(Sensitivity and Specificity of Treadmill Test and Myocardial Perfusion Imaging with SESTAMIBI in the detection of Coronary Artery Disease at the Hospital San Juan de Dios)
Juan Pablo Solís-Barquero, Jaime Tortós-Guzmán
Abreviaturas: CP, coronariopatía; estudio de perfusión miocárdica con SESTAMIBI, EPM-SESTAMIBI; FC max, frecuencia cardiaca máxima; HSJD, Hospital San Juan de Dios; DM, diabetes mellitus; HTA, hipertensión arterial; CLOBI, Comité Local de Bioética; DE, desviación estándar; ADA, arteria descendente anterior; ACD, arteria coronaria derecha;ACX, arteria circumfleja.
Correspondencia:
Apartado postal: San Pedro, 201-2050
Objetivo: La coronariopatía arterio esclerótica continúa siendo la principal causa de mortalidad mundial y Costa Rica no escapa a esta realidad. La prueba de esfuerzo, la imagen de perfusión con SESTAMIBI y la angiografía coronaria son métodos que permiten detectar esta entidad. El país no cuenta con datos sobre la información que proporcionan estas pruebas. El objetivo del estudio es determinar la rentabilidad diagnóstica de cada una de ellas.
Métodos:Es un estudio observacional, analítico de cohorte. Se incluyeron pacientes con factores de riesgo cardiovascular, que tuvieran prueba de esfuerzo, estudio de perfusión miocárdica y angiografía coronaria realizadas en el Hospital San Juan de Dios, desde 2003 a 2007. Se calculó la sensibilidad y especificidad de estos estudios. También se llevó a cabo un análisis con una estadística descriptiva de las características de la muestra y de los diferentes factores de riesgo cardiovascular.
Resultados: Se incluyeron 83 pacientes en el estudio, 75% hombres. Los principales factores de riesgo encontrados fueron dislipidemia (84%) e hipertensión arterial (70%). La prueba de esfuerzo tuvo una sensibilidad del 40% y una especificidad del 57%; el estudio de perfusión miocárdica con SESTAMIBI tuvo una sensibilidad del 66% y una especificidad del 71%. La mayoría de los pacientes tuvieron afección de uno o dos vasos coronarios, con lesiones mayores al 90%, y especialmente en la arteria descendente anterior.
Conclusión: Los factores de riesgo convencionales se presentaron en un alto porcentaje de la población estudiada. La prueba de esfuerzo mostró una baja sensibilidad y especificidad, sin embargo, coincide con el rango descrito en la literatura. El estudio de perfusión miocárdica con SESTAMIBI mostró un rendimiento diagnóstico significativamente superior (p =0.05).
Descriptores: coronariopatía, prueba de esfuerzo, imagen de perfusión miocárdica, SESTAMIBI, angiografía coronaria.
]]>
Abstract
Aim: Coronary artery disease is the first cause of mortality around the world, and Costa Rica does not escape from this reality. The treadmill test, myocardial perfusion imaging with SESTAMIBI, and coronary angiography are methods for detecting this disease. Our country does not have its own data regarding these tests. The aim of this study is to determine the diagnostic performance of each one. Methods: The present is an observational, analytic, cohort study. Patients included were those with cardiovascular risk factors that underwent a treadmill test, myocardial perfusion imaging, and a coronary angiography at the Hospital San Juan de Dios, from 2003 to 2007. Sensitivity and specificity were calculated. Adescriptive statistic analysis of the different risk factors was carried out.
Results: Eighty three patients were included in the study; 75% men and 25% women. The most frequently found risk factors were dyslipidemia (84%), and hypertension (70%). The treadmill test had a sensitivity of 40%, and specificity of 57%. Myocardial perfusion imaging with SESTAMIBI had a sensitivity of 66% and specificity of 71%. The majority of the patients had lesions in 1 or 2 coronary arteries, with more than 90% obstruction, mostly in the anterior artery descending.
Conclusion: A high prevalence of conventional risk factors was present in this population. The treadmill test showed a low sensitivity and specificity, according with the literature. The myocardial perfusion imaging had a significant (p =0.05) better diagnostic performance than the treadmill test.
