Diagnóstico serológico de la Hepatitis B
Serologic diagnostic of Hepatitis type B
Zaida García-Solano*+
Descriptores: HBsAg, HBeAg, anticore, prevalencia, marcadores serolόgicos.
Abstract: The hepatitis B surface antigen (HBsAg), the hepatitis B core antigen (HBcAg), the hepatitis B e antigen (HBeAg) and its antibodies such as the anti-HBs, the anticore (HBcAb), the IG M anticore (HBcAb Ig M), the total anticore; and the anti HBe (HBeAb) are found to be the most important among several serological markers for hepatitis B virus. The seroprevalence of hepatitis B virus was measured based on the presence of surface antigen. Any country is considered highly prevalent if the levels of the population under study are higher than 8%. The prevalence is considered intermediate if levels are between 2 and 8%; and it is low if they are less than 2%. The Caja Costarricense de Seguro Social relies on a network of 98 laboratories each with the necessary equipment to find out the antigens and antibodies of hepatitis B virus. A study carried out in 2005 determined a surface antigen seroprevalence of 0.1% in all the country. Therefore,
Key Words: CAP, College of American Pathologists.
El HBV tiene un genoma de ADN parcialmente de doble banda de 3.2 kb, el cual consiste, en una hebra negativa completa y una positiva incompleta. Posee una envoltura lipídica rica en una proteína viral llamada antígeno de superficie o proteína S de
Este virus, en los individuos infectados puede producir hepatitis aguda y crónica. Aproximadamente, el 90% de la hepatitis B agudas, son clínicamente silenciosas, especialmente cuando la infección es adquirida en etapas tempranas de la vida. La probabilidad de la progresión a la cronicidad depende de la edad del paciente, del sexo y del estado inmunológico del individuo afectado. Sus vías de transmisión son la parental por el uso de jeringas infectadas al inyectarse drogas, por un pinchazo accidental por una jeringa contaminada, sexual; perinatal; por transfusión; trasplante renal; hemodiálisis y por contacto intrafamiliar y mediante utensilios contaminados con sangre (peines, cuchillas de afeitar, toallas y otros). La esperma, la saliva, la sangre, las secreciones cervicales y vaginales, la orina y la leche materna son fuentes de infección. El HBV se distribuye a nivel mundial y su prevalencia varía geográficamente y epidemiológicamente. Las zonas de alto riesgo son aquellas donde la prevalencia de HBsAg supera el 8%, de riesgo intermedio, cuando la prevalencia de este marcador está entre un 2 y un 8% y de bajo riesgo, cuando la prevalencia es menor al 2%. Estudios seroepidemiológicos realizados en Costa Rica, en las áreas de San Carlos, Pérez Zeledón, San Vito de Coto Brus, San Ramón- Palmares y en donantes de sangre en todo el territorio (para el año 2005 una seropositividad de 0.1% del HBsAg) han demostrado, que en Costa Rica, se clasifica como región de baja endemicidad, sin embargo, la zona de Pérez Zeledón se clasifica como prevalencia intermedia. Las consecuencias de la infección por el HBV van desde una leve incapacidad de la persona infectada, hasta la incapacidad permanente y consecuente muerte por hepatitis fulminante, cirrosis hepática o hepatocarcinoma celular primario (HCCP).
Pruebas para el diagnóstico en laboratorio
En un primer contacto con el virus surgen los síntomas asociados, y se producen en el plasma humano antígeno y anticuerpos únicos que hacen no sólo posible el diagnóstico del tipo de hepatitis sino también, determinan el estado de infección y el probable pronóstico. El diagnóstico se basa en la determinación, a partir de suero o plasma, de diferentes marcadores serológicos y virológicos que correlacionan con la enfermedad en sus diferentes estadios. Actualmente, se recurre no solo a las pruebas convencionales sino también, a métodos moleculares para su diagnóstico y control.
Las pruebas para la determinación de marcadores, en el diagnóstico de la hepatitis, han obtenido un gran desarrollo y optimización desde su desarrollo inicial. Las mejoras están desde la fuente y purificación de las proteínas antigénicas empleadas como los anticuerpos y principios técnicos en que fundamentan las pruebas.
