











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Child abuse is a universal problem with critical lifelong effects. It is defined as a child being subjected to an adult's knowingly or unknowingly actions that are considered harmful, and that hinder or restrict the child's growth and development (1). Factors such as cultural structure, traditions, living conditions, educational level and economic status of families in the society constitute the basis for the emergence of this problem. It has been reported that physical and emotional abuse are mostly encountered due to patriarchal authority based child rearing, disciplining methods for children, and differences in perceptions of cultural violence in Turkey as well as in many other countries (2). According to the United Nations Convention on the Rights of the Child, every person under the age 18 is regarded as a child, unless a different legal age is defined by national laws. Every child has the right for a healthy life without violence (3). Nevertheless, many children are subjected to abuse worldwide. In recent years, social awareness on child abuse is on the rise. Studies in different countries have demonstrated the relevant knowledge, experien- ces, and attitudes of health professionals and in particular dentists about child abuse and the ways to be able to diagnose, report, and prevent child abuse have been suggested (4,5,6,7,8,9,10,11,12,13).
In diagnosing and reporting child abuse, dentists should play an important role. Actually, they are among the first to identify such cases, as the most common abuse findings are usually seen in areas of routine examination (14). Many studies report that primary areas of abuse are the face, head, neck and mouth circumference (15,16,17). These regions are thought to be subject to more abuse as they are vulnerable and accessible and also because the head represents the whole body (18). As dentists develop a regular interaction with children and their parents, they are also able to observe any abnormal patterns in child-parent behavior (19). Furthermore, abusive parents have been reported to change their doctors frequently, but continue with the same dentist (17,20).
Dentists are under the legal obligation to report cases of child abuse in many countries around the world (21), yet report rates are found to be low (4,5,6,7,8,9,10,11,22). All health-care professionals in accordance with Article 280 of the Turkish Penal Code and public servants in accordance with Article 279 of the Turkish Penal Code are obliged to report cases of child abuse, also in Turkey. However, the limited availability of the subject in dentistry undergraduate education, the small number of researches on the subject and the social and cultural characteristics of the society we live in affect dentists' reporting (23,24). The aims of this study are to evaluate the knowledge, attitudes, and experiences of dentists regarding child abuse and to increase relevant awareness of them.
Materials and Methods
Study sample and desing
Approval for the study was obtained from the Clinical Research Ethics Committee of the Faculty of Medicine, Suleyman Demirel University, Isparta, Turkey (decision no.129). The study has been conducted in accordance with the principles set forth in the Helsinki Declaration and written informed consent was obtained from all the participants. The study consisted of a self- administered questionnaire with 48 questions under four sections handed out to dentists. In the planning of the study, it was targeted to reach all dentists affiliated with the city of Isparta. For this purpose, the questionnaire was implemented to dentists working in Faculty of Dentistry of Suleyman Demirel University and dentists, who are registered with Isparta Chamber of Dentists, working in the public sector or private practice in Isparta and the surrounding provinces and districts. The dentists included in this study were generalist or specialist from all specialties, and were asked whether or not they provided care to the paediatric patients. The questionnaires were distributed to the participants in person by giving information and considering the willingness for participation. The researcher visited each participant at their workplace and explained the aim of the study and received the questionaires after filling out them. The average time to complete the questionnaire was approximately 10 minutes.
The self-administered questionnaire, which was implemented in a 2-month period, included multiple-choice, open-ended and closed-ended questions about participants' personal and educational information and their level of knowledge, attitudes, and experiences on child abuse. The questions were based on the questionnaires from previously published related studies (8,9,10,11). The prepared questionnaire was translated from English to Turkish, and the content validity of it was assessed by two paediatric dentists and one forensic specialist. In line with their suggestions, minor corrections for some items were made to improve wording and clarity, and any items were not excluded from the questionnaire. Prior to the study, a pilot study was performed to test the prepared questionnaire for the feasibility. The questionnaire was implemented in a small sample group of 10 dentists who provide care to the paediatric patients. It was modified according to the feedback obtained from the pilot study and the final version of it was created.
Out of the targeted 305 participants, 183 (60.0%) returned with filled out questionnaires meeting the inclusion criteria, and the data obtained were evaluated and analyzed statistically. Questionnaires that were incomplete or obtained from dentists who did not provide care to the paediatric patient group were excluded.
Statistical analyses
The IBM SPSS (IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.) package was used for data entry and analysis. Answers to the question- naire were processed in the form of numbers and percentages to obtain descriptive statistics. For the continuous data, such as clinician's experience or age, descriptive statistics were obtained by way of calculating the mean, standard error of the mean, standard deviation, minimum and maximum values. Data obtained in terms of clinician experience were classified as <5, 5-10, and >10. Two-way tables were created in pairs between these classified data and Chi-square test statistics were calculated to evaluate the indepen- dence. p value of less than 0.05 (p<0.05) was accepted as statistically significant.