]]> Keywords: coronary artery disease, exercise test, myocardial perfusion imaging, Technetium Tc 99m Sestamibi, coronary angiography
Según datos del Centro Nacional de Estadísticas en Salud y de la Asociación Americana del Corazón, las enfermedades del corazón afectan a más de 71 millones de estadounidenses, y causan más del 30% de muertes en los Estados Unidos.4,5 En Costa Rica, los reportes epidemiológicos apuntan a las enfermedades de origen cardiovascular como la primera causa de mortalidad, con una tasa de 11/10,000 habitantes para 2006.6
La estimación de la probabilidad de tener CP se debe enfocar en la presencia de factores de riesgo.3 Existen algunas escalas, como la de Framingham, que permiten determinar el riesgo individual para un paciente, de tener un evento coronario mayor, o muerte, en los próximos 10 años.7
En el país se cuenta con métodos de diagnóstico y evaluación para la CP, entre ellos la prueba de esfuerzo, los estudios de perfusión miocárdica con SESTAMIBI (EPM-SESTAMIBI) con esfuerzo físico o farmacológico, y la angiografía coronaria.8-10 La prueba de esfuerzo presenta una sensibilidad y una especificidad muy variable, que dependen del sexo del paciente, la edad, la cantidad de vasos coronarios afectados, la frecuencia cardiaca máxima alcanzada (FC max) durante el estudio, la probabilidad de tener CP y la experiencia del clínico que realiza la prueba.3 El EPM- SESTAMIBI es un estudio de medicina nuclear realizado en 2 etapas: reposo y ejercicio, y tiene la capacidad de diferenciar si los defectos de perfusión son por necrosis isquémica antigua (“cicatriz”) o por isquemia miocárdica actual.11 Otra indicación que tiene este estudio es para la estratificación de riesgo en los servicios de emergencias médicas, donde se ha visto que mejora la clasificación entre los pacientes de alto y de bajo riesgo.12 La angiografía coronaria se utiliza para establecer el diagnóstico definitivo de CP y se sigue considerando el “estándar de oro”. 3, 9,13 Debido a que no se tienen en el país datos predictivos sobre estas pruebas, se analizó la rentabilidad diagnóstica (sensibilidad, especificidad) de la prueba de esfuerzo y el EPM-SESTAMIBI en comparación con la angiografía coronaria; caracterizando además, los factores de riesgo cardiovascular de la población del estudio.
]]>
Métodos
Se trata de un estudio observacional, analítico de cohorte. La población que se estudió fue los adultos, mayores de 18 años, correspondientes al área de atracción del Hospital San Juan de Dios (HSJD) de San José, Costa Rica, que tuvieran factores de riesgo cardiovascular y sospecha o presencia de CP, que se hubieran realizado una prueba de esfuerzo, un EPM-SESTAMIBI y una angiografía coronaria en este centro, durante el periodo comprendido entre el 10 de enero de 2003 y el 31 de diciembre de 2007.
La fuente primaria de la información estuvo constituida por los expedientes clínicos en papel o microfilmados, del archivo del HSJD. Se diseñó una hoja especial para recolectar los datos. A cada paciente se le identificó con un número consecutivo y su número de cédula. Se recogió la información de las siguientes variables: edad, sexo, presencia de los siguientes factores de riesgo cardiovascular: diabetes mellitus (DM), hipertensión arterial (HTA), tabaquismo, sedentarismo, obesidad, dislipidemia e historia familiar de cardiopatía; además, el valor de la presión arterial, el perfil de lípidos y el motivo de solicitud de los estudios. Finalmente, se tomó el reporte de la prueba de esfuerzo como: positiva por isquemia, negativa o indeterminada, con la FC max; el reporte del EPM-SESTAMIBI como: positivo (por isquemia o cicatriz) o negativo; y la angiografía coronaria como: positiva por CP o negativa, con la cantidad de vasos epicárdicos afectados y el porcentaje de obstrucción.
Se analizaron los datos con el paquete estadístico SPSS, versión 8.0. Se confeccionaron tablas de 2 por 2 para calcular la sensibilidad y especificidad de la prueba de esfuerzo y el EPM-SESTAMIBI, corriendo además una regresión logística para determinar la significancia estadística. También se llevó a cabo un análisis de estadística descriptiva, con medidas de posición (moda, mediana) y medidas de dispersión (desviación estándar, valores mínimos y máximos) para cada una de las variables de los factores de riesgo.
