilustra el abordaje quirúrgico de un caso.
Palabras clave
Tumor de Koënen, fibroqueratoma hereditario, esclerosis tuberosa, enfermedad de Pringle-Bourneville, tumor fibroepitelial
]]>
Koënen tumor represents one of the main signs of the Tuberous Sclerosis, they are present in 50% of the patients with this illness. They are common ingrowings around the nail tissue which causes dysfunction in the nail. They are considered an hereditary variant of the fibrokeratoma which originates in the proximal nail fold or in the surrounding connective tissue. In the surgical approach, the tumor needs to be dissected up to its base, this requires the reflection of the proximal nail fold. The surgical procedure of a case is described and illustrated.
Key words
Koënen Tumor, hereditary fibroqueratoma, tuberous sclerosis, Pringle-Bourneville disease, fibroepitelial tumor
Introducción
Los tumores fibroepiteliales del aparato ungüeal son condiciones dermatológicas benignas que pueden ser adquiridas o asociadas a la Esclerosis Tuberosa o a la Neurofibromatosis (1). Su aspecto difiere según su localización (superficial o profunda), pueden ser únicos o múltiples
Los tumores de Koënen constituyen uno de los signos mayores de la Esclerosis Tuberosa o enfermedad de Pringle-Bourneville. En la mitad de los casos aparecen durante o después de la pubertad (2, 3). Se encuentran en un 50% de los pacientes con esta enfermedad (3).
Estos tumores son proliferaciones típicas periungüeales color piel, alargadas, con una extremidad libre cornificada, que se desarrollan por debajo del repliegue ungüeal proximal y descansan sobre el plato. Cuando son múltiples, a menudo se disponen en semicírculo en la base de la uña. Su crecimiento a nivel del aparato ungüeal causa una presión excesiva que a nivel de la matriz ungüeal da como resultado depresiones longitudinales en la tableta ungüeal, o al localizarse debajo pueden levantarla e incluso destruirla (2). A las formas frustras cuya presencia solo es revelada por la existencia de una depresión canalicular longitudinal discreta, se oponen las lesiones fibromatosas exuberantes múltiples (4).
Desde el punto de vista histológico se observan generalmente dos partes distintas: un segmento distal estrecho formado por fibras de colágeno laxo y rico en vasos sanguíneos, y una zona proximal formada por haces de colágeno denso orientados en el eje del tumor, menos rico en capilares (4). ]]>
Estos tumores se prestan a un diagnóstico diferencial con otras patologías como las verrugas vulgares, los granulomas piógenos, los cuernos cutáneos, pero la histología y el contexto clínico permiten diferenciarlos (5).Presentación del caso
Paciente femenina de 15 años, sin antecedentes de patología similar en la familia, con una y única hermana 3 años mayor y sana.
Presentó estenosis de válvula aórtica tratada a los 4 años mediante dilatación a través de catéter. Diagnosticada portadora de Esclerosis Tuberosa mediante biopsias y estudio histológico de lesiones en piel y estudios radiológicos de Sistema Nervioso Central, ha presentado crisis de epilepsia desde el año y medio de edad, tratada con valproato de sodio, sin crisis desde hace 10 años. Con manifestaciones de angiofibromas en la cara, máculas hipocrómicas múltiples a nivel del tronco, fibroqueratomas digitales y retraso mental leve a moderado.
En la actualidad la paciente presenta tumores de Koënen únicos a nivel de dedos 3 y 5 de la mano izquierda y múltiples en varios ortejos de ambos pies. Presenta además procesos inflamatorios y sangrados post-traumáticos a repetición, molestias funcionales con uso de calzado y con la utilización de las manos en las labores cotidianas. Razones que motivaron la solicitud de intervenir para su eliminación.
Descripción del procedimiento quirúrgico
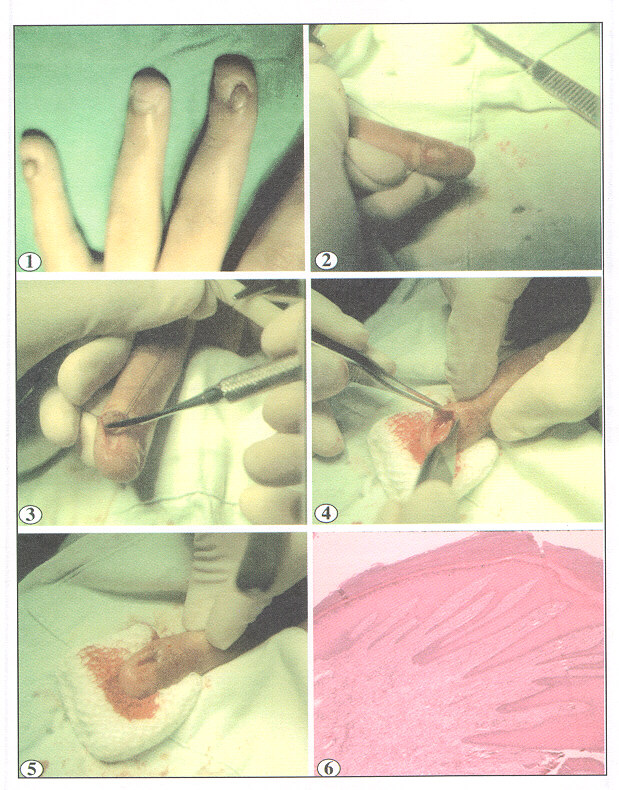
Se efectuó la exéresis quirúrgica del tumor de Koënen del tercer dedo izquierdo de localización sobre el surco lateral interno, de 0,5 cm. de ancho por 0,8 de largo, que ha impreso una depresión canalicular sobre el margen lateral de la tableta ungüeal (foto 1) ]]>
Previa asepsia de la mano izquierda se efectuó la anestesia troncular del tercer dedo y aplicación de torniquete a nivel de la base para mantener el sitio operatorio exangüe. Se efectuó una incisión longitudinal del repliegue cutáneo sobre el tumor, se aplicaron puntos para tracción y separación de ambas mitades del repliegue (foto 2), se efectuó una disección roma a lo largo del tumor y en toda su periferia hasta obtener la separación completa (foto 3). Se efectuó la disección y corte de la base del tumor mediante bisturí con la precaución de no lastimar la matriz ungüeal que se visualizaba por debajo del tumor (foto 4). Se efectuó la reconstrucción del repliegue supra-ungüeal mediante la aplicación de un punto simple distal con Nylon 5-0 (foto 5).La histopatología del tumor mostró una hiperplasia epitelial con proliferación de fibroblastos orientados en el eje mayor del tumor (foto 6).
