Leiomioma, leiomioma pilar múltiple.
Abstract
The pilar leiomyoma is an uncommon benign skin tumor diagnosed more frequently in young adults. lt appears as single lesion or more often multiple lesions, which have their onset early in the life on the second decade.
They could be nonsymptomatic but more often they are tender or slightly painful. Malignancy of these tumors is uncommon. Diagnosis is often done by histology characteristics of the lesion. We report in this paper a 28 years old patient having smooth, firm, slow growing nodules during the last 8 years, pink to yellowbrown color with tendency to coalesce in the extensor part of the arms and upper back. Some of them were tender. Histology analysis of the biopsy showed interweaving bundles of spindle-shaped cells localizad in the dermis which were strongly eosinophilic having long and thin nuclei and corresponding to the arrector pilorum muscles.
Key words
Leiomyoma, multiple pilar leiomyoma.
]]>
La dermis contiene fibras musculares lisas en los músculos piloerectores, la pared de los vasos sanguíneos y en el músculo dartos del escroto, areola, vulva y pezón (1, 2). Podemos encontrar tres tipos de lesiones tumorales musculares lisas: hamartomas, leiomiomas y leiomiosarcomas (3), aunque estos últimos son muy infrecuentes. Las células musculares lisas se caracterizan histológicamente por ser fusiformes, eosinófilas, con citoplasma fibrilar y núcleo en forma de cigarro.Histoquímicamente podemos demostrar la presencia de alfa actina y desmina (2, 3).
Los leiomiomas de la piel los podemos clasificar en tres categorías: a) leiomioma múltiple o solitario del músculo piloerector, b) angioleiomiomas del músculo liso de la túnica media de las venas y c) leiomiomas del músculo dartos en genitales, areola o pezón (2, 4). Los leiomiomas pilares son los más frecuentes (4-6), tienen un tamaño variable desde varios milímetros hasta 1 centímetro. Son nódulos lisos, firmes de color eritematoso a café claro o pardo (5). Los tumores tienen tendencia a agruparse formando placas de lesiones localizadas, generalmente en tronco, parte proximal extensora de extremidades, cara y cuello (1, 3, 4). Los grupos de lesiones generalmente se localizan en varias áreas. Las lesiones son generalmente sensibles al tacto y algunas son dolorosas espontáneamente (1-3, 5) por lo que el paciente tiende a consultar.
Cuando los leiomiomas pilares son múltiples, estos aparecen en etapa de adulto joven y continúan formándose hasta llegar a ser muy numerosos (6). En pacientes con cientos de tumores se ha descrito una transmisión autosómica dominante de penetrancia variable (3).
La histología de todos los tipos de leiomioma es similar y de fácil diagnóstico, pues, presentan haces de células de músculo liso poco delimitados (1), entrelazadas con fibras colágenas localizadas en la dermis que a veces infiltran el subcutis (2). Generalmente la tumoración está separada de la epidermis y tiene origen en el músculo arrector del pelo (1, 2). Las células musculares se tiñen de rosado con hematoxilina-eosina y contienen núcleos alargados localizados centralmente.
Presentación del caso ]]>
Este tumor es muy poco frecuente en Costa Rica. A pesar de ser un tumor benigno de muy baja incidencia el diagnóstico clínico de leiomioma pilar debemos tenerlo presente en el caso de nódulos solitarios o múltiples cuando se presentan en gente joven y estas personas aducen dolor de las lesiones (6). El diagnóstico clínico es difícil inicialmente porque no se piensa en este tumor (5). El diagnóstico diferencial debe hacerse con neurofibromas pero usualmente estos tienen una consistencia más suave, son de color piel, la distribución es más generalizada y se asocian a la presencia de máculas color café con leche de la neurofibromatosis tipo I. Otra lesión puede considerarse como diagnóstico diferencial es el hidrocistoma (4). Hay muy poca evidencia de transformación maligna de los leiomiomas cutáneos (1, 3). El tratamiento de elección en los tumores solitarios es la excisión quirúrgica (4, 6). En este paciente que desea la eliminación de los tumores debe evaluarse el beneficio cosmético de resecarlos quirúrgicamente contra las posibles cicatrices del procedimiento. Debido a la profundidad de los tumores y de su localización, la criocirugía y la cirugía con radiofrecuencia pueden dejar cicatrices similares. La ablación con láser no se recomienda.