La investigación se sometió a los principios de autonomía, justicia, beneficencia y no maleficencia, siendo aprobada por el Comité Local de Bioética (CLOBI) del HSJD, con el número CLOBI-HSJD-038-2008.
Se trata de un estudio observacional, analítico de cohorte. La población que se estudió fue los adultos, mayores de 18 años, correspondientes al área de atracción del Hospital San Juan de Dios (HSJD) de San José, Costa Rica, que tuvieran factores de riesgo cardiovascular y sospecha o presencia de CP, que se hubieran realizado una prueba de esfuerzo, un EPM-SESTAMIBI y una angiografía coronaria en este centro, durante el periodo comprendido entre el 10 de enero de 2003 y el 31 de diciembre de 2007.
La fuente primaria de la información estuvo constituida por los expedientes clínicos en papel o microfilmados, del archivo del HSJD. Se diseñó una hoja especial para recolectar los datos. A cada paciente se le identificó con un número consecutivo y su número de cédula. Se recogió la información de las siguientes variables: edad, sexo, presencia de los siguientes factores de riesgo cardiovascular: diabetes mellitus (DM), hipertensión arterial (HTA), tabaquismo, sedentarismo, obesidad, dislipidemia e historia familiar de cardiopatía; además, el valor de la presión arterial, el perfil de lípidos y el motivo de solicitud de los estudios. Finalmente, se tomó el reporte de la prueba de esfuerzo como: positiva por isquemia, negativa o indeterminada, con la FC max; el reporte del EPM-SESTAMIBI como: positivo (por isquemia o cicatriz) o negativo; y la angiografía coronaria como: positiva por CP o negativa, con la cantidad de vasos epicárdicos afectados y el porcentaje de obstrucción.
Se analizaron los datos con el paquete estadístico SPSS, versión 8.0. Se confeccionaron tablas de 2 por 2 para calcular la sensibilidad y especificidad de la prueba de esfuerzo y el EPM-SESTAMIBI, corriendo además una regresión logística para determinar la significancia estadística. También se llevó a cabo un análisis de estadística descriptiva, con medidas de posición (moda, mediana) y medidas de dispersión (desviación estándar, valores mínimos y máximos) para cada una de las variables de los factores de riesgo.
La investigación se sometió a los principios de autonomía, justicia, beneficencia y no maleficencia, siendo aprobada por el Comité Local de Bioética (CLOBI) del HSJD, con el número CLOBI-HSJD-038-2008.
]]>
Resultados
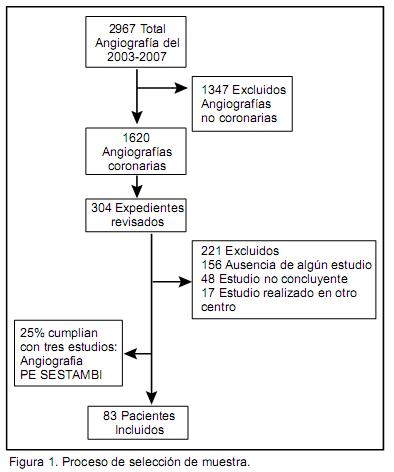
De 2967 angiografías realizadas en el HSJD, se excluyeron 1347, que correspondían a estudios en otros territorios (cerebro, vasos carotídeos, pulmón, aorta, vasos ilíacos y miembros inferiores). Las restantes 1620 fueron las angiografías coronarias. El tamaño de la muestra calculado con un nivel de confianza de 0.95, una varianza de 0.2 y un error máximo de 0.05, fue de 214 pacientes con un ajuste poblacional. Según los cuadros aleatorios, se seleccionaron y se revisaron 304 expedientes, para tener un margen de 90 pacientes más. Aunque se revisó esta cantidad de expedientes, 221 no cumplían con todos los criterios de inclusión del estudio y la muestra final fue de 83 pacientes, que correspondían al 25% de los expedientes revisados. (Figura 1)
De los pacientes incluidos en el estudio 62 (75%) fueron hombres y 21 (25%) fueron mujeres. El promedio de edad de los participantes fue de 61 años, con una moda en 58 años; la edad mínima fue de 35 años y la máxima de 85.
