Caso clínico
Reparación endovascular de coartación de aorta con parada cardíaca inducida con adenosina
Endovascular Repair of Aortic Coarctation with Adenosine Induced Cardiac Arrest ]]>
Ignacio José Rivera-Chavarría, Michael Abarca-Brenes, José David Brenes-Gutiérrez y Juan Carlos Alvarado-Marín
*Dirección para correspondencia:
Resumen
La coartación de aorta es un estrechamiento congénito de la luz aórtica que, generalmente, afecta la porción torácica distal a la emergencia de la arteria subclavia izquierda. Esta condición es de gran importancia, pues predispone al desarrollo de patologías cardiovasculares a edades tempranas, lo que se traduce en una alta morbimortalidad. Se reporta el primer caso en Costa Rica, de reparación endovascular de una coartación de aorta, mediante la colocación de un stent recubierto, con parada cardiaca inducida con adenosina. La paciente toleró el procedimiento bien y el gradiente postintervención fue menor de 5 mmHg. Su presión arterial sistémica es 100/60mmHg y no tiene limitaciones o sintomatología.
Descriptores: coartación de aorta, terapia endovascular, parada cardíaca, stent recubierto, adenosina
Abstract
Aortic coarctation is a congenital narrowing of the aortic lumen that generally occurs distally from the origin of the left subclavian artery. It is of great importance because it predisposes to cardiovascular conditions at an early age, resulting in high morbidity and mortality. We report the first case in
La coartación de aorta (CoA) se define como el estrechamiento del lumen aórtico que suele afectar la aorta torácica descendente, generalmente distal a la subclavia izquierda.1 La CoA se puede asociar a diferentes condiciones, tales como: válvula aórtica bicúspide, arco aórtico hipoplásico, y aberrancia de los vasos de cuello.
La disminución del lumen aórtico produce un aumento de la postcarga del ventrículo izquierdo, alteraciones en el flujo de la aorta torácica y disminución en el flujo sanguíneo de la parte inferior del cuerpo.2
La incidencia es de 4 por cada 10000 nacimientos y corresponde a un 5-8% de todos los nacimientos de niños con enfermedades cardíacas.2 Usualmente, el diagnóstico se realiza durante la infancia, sin embargo, su diagnóstico puede ser tardío.3 La CoA no tratada tiene un pobre pronóstico en la mayoría de los pacientes, asociando morbilidades como hipertensión arterial, hipertrofia ventricular izquierda, valvulopatía mitral, estenosis subaórtica, muerte prematura, falla cardíaca, eventos cerebro-vasculares y enfermedad arterial coronaria prematura.4 El tratamiento usual de esta condición fue siempre la cirugía, al principio mediante la resección del segmento estenótico y la reanastaomosis aórtica,5 y posteriormente, utilizando colgajos arteriales o parches biológicos o sintéticos, para aumentar el lumen.6
Paciente femenina de 28 años, costarricense, de Cartago. Hipertensa, de 10 años de evolución, en tratamiento con Irbesartán 150 mg c/12horas. Fue referida al Hospital Dr. R. Á. Calderón Guardia, por CoA ductal, diagnosticada en mayo de 2013, por angioresonancia. Sin ningún otro antecedente significativo.
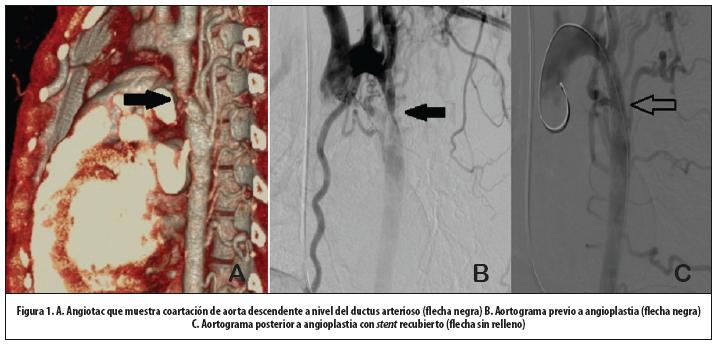
Un angiotac torácico evidenció la CoA y abundante circulación colateral (Figura 1A). El ecocardiograma mostró un ventrículo izquierdo hipertrófico con una fracción de eyección del 68%, sin otras anomalías, y una CoA a nivel del remanente del ductus arterioso, con diámetro mínimo de 3mm; la aorta postcoartación era hipoplásica y medía 1,2cm, con importante circulación colateral.