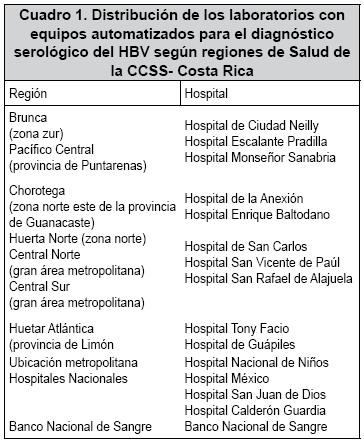
Además, coadyuva a lo anterior, el advenimiento global, en el desarrollo de sistemas automatizados, que han permitido el seguimiento de la trazabilidad total de las muestras, disminuyendo, sustancialmente, el consumo de recursos en término de costos y cargas de trabajo. CCSS cuenta con una red de 98 laboratorios, 29 son hospitales, 17 de los cuales están dotados de equipos analizadores para la realización de los exámenes serológicos para el diagnóstico de la hepatitis por virus B, los cuales funcionan en una red de referencia y contrareferencia.
Para la presentación de la distribución geográfica de los laboratorios que realizan la serología por HBV, se presenta la división por regiones de la CCSS, distribuidas de acuerdo al cuadro 1.
La CCSS, desde el inicio del año 2000, hasta los que llevamos del 2006, en cuanto a licitaciones realizadas, a nivel central, han invertido solo en el diagnóstico de la infección por el VHB un total de $1.905.423.38 millones para un total de 1.110.100 pruebas distribuidas entre HBsAg, IgM core, Anti core total, HBe Ag, anti HBe dando cobertura a todo el territorio nacional.
Marcadores serológicos (cuadro 4)
Cuando un paciente se presenta con síntomas o antecedentes que sugieren una hepatitis viral, después de un periodo de incubación, que puede durar hasta 10 semanas, se desarrolla la infección aguda con síntomas o no, resolviéndose o continua en cronicidad.
Se debe estudiar en la sangre de una individuo expuesto al virus, la presencia o no de antígenos virales como: el HBsAg y el antígeno “e” HBeAg.
El HBsAg es el primer marcador serológico que se detecta. Aparece semanas o meses (1 a 6 meses) luego de la exposición al virus. Su título llega a un pico en varias semanas, persiste durante un periodo variable, disminuye y desaparece con la recuperación clínica.
El HBsAg está presente durante la fase aguda de la infección en paralelo o a los pocos días aparece el antígeno, que indica un estado altamente infeccioso, por la replicación activa del virus donde el ADN del HBV esta circulando en la sangre y declina en parelelo con el HBsAg.
El diagnóstico del estadio de la enfermedad se completa por la evidencia de la lesión hepática con pruebas de laboratorio como transaminasas y anatomopatológicas.
También debe de valorarse la respuesta de anticuerpos específicos contra los antígenos HBsAg, HBeAg y HBcAg.
El primer anticuerpo en aparecer es el anti-HBc tipo IgM. La IgM va declinando y desaparece como a los seis meses, pero la IgM-anti-HBc persiste durante años.
Muy frecuentemente, los pacientes se presentan, tardíamente, durante el curso de la enfermedad, cuando el HBsAg ya ha desaparecido, la detección de IgM anti-HBc es el marcador serológico de mayor valor en una infección aguda por HBV.
El HBe Ag es reemplazado con el anticuerpo Anti-HBe, al comienzo de la recuperación clínica. Este anticuerpo, persiste 1-2 años tras desaparecer la infección aguda por hepatitis B.
Infección crónica por HBV se define con la persistencia del HBsAg, detectado en sangre, por un periodo mayor de 6 meses, producto de una incapacidad del individuo para eliminar el virus, este puede persistir por el resto de la vida del paciente o, en algunos casos, ser eliminado de forma espontánea. Aunque el 90-95% de los adultos con HBV se recuperan completamente, el virus puede dañar severamente el hígado y causar la muerte. El riesgo de desarrollar cronicidad por HBV depende en gran medida de la edad en que se infecta la persona. Cuando la infección ocurre por vía vertical o perinatal, el riesgo de cronicidad llega a valores hasta de un 90%.
Estos niños se convierten en replicadores activos del virus y por consiguiente, en diseminadores de la infección, en poblaciones infantiles además que también poseen un elevado riesgo de padecer afecciones del hígado y morir cuando llegan a ser adultos o jóvenes. Los niños que se infectaron por vía perinatal tienen un riesgo que va de 30 a un 60% de infectarse y de convertirse en portadores crónicos de HBV en los primeros 5 años de vida, por el contacto estrecho y continuo con las personas infectadas.