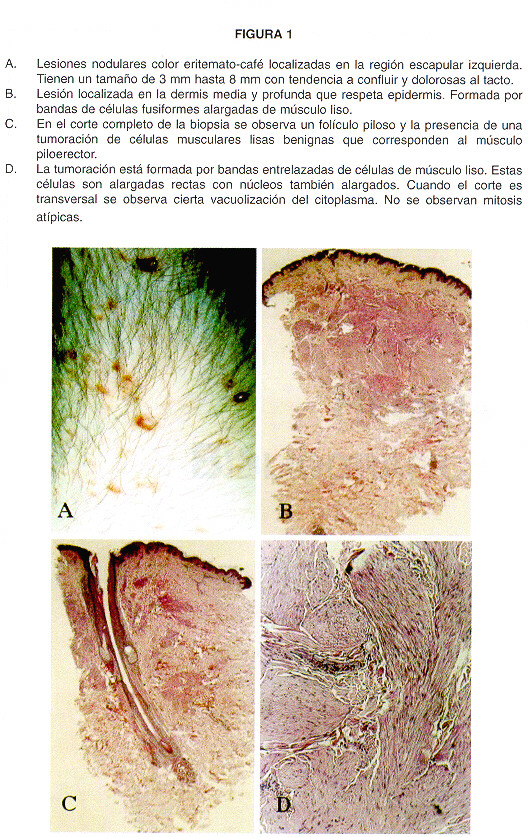
El diagnóstico histológico en este caso no presenta dificultad. El corte histológico de la lesión observada a bajo aumento muestra que está localizada en la dermis media y profunda respetando la epidermis (Fig 1B) y formada por bandas de células fusiformes alargadas de músculo liso. Se puede observar un corte completo de un folículo piloso y la presencia de una tumoración de células musculares lisas benignas que corresponden al músculo piloerector (Fig. 1 C). D. La tumoración está formada por bandas entrelazadas de células de músculo liso. Estas células son alargadas rectas con núcleos también alargados. Cuando el corte es transversal se observa cierta vacuolización del citoplasma. No se observan mitosis atípicas (Fig. 1 D).
En algunas tumoraciones es difícil diferenciar las fibras musculares de las colágenas pues ambas se tiñen de rosado con hematoxicilina-eosina. Pero la forma del núcleo en las fibras musculares es mucho más alargado que en los fibroblastos que pudieran estar presentes, además en un corte transversal las fibras musculares presentan microvacuoiización. En caso de duda en el tipo de célula de la tumoración puede realizarse una tinción con azul de anilina donde las fibras colágenas se tiñen de azul y las musculares de rojo. La tinción de Masson tiñe las fibras musculares de rojo oscuro y las colágenas de verde (3).
Referencias ]]>
1. Gómez Orbaneja J. Dermatología. Edit. Aguilar. Madrid. 1976:516-517. [ Links ]
2. Lever WF and Schaumburg Lever G. Histopathology of the Skin. 6th edition. Ed. J. B. Lippincott Co. Philadelphia. 1983:658-659. [ Links ]
3. Albrecht S. Neoplasias and hyperplasias of neural and muscular origin. En: Fitzpatrick's Dermatology in General Medicine. Editors: Freedberg l.M, Eisen A.Z, Wolff K, Austen K.F, Golsmith L.A, KatzS.I, Fitzpatrick T.B. 5th Edition. McGraw-Hill, New York. 1999:1210-1212. [ Links ]
4. Rook A, Wilkinson D.S, Ebling F.J.G. Textbook of Dermatology. Erd Edition. Blackwell Scientific Publication. Oxford. 1979:2228-2229. [ Links ]
5. Moschella S.L, Hurley H.J. Dermatology. 2nd Edit. W.B. Saunders Co. Philadelphia. 1985:1619-1620. [ Links ]
]]>
* Unidad de Microscopia Electrónica.
Universidad de Costa Rica. CP-2060, San José, Costa Rica.
Teléfono: (506) 207-3207. Fax: (506) 207-3182.
Correo electrónico: efreer@cariari.ucrac.cr