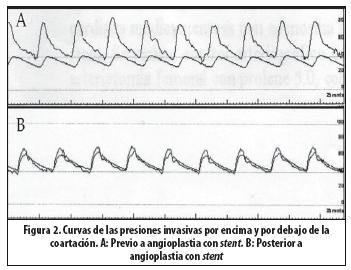
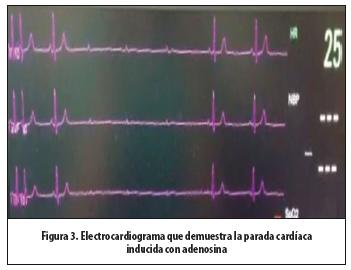
Previa obtención del consentimiento informado, explicando a la paciente las posibles complicaciones y riesgos del procedimiento, y con equipo quirúrgico preparado ante cualquier complicación, en sala de hemodinamia, bajo anestesia general, se le colocó un marcapaso transvenoso. Se accedió la arteria braquial izquierda y se expusieron los vasos inguinales derechos. Se hizo un aortograma por catéter desde el arco aórtico (Figura 1B). Se midieron las presiones por encima y por debajo de la coartación, obteniéndose un gradiente de 40mmHg (Figura 2A). Se introduce un stent recubierto de politetrafluoroetileno balón expandible (ADVANTA V12®)12X41mm, el cual se colocó en la posición deseada y luego se indujo la parada cardíaca con adenosina (bolo intravenoso de 60 mg de adenosina por vía central), que se logra por un tiempo aproximado de 6 segundos (Figura 3), durante el cual se libera el stent. La paciente recupera espontáneamente el ritmo sinusal. El control arteriográfico muestra un excelente resultado (Figura
La paciente es egresada 2 días después de la intervención, sin ninguna molestia.
Discusión
La reparación quirúrgica de la CoA fue descrita inicialmente en 1944, desarrollándose diferentes técnicas, dependiendo del tipo anatómico. Estas incluían: resección con anastomosis termino-terminal, reparación con parche, bypass con prótesis, entre otras.5-7 La cirugía sigue siendo el tratamiento de elección en infantes.8
El manejo actual endovascular de la patología aórtica torácica, ha disminuido la mortalidad del 40% al 14%.9 La angioplastia con balón ha sido aceptada en las 3 últimas décadas, como tratamiento de la CoA. Esta técnica es satisfactoria en casos de recoartación, después de la reparación quirúrgica en infantes, pero su uso en coartaciones nativas en todas las edades, es controversial, debido a la disrupción de la íntima y media de la pared de la aorta ocasionada durante el procedimiento, y a que tiene una alta predisposición de formación de aneurismas y persistencia de la lesión. Lo anterior obedece a que la pared arterial de la aorta en la coartación es primariamente anormal, y la alteración en el flujo hace que con el tiempo la aorta se vuelva tortuosa, delgada, con necrosis quística de la media y calcificación, lo que puede predisponer la disección y formación de aneurismas con el riesgo de ruptura.10
La utilización de stent balón expandible en las coartaciones de aorta fue reportada por primera vez en 1996,11 y ha ganado popularidad desde la década de los noventa. El stent puede reforzar áreas de debilidad de la pared y promover la formación de neoíntima, disminuyendo la formación de aneurismas, al compararse con la reparación únicamente con balón.12
Existen indicaciones de implantación de stent recubierto en pacientes con CoA, entre las cuales se citan:13
CoA asociada con aneurismas o con cambios degenerativos en la pared de la aorta, que sugieran las presencia de aneurismas ascendentes o una aorta sumamente tortuosa.
Obstrucciones críticas o atrésicas
Edad mayor de 18 años
Aortitis, síndrome de Turner, síndrome de Williams
La mayor preocupación de la implantación de un stent recubierto en la aorta, es el riesgo de oclusiones de las ramas durante la implantación, especialmente la subclavia izquierda y la arteria espinal, lo que podría resultar en paraplejia. El stent puede migrar y producir oclusiones de arterias en otros sitios, como en las arterias renales o las mesentéricas.13
Debido a lo anterior, la implantación de los stents recubiertos debe realizarse con mucha precisión. Sin embargo, el gran flujo de la aorta torácica afecta la estabilidad y, por lo tanto, la exactitud al despliegue. Existen métodos para contrarrestar esta situación: hipotensión controlada, oclusión con balón proximal, fibrilación ventricular inducida y parada cardíaca con adenosina.14
La adenosina ha probado ser segura y simple de utilizar, con pocos efectos secundarios.15,16 Una dosis de 60-90 mg (1 mg/kg) induce una parada cardíaca de 20-30 segundos, tiempo suficiente para el despliegue del stent.16
Se concluye entonces que la reparación endovascular con stent recubierto balón expandible, es una buena opción terapéutica, rápida, efectiva, y con menor morbilidad que la cirugía convencional. El uso de adenosina para inducir la parada cardíaca en procedimientos endovasculares es un método sencillo y seguro.