Resultados
De 2967 angiografías realizadas en el HSJD, se excluyeron 1347, que correspondían a estudios en otros territorios (cerebro, vasos carotídeos, pulmón, aorta, vasos ilíacos y miembros inferiores). Las restantes 1620 fueron las angiografías coronarias. El tamaño de la muestra calculado con un nivel de confianza de 0.95, una varianza de 0.2 y un error máximo de 0.05, fue de 214 pacientes con un ajuste poblacional. Según los cuadros aleatorios, se seleccionaron y se revisaron 304 expedientes, para tener un margen de 90 pacientes más. Aunque se revisó esta cantidad de expedientes, 221 no cumplían con todos los criterios de inclusión del estudio y la muestra final fue de 83 pacientes, que correspondían al 25% de los expedientes revisados. (Figura 1)
De los pacientes incluidos en el estudio 62 (75%) fueron hombres y 21 (25%) fueron mujeres. El promedio de edad de los participantes fue de 61 años, con una moda en 58 años; la edad mínima fue de 35 años y la máxima de 85.
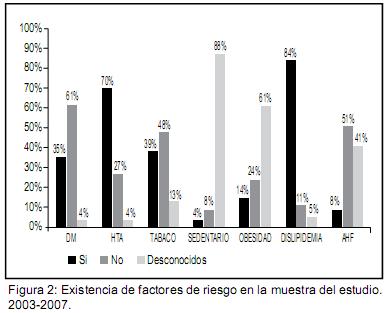
Los factores de riesgo encontrados en el estudio, aparte del sexo masculino y la edad mayor de 65, fueron: DM, HTA, tabaquismo, sedentarismo, obesidad, dislipidemia e historia familiar de cardiopatía. Como lo muestra la Figura 2, los principales factores de riesgo presentes en esta población fueron la dislipidemia en el 84% y la HTA en el 70%, con una frecuencia de DM del 35% y de tabaquismo del 39%. Se desconocía la frecuencia de sedentarismo en un 88%, de obesidad en un 61,5% y de antecedentes familiares en un 41%.
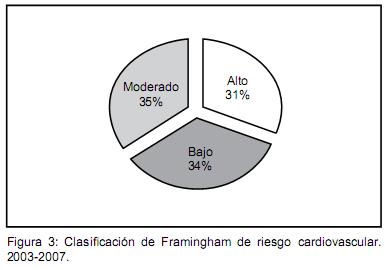
Según la clasificación de Framingham, aproximadamente una tercera parte de los individuos correspondían a pacientes de bajo riesgo, otra tercera parte a moderado riesgo, y una última parte a pacientes con alto riesgo. (Figura 3)
La prueba de esfuerzo demostró una sensibilidad del 40% y una especificidad del 57%. El promedio de FC max fue del 88%.
El EPM-SESTAMIBI demostró una sensibilidad del 66% y una especificidad del 71%. Reveló la presencia de cicatriz miocárdica en el 46%, de isquemia en el 32.5%, y defectos mixtos en el 21.5%.
El análisis de regresión logística determinó diferencias significativas entre el EPM-SESTAMIBI y la prueba de esfuerzo (p =0.05).
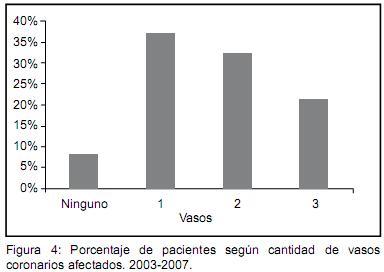
Según la cantidad de vasos afectados por la angiografía coronaria, se encontró que la mayoría de los pacientes presentaban enfermedad de uno o dos vasos, en el 37% y 33%, respectivamente. El otro 22% tenía afección de 3 vasos coronarios. (Figura 4)
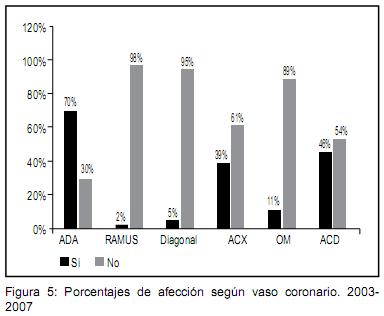
La Figura 5 demuestra el porcentaje de afección de los vasos coronarios, siendo la arteria descendente anterior (ADA) la más afectada en la muestra de este estudio, encontrándose en un 70% de los casos, seguida por la arteria coronaria derecha (ACD) en el 46%, y la arteria circumfleja (ACX) en el 39%.
]]>