Resumen: La sarcoidosis es una enfermedad que se diagnostica con poca frecuencia en Costa Rica; en 1988 fueron informados 6 casos en el Hospital San Juan de Dios. En este estudio se da cuenta de las características clínicas y el manejo de 15 pacientes del Hospital Calderón Guardia, diagnosticados entre 1987 y 2001. Todos los casos fueron de localización torácica y en doce de ellos la enfermedad afectó solamente los ganglios del mediastino, por lo que la radiografía de tórax fue el método de detección . Los síntomas más frecuentes fueron tos y disnea. La mediastinoscopía fue el método más utilizado para obtener la biopsia. El diagnóstico histológico se hizo por el hallazgo de granulomas no necrotizantes, infiltrado linfocitario y la presencia de células gigantes, sin que se aislara ningún germen. Catorce pacientes recibieron tratamiento sintomático y observación y solo uno presentó afección pulmonar y sintomatología respiratoria y recibió esteroides. El paciente con enfermedad pulmonar sintomática continúa con esteroides y los pacientes observados, por un promedio de 7 años, evolucionaron a resolución espontánea sin producirse recidivas.
Descriptores: Sarcoidosis, tumores del mediastino, mediastinoscopía
Recibido: 06 de febrero del 2002. ]]>
Aceptado: 23 de abril del 2002.La sarcoidosis es una enfermedad multisistémica descrita por primera vez en 1877 por el médico inglés Jonathon Hutchinson 2-3. Su incidencia y prevalencia presentan variaciones considerables entre países y continentes, y a pesar de que estas posiblemente son reales, también se relacionan con la conciencia local e interés por la enfermedad. En 1988 Alvarado y Haryley informaron seis casos diagnosticados en Costa Rica 1.
Aunque su causa es aún desconocida, el hecho de que los órganos más comúnmente afectados son los pulmones y los módulos linfáticos mediastinales, sugiere que la enfermedad sea causada por un agente que se adquiere posiblemente por inhalación. Algunos microorganismos como Mycobacterium tuberculosis, Yersinia enterocolítica, Borrelia burgdorferi y Propionibacterium acnes, se han mencionado como posibles causas 2,4. Otros proponen que la enfermedad se desarrolla en individuos con predisposición genética, los cuales son expuestos a un antígeno que desencadena una reacción inflamatoria de tipo granulomatosa 5-6. Los hallazgos, tanto moleculares como histológicos, evidencian una respuesta inflamatoria e inmune a un estímulo antigénico. Se han observado cúmulos familiares de sarcoidosis, sin embargo, parece poco probable que un solo gen sea el responsable y es más posible que el factor genético que promueve susceptibilidad resida en loci que influencian la regulación inmune, la función de células T o la presentación y reconocimiento de antígenos 7-9.
Es más frecuente en mujeres 16 y se puede presentar a cualquier edad, pero es más común entre los 20 y 40 años 10-13. De acuerdo con el órgano afectado, presenta una amplia variedad de características clínicas y radiológicas. Los tejidos que se ven afectados con más frecuencia por esta enfermedad son los ganglios mediastinales y el pulmón (80% a 90% de los casos) 1. También puede involucrar el hígado, ojos, bazo, glándulas salivales, corazón, sistema nervioso, músculos, huesos y otros órganos, con menos frecuencia.
Histológicamente se describe una acumulación de linfocitos T, fagocitos mononucleares y, característicamente, es la presencia de granulomas no caseificantes asociados con células gigantes multinucleadas 21. Los ganglios linfáticos se ven reemplazados difusamente por granulomas de apariencia histológica variable, que se palpan duro elásticos y se encuentran mal delimitados. La mayoría de los granulomas en sarcoidosis no presentan necrosis sin embargo ésta se ha documentado en un 4% a un 38% de los casos 14, razón por la cual se ha relacionado con tuberculosis y sugerido, sin confirmarse, la posibilidad de una micobacteria atípica. Algunos pacientes que en el pasado se curaban de tuberculosis espontáneamente, bien pudieron ser portadores de esta enfermedad, pues se asocia con curación espontánea.
Cuando hay afección pulmonar, los granulomas son inicialmente discretos e histológicamente activos, pero conforme avanza la enfermedad, pasan a ser confluentes y se asocia fibrosis que produce engrosamiento intersticial difuso. Los granulomas se localizan en el tejido conectivo peribronquial, pero también afectan la mucosa de la vía aérea. Son más comunes en las vías aéreas pequeñas, aunque se pueden encontrar también en las paredes bronquiales.