Niños de madres que son HBsAg y HBeAg positivos, el riesgo de transmisión perinatal es de
En la infección crónica, el antígeno HBsAg, persiste durante años o décadas. El título puede disminuir, un poco, a medida que pasan los años, pero se mantiene durante toda la vida. Se pueden detectar el antígeno HBeAg, anti HBe y el ADN del HBV en el suero de individuos infectados. Los pacientes con mutaciones en la proteína viral pre core/core mostrarán presencia de anti HBe y de viremia.
El ADN del HBV puede, eventualmente, integrarse al ADN del hepatocito, lo cual resulta ser importante en la aparición de carcinoma hapatocelular primario, la complicación más grave de esta enfermedad.
El anticuerpo anti-HBc (una IgG) esta invariablemente presente en el suero de los portadores; hay muy pocas IgM presente, los anticuerpos anti-HBc totales pueden detectarse, tanto en infección aguda, crónica, como en aquellos que ha resuelto una hepatitis B.
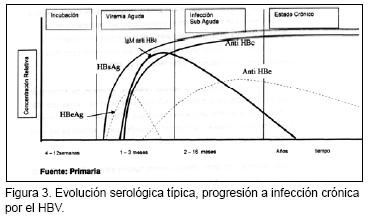
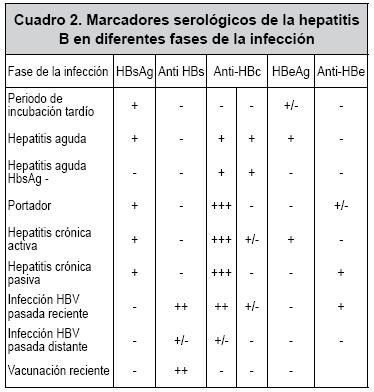
En la Figura 3 se ilustra una evolución serológica típica de una infección crónica por HBV y en el cuadro 2 se describe los marcadores serológicos en diferentes patrones de infección.
Control de un paciente con hepatitis B
Una vez que una infección con HBV ha sido confirmada por pruebas serológicas, es importante determinar el estado de la infección y el pronóstico, con el objeto de realizar el tratamiento apropiado e iniciar las medidas de control entre los contactos íntimos.
Las pruebas para los siguientes marcadores pueden ser utilizadas para controlar el proceso: HBsAg, Anti HBe y Anti-HBs. El control de la muestra original del paciente para HBeAg y Anti HBe ayudará a determinar el estado de la infección y qué tan infecciosa es la persona. Si la muestra original fue negativa, se debe controlar al paciente aproximadamente un mes después, realizando las pruebas para HBs Ag, Anti-HBc IgM, HBeAg con lo cual se llegará a igual fin.
Por otra parte, la persistencia de HbeAg y HBsAg durante
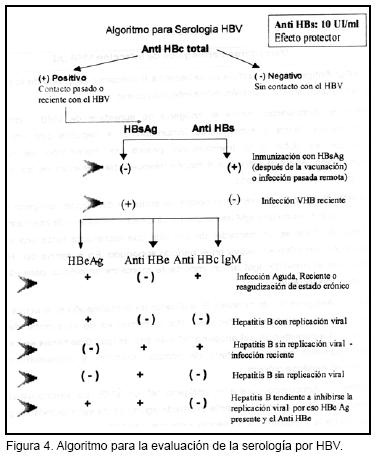
En el último caso, estos individuos, en su mayoría, no desarrollan una severa enfermedad hepática. Cuando un paciente se presenta con síntomas o antecedentes que sugieren una hepatitis aguda viral, las primeras pruebas apropiadas para una evaluación son el HBsAg, el Anti-HBc IgM, el Anti-HbC total.