Agradecimientos: a la Dra. Mayra Vanesa Vaca Rojas, quien fue la anestesióloga del caso, y al Dr. Víctor Hugo Monge Monge, por su colaboración durante el procedimiento.
Referencias
1. Budoff M, Shittu A, Roy S, Use of cardiovascular computed tomography in the diagnosis and management of coarctation of the aorta. J Thorac Cardiovasc Surg 2013; 146:229-32. [ Links ]
2. Jurcut R, Daraban A, Lorber A, Deleanu D, Amzulescu M, Zara C et al. Coarctation of the aorta in adults: what is the best treatment? Case report and literature review. J Med Life 2011; 4:189-195. [ Links ]
3. Thani K, Kaushal K, Barnard D, Copeland J, Prasad A. Coarctation of the thoracic aorta masquerading as bilateral aorto-iliac stenosis. J Cardiol Cases 2011;4:172-175. [ Links ]
4. Maldonado J, Henry T, Gutiérrez F. Congenital Thoracic Vascular Anomalies. Radiol Clin North Am 2010;48:85–115
5. Crafoord S. Congenital coarctation of the aorta and its surgical management. J thorac Cardivasc Surg, 1945 ; 14:347. [ Links ]
6. Induni E, Pucci J, Soto L, Alvarado M, Méndez E, Salazar C, et al. Corrección quirúrgica de la coartación de la aorta: experiencia quirúrgica durante 30 años en el Hospital México. Rev costarric cardiol 2000; 2: 11-14 . [ Links ]
7. Mettler B, Peeler B. Congenital Heart Disease Surgery in the Adult. Surg Clin North Am 2009; 89:1021–1032. [ Links ]
8. Bentham J, English K, Ballard G, Thomson J. Effect of Interventional Stent Treatment of Native and Recurrent Coarctation of Aorta on Blood Pressure. Am J Cardiol 2013; 111:731-736. [ Links ]
9. Baker B, Phil D. Perioperative Considerations and Anesthetic Management for Endovascular Procedures. Advances in Anesthesia 2008; 26:137-156
10. Tanous D, Collins N, Dehghani P, Benson L, Horlick E. Covered stents in the management of coarctation of the aorta in the adult: Initial results and 1-year angiographic and hemodynamic follow–up. Int J Cardiol 2010; 140:287-295. [ Links ]
11. Ringel R, Gauvreau K, Moses H, Jenkins K. Coarctation of the Aorta Stent Trial (COAST) Study design and rationale. Am Heart J 2012; 164:7-13. [ Links ]
12. Forbes T, Kim D, Du W, Turner D, Holzer R, Amin Z, et al. Comparison of Surgical, Stent, and Balloon Angioplasty Treatment of Native Coarctation of the Aorta. J Am Coll Cardiol 2011; 58:2664–74. [ Links ]
13. Aboulhosn J, Levi D, Child J. Common Congenital Heart Disorders in Adults: Percutaneous Therapeutic Procedures. Curr Probl Cardiol 2011; 36:263-284. [ Links ]
14. Bruckheimer E, Cardoso C. Stenting Options for Coarctation of the Aorta. Intervent Cardiol Clin 2013; 2:115-129. [ Links ]
15. Fang T, Lippmann M, Kakazu C, Donayre C, Bui H, Kopchok G et al. High-Dose Adenosine-Induced Asystole Assisting Accurate Deployment of Thoracic Stent Grafts in Conscious Patients. Ann Vasc Surg 2008; 22:602-607. [ Links ]
16. Qu L, Raithel D. Techniques for precise thoracic endograft placement. J Vasc Surg 2009; 49:1069-72. [ Links ]
*Correspondencia a:
Afiliación de los autores: Sevicio de Vascular Periférico, Hospital Dr. Rafael Ángel Calderón Guardia, Caja Costarricense de Seguro Social, San José, Costa Rica *riveraignacio@hotmail.com
Fecha recibido: 06 de enero de 2014 Fecha aceptado: 15 de mayo de 2014
{kind=link}
{kind=link}
{kind=link}