Algunos granulomas se resuelven espontáneamente, pero otros sufren fibrosis. La apariencia de sarcoidosis pulmonar depende de la severidad y de la etapa en la cual se encuentra la patología. En etapas tempranas la inflamación granulomatosa es prominente en el nivel peribroncovascular, interlobular y en el tejido conectivo pleural, presentando cierto parecido a una carcinomatosis linfangítica. Conforme avanza la enfermedad, en el parénquima pulmonar se observan focos de fibrosis intersticial o nodular; siendo este proceso más severo en los lóbulos superiores 4,15.
En pacientes con sarcoidosis hay aumento del complejo mayor de histocompatibilidad clase II y de otras moléculas involucradas en la activación de células T. Debido a esto, la habilidad de los macrófagos alveolares para producir antígenos se encuentra aumentada 16. El macrófago alveolar es responsable del procesamiento y presentación del supuesto antígeno productor de sarcoidosis a las células inmunocompetentes, iniciando de esta manera la alveolitis linfocitaria característica de la enfermedad. El papel principal de dichas células es la iniciación de la respuesta inmune mediada por células T, que lleva a la formación de granulomas 9. La activación de macrófagos se caracteriza por acumulación de linfocitos alrededor de ellos y producción de citoquinas (IL-1, IL-2, IL-6 e IL-8, factor de necrosis tumoral a, proteína quimiotáctica monocitaria-1), glucoproteínas (CD14) y moléculas de adhesión. Dichas moléculas estimulan la migración y activación de linfocitos, leucocitos polimorfonucleares y fibroblastos, los cuales participan en la reacción inflamatoria y fibrosis característica 2. Los macrófagos se incorporan a los granulomas como histiocitos epiteliales y secretan T G F - ß1 (factor transformador de crecimiento), el cual modula la fibrosis del granuloma, debido a su acción antiinflamatoria.
Un 50% de los pacientes son asintomáticos y la enfermedad se detecta como hallazgo casual en una radiografía de tórax. La sintomatología es generalmente de inicio insidioso. Un 90% de los pacientes presenta síntomas respiratorios caracterizados por tos seca y disnea y sólo un 10% manifiestan síntomas referidos a otros órganos 2. Los más afectados son el corazón, la piel y los ojos 3. El agrandamiento de ganglios linfáticos mediastinales ocurre en el 75% al 90% de los casos, y la compresión del árbol respiratorio es causa de la disnea. La afección ocular se presenta en un 25% de los pacientes con uveítis anterior aguda o crónica 17. De un 20% a un 30% de los afectados presentan alteraciones dermatológicas inespecíficas como eritema nodoso y lupus pernio, que resuelven espontáneamente 18,19. Un 5% de los pacientes presenta evidencia clínica de afectación cardiaca 2 que puede ser directa como la miocarditis granulomatosa, o indirecta cuando se desarrolla de cor pulmonale secundario a fibrosis parenquimatosa 12. En un estudio de autopsias se informó que aproximadamente dos tercios de los pacientes presentan compromiso de hígado, bazo y riñón, que raramente produce sintomatología 20. Puede también afectar el cerebro, médula espinal, meninges, pares craneales y nervios periféricos 21. ]]>
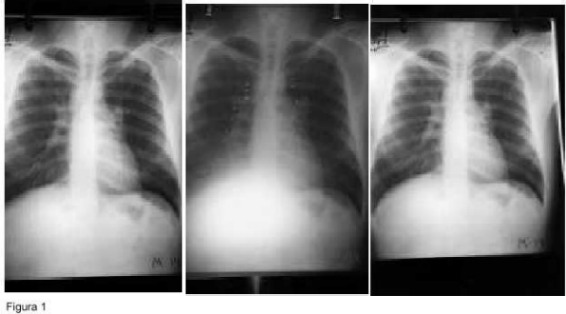
El mal estado general, pérdida de peso, fiebre, sudoración nocturna y fatiga, son manifestaciones sistémicas y son inespecíficas. Esta enfermedad se asocia con dos síndromes, el Síndrome de Lofgren que es la tríada de linfadenopatía hiliar bilateral, eritema nodoso y poliartralgias 22 y el Síndrome de Heerfordt Waldestrom con fiebre, parotiditis, uveítis anterior y parálisis facial. También se asocia con enfermedades del colágeno 4.Las alteraciones radiológicas en sarcoidosis torácica (ver figura 1) se clasifican según la clasificación propuesta por Wurm y colaboradores 25 en cuatro grupos:
Etapa I: Únicamente aumento de tamaño de los ganglios linfáticos mediastinales e hiliares.