La evolución posoperatoria inmediata no tuvo complicaciones, el repliegue ungüeal proximal presentó una buena cicatrización, manteniéndose aún la deformidad canalicular sobre la tableta a dos meses posexéresis. A ocho meses de la cirugía no ha habido recidiva del tumor y la tableta ungüeal ha restablecido en un 80%.
Discusión
La patología del aparato ungüeal y su manejo siguen siendo un campo poco conocido en la formación del médico general y del dermatólogo, a pesar de ser ésta muy amplia tanto como manifestación de enfermedad sistémica, como también de enfermedad cutánea ya sea localizada o generalizada.
Los tumores de Koënen pueden ser considerados una variante hereditaria del fibroqueratoma que se origina del repliegue ungüeal proximal o del tejido conectivo de la zona (3)
Estos tumores a pesar de ser lesiones benignas causan molestias de índole funcional para las labores cotidianas, dolor por la presión del calzado, sangrado y patología infecciosa agregada por su traumatismo, repercuten en la salud de la persona. Razones que justifican su conocimiento y abordaje.
En cuanto al tratamiento, la excisión quirúrgica completa de la lesión pareciera ser la más recomendada (2, 3, 6-9). La destrucción del tumor mediante electrofulguración u otras técnicas que producen extensa necrosis pueden afectar negativamente la estructura de la matriz ungueal y producir secuelas en la arquitectura normal de la uña, por lo que estos procedimientos no se recomiendan. El tratamiento quirúrgico es el recomendado y debe ser amplio, debe resecarse el tumor, pediculizarlo y llegar hasta su base de implantación, lo cual requiere la reflexión del repliegue ungüeal proximal (10). No es necesario hacer una resección del tejido cutáneo en relación al tumor. ]]>
El reconocimiento de estos tumores es fácil, su abordaje plantea dudas por la falta de conocimiento, a pesar de que la técnica quirúrgica es sencilla y está al alcance de todos.Agradecimientos
Al Dr. Miguel Meléndez por haberme permitido intervenir en su paciente. Al Dr. Enrique Freer por el análisis y sugerencias al manuscrito.
Referencias
1 Baran RL, Dawber RR. Guide medico-chirurgical del onychopaties, 2 ed., Paris Francia: Arnette Blackwell SA.,1995:80-81. [ Links ]
2 Baran R, de Berker D, Dawber R. Nails: appearance and therapy, United Kingdom: Martin Dunitz Ltd, 1993:48. [ Links ]
3 Berger RS, Spielvogel RL Dermal papule on a distal digit. Acquired digital fibrokeratoma. Arch Dermatol 1988;124:1559-1560,1562-1563. [ Links ]
4 Chin FE, McCarthy DJ. The cytological and biochemical implications of periungual fibroma. J Foot Surg 1992;31:486-497. [ Links ]
5 Freedberg IM, Eisen AZ, Wolf K, et al. Fitzpatricks dermatology in general medicine, 5 ed., United States of America: McGraw-Hill, 1999:2148-2151 [ Links ]
6 Kint A, Baran R. Histopathologic study of Köenen tumors.Are they different from acquired digital fibrokeratoma? J Am Acad Dermatol 1988;18:369-372. [ Links ]
7 Pasyk KA, Argenta LC. Argon laser surgery of skin lesions in tuberous sclerosis. Ann Plast Surg 1988;20:426-433. [ Links ]
8 Tisa LM, Iurcotta A. Solitary periungual angiofibroma.An unusual case report. J Am Pediatr Med Assoc 1993;83:679-680. [ Links ]
9 Vinson RP, Angeloni VL.Acquired digital fibrokeratoma. Am Fam Physician 1995;52:1365-1367. [ Links ]
10 Ward PE, McCarthy DJ. Periungual fibroma. Cutis 1990;46:118-124. [ Links ]
]]>