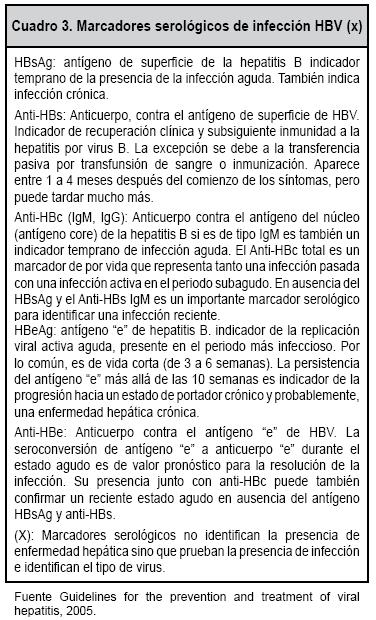
El cuadro 2 resume los cuadros típicos vistos con estas pruebas y sus interpretaciones clínicas. Cuadro 3, figura 4
Aguilera AG, Romero YS, Regueiro BJ. Epidemiología y manifestaciones clínicas de las hepatitis virales. Enferm Infec Microbiol Clin. 2006; 24:264-276. [ Links ]
Brezmes MF, Ochoa C, Eiros JM. Cost análisis in a clinical microbiology laboratory. Eur J Clin Microbiol Infect Dis 2002; 21:582-8. [ Links ]
Bruguera M, Forns X. Epidemiología actual de las hepatitis virales ¿Quién la padece y quien puede protegerse?.Enf Infecc Microbiol Clin 2004; 22:443-447. [ Links ]
Caja Costarricense de Seguro Social, Dirección técnica de servicios de salud-sección de laboratorios. Informe de Bancos de sangre año 2000-2001, 2002-2003, 2004-2005; San José Costa Rica; 2005. Serie de Informes Técnicos: 2000-2005. [ Links ]
Codoñer F.P. Hepatitis B, el virus, técnicas de diagnóstico epidemiología, enfermedad y sus posibilidades evolutivas. An Pediatr 2003;58:478-81. [ Links ]
Chein Fu H, Shih Shen L, Young Chyuan H et al. The immune response induced by hepatitis B virus principal antigens. Cell Mol Inmunol 2006; 3:97-106. [ Links ]
Delgado A, Echeverría JM, León P. Serología de la hepatitis víricas. 2° ed. En: Cercenado E, Cantón R. Procedimientos en microbiología clínica. Recomendaciones de la Sociedad Española de enfermedades infecciosas y microbiología clínica.
Guildelines for the Prevention and treatment of Viral Hepatitis. October 2005. Federal Bureau of Prisions. Clinical Practice Guildelines. 2005;1-70. [ Links ]
Holliger FB. 1996 Chapter 86: Hepatitis B fields Virology, ed B.N Fields, DM. Knipe PM. Holowey et al. Third edition. Lippincott- Raven Pubhlisher,
Jinlin H, Zhiua L, Fan G. Epidemiology and prevention of hepatitis B virus infection Review. Int J Med Sci 2005; 2: 50-58. [ Links ]
Kenneth WL, Kirchner JT. Hepatitis B. Am Fam Phys 2004; 69:75-82. [ Links ]
Khourime M, Aparecida V, Review Hepatitis B: Epidemiological, immunological and serological considerations emphasizing mutation. Rev Hosp Clin Fac Med
Khouri M. Hepatitis B epidemiology, inmunology and serology. Rev Hosp Clin Fac Med
Mahoney FJ. Update on diagnosis, management and prevention od Hepatitis B virus infection. Clin Microbiol Rev 1999; 12: 351-366. [ Links ]
Miller Rh, Kanicko S, Chung C. Compact organization of the hepatitis B virus genome. Hepatology 2006; 9:322-327. [ Links ]
Ortiz de Lejarazu R, Avellón Ana, Eiros JM. Diagnóstico microbiológico de las hepatitis víricas. Enf Infecc Microbiol Clin 2006; 24:194-2004. [ Links ]
Park W, Keefe EB. Diagnosis and treatment o chronic hepatitis BB. Minerva Gastr Enterol Dietol 2004; 50: 289-303. [ Links ]
Rakesh A, Piyush R, Preventing ant treating hepatitis B infection. BJM 2004; 329;1080-1086. [ Links ]
Salas O, Informe automatización de laboratorios a Junta Directiva CCSS. Departamento de regulación y Sistematización Área Laboratorios Clínicos, 2002. [ Links ]
Torres Al, Gar MZ. Revista Costarricense de Ciencias Médicas 2004; 25: 21-25. [ Links ]
Uchida T. Genetic cíavariations of the Hepatitis B virus and their clinical relavence. Microbiol Inmunol 1993;37:425-439. [ Links ]
Visoná KA, Eduarte CE, Zamora E, Salazar LM. Estudio epidemiológico de las hepatitis virales en San Ramón y Palmares de 1972-1985. Act Med Costarric.1998;33:69-77. [ Links ]
Zunino M. ENNA. Epidemiología de la Hepatitis B en Chile y esquemas de vacunación en Latinoamerica. Rev Chil Infecctol.2002;19:140-155. [ Links ]
*Microbióloga, Caja Costarricense de Seguro Social.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}