Etapa II: Aumento de tamaño de ganglios linfáticos, asociado con anormalidades pulmonares
Etapa III: Enfermedad pulmonar difusa, no asociada con aumento de tamaño ganglionar
Etapa IV: Fibrosis pulmonar
Existe gran discordancia en cuanto al esquema de tratamiento. Los puntos debatibles son el momento de inicio, la duración y la dosificación. Como una regla general, los esteroides constituyen la droga de primera línea 18. Se utilizan de entrada en las siguientes situaciones: enfermedad ocular severa, sarcoidosis neurológica o cardiaca, hipercalcemia maligna, etapa II sintomática, etapa II en vías de progresión y etapa III 3. Los protocolos son de 30 a 40 mg de prednisona diarios por 8 a 12 semanas con disminución gradual a 10 a 20 mg por día, en un periodo de 6 a 12 meses, para establecer la mínima dosis efectiva 3. ]]>
La mayoría de los pacientes en estadio I y II suelen remitir espontáneamente, mientras que en estadios más avanzados es necesaria la inmunoterapia para lograr la remisión, y estos tienden a las recaídas 24. La mayoría de los pacientes que mueren es a causa de cor pulmonale secundario a fibrosis pulmonar o de una arritmia cardiaca secundaria a miocarditis granulomatosa 4.El objetivo de este estudio es informar la experiencia con la presentación clínica, métodos de diagnóstico, manejo y evolución de 15 casos de Sarcoidosis tratados en el Hospital Calderón Guardia y ofrecer una revisión bibliográfica para motivar a la comunidad médica en la detección de estos casos.
Materiales y Método
La población del estudio está constituida por quince pacientes diagnosticados de sarcoidosis en el Hospital Calderón Guardia, en el periodo comprendido entre enero de 1987 y julio del 2001. El criterio para hacer el diagnóstico se basó en el cuadro clínico, apoyado en todos los casos por una biopsia con el hallazgo histológico de granulomas sin necrosis, con presencia de infiltrado linfocitario, células gigantes y ausencia de microorganismos. Se recolectaron los datos clínicos mediante un instrumento de recolección que fue aplicado a los expedientes en cuestión. El estudio se realizó en forma retrospectiva, se trabajó con el universo entero y no se efectuó análisis estadístico, dado el tamaño reducido de la muestra.
Resultados
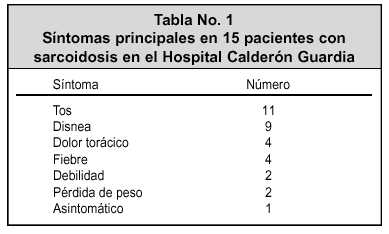
Se encontraron 8 pacientes femeninos y 7 masculinos, todos caucásicos. La edad osciló entre 17 y 55 años, con un promedio de 37 años. Nueve con antecedente de tabaquismo y 6 sin él. Ninguno refirió antecedente familiar de sarcoidosis, ni ser portadores de enfermedades del colágeno. En todos los casos la lesión se observó en la radiografía de tórax. El tiempo de evolución de los síntomas fue entre 1 mes y 18 meses, con una media de 5 meses. Los síntomas más frecuentes se muestran en la tabla No. 1. La biopsia se obtuvo en 11 pacientes por mediastinoscopia, en 3 por cielo abierto y en uno por vía transbronquial. No se encontró ningún caso de sarcoidosis extratorácica en los archivos de patología del hospital. Los pacientes fueron agrupados de acuerdo con los hallazgos radiológicos, correspondiendo doce a la etapa 1, dos a la etapa 2 y uno a la etapa 3
El tratamiento que se le dio a los pacientes consistió en: explicarles su enfermedad, medicación sintomática y observación en 14 casos, y en el paciente con infiltrado pulmonar difuso y sintomatología, esteroides. Salvo este último caso, que aún se encuentra en tratamiento, todos los pacientes han tenido remisión espontánea de las adenomegalias y se encuentran asintomáticos. El tiempo en que se ha observado va de 6 meses a 14 años, con un promedio de 7 años, período durante el cual no se ha presentado ninguna recidiva ni complicación relacionada.
]]>
Discusión
La sarcoidosis es una enfermedad poco frecuente en Costa Rica, sin embargo, podrían existir casos no diagnosticados, sobre todo en localizaciones donde tomar una biopsia resulta un proceso complejo.
Aunque en los países del norte la enfermedad se presenta con mayor frecuencia en pacientes de raza negra con una proporción de 3:1 26,27, en nuestra serie no se presentó en ninguno. De acuerdo con la bibliografía hay predilección por adultos menores de 40 años; en este caso el promedio fue de 37 años.
En 1940 casos de sarcoidosis en mujeres trabajadoras de la industria de fluorescentes en Salem, Massachussets, se reconoció la exposición al berilio como causante de "Sarcoidosis de Salem". La exposición a otros polvos de metal, gases y antígenos orgánicos, puede causar enfermedades pulmonares granulomatosas difíciles de distinguir clínicamente de la sarcoidosis 18,28 . Solo uno de los pacientes en este estudio es operario industrial, por lo que no existe de la enfermedad con riesgo el ocupacional.
A pesar de que en la bibliografía se informa que un 50% de pacientes son asintomáticos, lo que obedece posiblemente a la rutina de realizar estudios en pacientes sanos para tamizaje, en nuestra serie todos presentaron síntomas respiratorios, siendo la tos y la disnea los más frecuentes, y en ningún caso se encontraron síntomas extratorácicos. Al único paciente asintomático se le encontró una masa mediastinal en una radiografía de previo empleo.
La mediastinoscopía fue el método más utilizado para obtener la biopsia, ya que en la mayoría de los casos la enfermedad estaba localizada en los ganglios del mediastino. En este estudio el diagnóstico se hizo relacionando la clínica, los hallazgos histológicos y la evolución.
Los pacientes fueron agrupados en etapas, sin que se considerara ello una clasificación de estadio, ya que únicamente se aplican criterios radiológicos. Los pacientes clasificados en etapa I y II resolvieron espontáneamente, de acuerdo con lo citado en la bibliografía. El paciente en etapa III recibió Prednisona 50 mg por día, durante tres meses, 37.5 mg, durante día por diez meses, 12.5 mg en días alternos, durante un mes y 1 miligramo cada tercer día, durante un mes. El resto del grupo fue únicamente observado en su evolución.
]]>
Sarcoidosis is an infrequent disease in Costa Rica. In 1988 the Hospital San Juan de Dios reported six cases. This is a clinical study of 15 patients diagnosed at the Hospital Calderón Guardia from 1987 to 2001. All the patients presented with thoracic disease and in 12 of them it was localized to the mediastinal lymph nodes. A chest X-ray detected all the cases; cough and dispnea were the most frequent symptoms and mediastinoscopy was the most useful method to obtain a biopsy. The histologic diagnosis was made in the presence of non-necrotizing granulomas, giant cells and a lymphocytic infiltrate. No microorganisms were isolated. Fourteen patients received symptomatic treatment and observation, and one with pulmonary disease and respiratory symptoms received also steroids. All the patients were observed, for an average of 7 years. They presented spontaneous resolution without remissions.
Referencias
1. Alvarado A. Haryley L. Sarcoidosis. Acta Médica Costarricense 1988; 31(1):10-19. [ Links ]
2. Hillerdal G. et al. Statement on Sarcoidosis. Am J Resp Crit Care Med. 1999; 160: 735-755. [ Links ]
3. Newman L. Rose C. and Maier L. Sarcoidosis. N. Engl. J. Med. 1997; 336:1224-1232. [ Links ]
4. Fraser R. et al. Sarcoidosis. Diagnosis of Diseases of the Chest. Saunders, Pennsylvania, 1999. Págs. 1533-1573. [ Links ]
5. Rybicki B et al. Racial diffferences in sarcoidosis incidence: a 5 year study in a health maintenance organization. Am J Epidemiol 1997; 145:234-241. [ Links ]
6. Buck A. Epidemiologic investigations on sarcoidosis. Am J Hyg 1961; 74:189-202. [ Links ]
7. Konishi K. Molleer et al. Spontaneous expression of the IL2 receptor gene and presence of functional IL2 receptors on T lymphocytes in the blood of individuals with active pulmonary sarcoidosis. J Clin Invest 1988; 82:775-781. [ Links ]
8. Agostini C. et al. Role of IL15 and IL2 and their receptors in the development of T cell alveolitis in pulmonary sarcoidosis. J Inmunol 1996; 157: 910-918. [ Links ]
9. Gibson G. Prescott R. Muers M. et al. British Thoracic Society Sarcoidosis study: effects of long term corticosteroid treatment. Thorax 1996; 51:238-47. [ Links ]
10. Gordis L. Sarcoidosis: Epidemiology of Chronic Lung Diseases in Children. The John Hopkins University Press, Baltimore. 1973; 53-78. [ Links ]
11. English J. Patel P. Greer K. Sarcoidosis. J Am Acad Dermatol. 1999; 44 (5): 725-43. [ Links ]
12. Kwai K. Et al. Racial difference in cardiac sarcoidosis incidence observed at autopsy. Sarcoidosis 1994; 11:26-31. [ Links ]
13. Milman N. Selroos. Pulmonary sarcoidosis in the Nordic countries 1950-1982: epidemiology and clinical picture. Sarcoidosis 1990; 7:50-57. [ Links ]
14. Rosen Y. Sarcoidosis. In D. Dail and P. Hammer, editors. Pulmonary Pathology. Springer-Verlag, New York 1994; 13-645. [ Links ]
15. Colby T. Intersticial lung diseases. In W. Thurlbeck and A. Churg editors. Pathology of the Lund. Thieme Medical Publishers, New York 1995; 589-737. [ Links ]
16. Semenzato G. et al. Redistribution of T lymphocytes in the lymph nodes of patients with sarcoidosis. N Engl J Med 1982; 306:48-49. [ Links ]
17. Karma A. Ophthalmic changes in sarcoidosis. Acta Ophthalmol Suppl 1979; 141:1-94. [ Links ]
18. Wilson et al. Sarcoidosis. Harrison´s Principles of Internal Medicine. Mc Graw Hill, Estados Unidos. Págs. 1463-1469. [ Links ]
19. Sharma O. Cutaneous sarcoidosis: clinical features and management. Chest 1972; 61:320-325. [ Links ]
20. Maddrey W. et al. Sarcoidosis and chronic hepatic disease: a clinical and pathology study of 20 patients. Medicine 1970; 49:375-395. [ Links ]
21. Sharma O. Vitamin D, calcium, and sarcoidosis. Chest 1996; 109:525- 539. [ Links ]
22. Lofgren S. Erythema nodosum: studies on etiology and pathogenesis in 185 adult cases. Acta. Med. Scand. 1996; 124:1-197. [ Links ]
23. Alsbirck P. Epidemiologic studies on sarcoidosis in Denmark based on a nationwide central register: a preliminary report. Acta Med Scand 1964; 176:106-109. [ Links ]
24. Sharma O. Pulmonary sarcoidosis and corticosteroids. Am Rev Resp. Dis 1993; 147:598-600. [ Links ]
25. De Remee R. Concise Review for Prmary-Care Physicians. Sarcoidosis. Mayo Clin Proc 1995; 70:177-181 [ Links ]
26. Rybicki B. Maliarik M. Popovich J. Jr, et al: Epidemiology, demographics and genetics of sarcoidosis. Semin Respir Infect 1998; 13: 166. [ Links ]
27. Douglas J. Middleton J. Gaddie G. Petrie Y. Chookang R. Prescott and Crompton. 1986. Sarcoidosis: a disorder commoner in non-smokers? Thorax 1986; 41:787-791. [ Links ]
28. De Vuyst P. Dumortier L. Schandene M. Estenne A. Verhest and Yernault. Sarcoidlike lung granulomatosas induced by aluminum dusts. Am Rev Respir Dis 1987; 135:493-497. [ Links ]
1 Jefe Servicio Cirugía de Tórax. Profesor de Cirugía. Hospital Calderón Guardia,
2 Médico General, Universidad de Costa Rica
Correspondencia: José A. Mainieri Hidalgo. Apartado Postal: 1964-2100
Costa Rica. Correo electrónico: albertom@racsa.co.cr ]]>