Results
The section of participants' demographics
Table 1 shows personal and educational data of the participants, whose mean age was 33.9 years (min. 23.0-max. 66.0). The gender distribution of the participants was almost equal. The majority of them were married, did not have children, were working in the public sector, were specialists, had >10 years' experience in practice and did not have training on child abuse.
The section of participants' knowledge level regarding child abuse
Dentists' legal obligation to report cases of child abuse in Turkey was stated by 162 partici- pants (88.5%), whereas 10 participants (5.5%) were not informed on the subject (Table 1).
Table 1 Personal and educational data of the participants.
| Data | Participants | - |
|---|---|---|
| - | N | % |
| Gender | - | - |
| Female | 92 | 50.3 |
| Male | 91 | 49.7 |
| Marial status | - | - |
| Married | 102 | 55.7 |
| Single | 81 | 44.3 |
| Having children | - | - |
| Yes | 80 | 43.7 |
| No | 103 | 56.3 |
| Place of working | - | - |
| Public | 151 | 82.5 |
| Private | 32 | 17.5 |
| Specialization status | - | - |
| No | 62 | 33.9 |
| Yes | 121 | 66.1 |
| Experience in practice | - | - |
| <5 | 64 | 35.0 |
| 5-10 | 52 | 28.4 |
| >10 | 67 | 36.6 |
| Training on child abuse | - | - |
| Yes | 17 | 9.3 |
| No | 166 | 90.7 |
| Total | 183 | 100.0 |
| Dentists' legal obligation to report cases of child abuse | - | - |
| Yes | 162 | 88.5 |
| No | 11 | 6.0 |
| No knowledge | 10 | 5.5 |
Table 2 provides the distribution of the information of the dentists according to the signs and symptoms of child abuse. It is seen that the information according to the signs and symptoms was quite different. The majority of participants accepted bruises, bite marks, fear to go home or fear of parents, burn scars, unclear or inconsistent patient history each time, dental trauma that has no reasonable cause and/or that is recurrent and head traumas as the signs and symptoms of child abuse. On the other hand, shy personality, indifferent parents and stubborn child were the less known signs and symptoms of child abuse.
Only 8 participants (4.4%) stated that they had no knowledge on this subject.
More than half of the participants were well- informed on what to do in case of child abuse. However, a non-negligible proportion of the participants, 13 participants (7.1%) stated that they had no knowledge. None of the participants selected the option of 'To do nothing'. Table 3, which includes the steps to be followed in case of child abuse, presents the distribution of the information on what dentists should do when faced with a case of child abuse.
Table 2 The distribution of the information of the dentists according to the signs and symptoms of child abuse.
| Signs and symptoms of child abuse | Participants | - |
|---|---|---|
| - | N | % |
| Bruises | 165 | 90.2 |
| Bite marks | 154 | 84.2 |
| Child with fear to go home or fear of parents | 151 | 82.5 |
| Burn scars | 146 | 79.8 |
| Unclear or inconsistent patient history each time | 144 | 78.7 |
| Dental trauma that has no reasonable cause and/or that is recurrent | 130 | 71.0 |
| Head traumas | 126 | 68.9 |
| Shy personality | 95 | 51.9 |
| Indifferent parents | 61 | 33.3 |
| Stubborn child | 45 | 24.6 |
| No knowledge | 8 | 4.4 |
Table 3 The distribution of the information on what dentists should do when faced with a case of child abuse.
| Action | Participants | |
|---|---|---|
| N | % | |
| To record the signs and symptoms and the suspicion in the child's file | 127 | 69.4 |
| To report to legal authorities | 125 | 68.3 |
| To check the consistency of the explanations given by the parents and/or the child with their clinical findings | 123 | 67.2 |
| To observe the child for this suspicion in later appointments | 115 | 62.8 |
| To inquire the subject through the child and/or family | 113 | 61.7 |
| To consult the case with a doctor, colleague or institution representative | 103 | 56.3 |
| No knowledge | 13 | 7.1 |
| To do nothing | 0 | 0.0 |
In answering the question where to report a case of child abuse; the police was mostly answered by the participants, and a quarter of the participants stated that they had no knowledge on this (Figure 1).
As for their main resource of the information on child abuse, online resources were reported mostly by the participants (Figure 2). Single (33 participants, 40.7%) and <5 years experienced (35 participants, 54.6%) participants reported undergraduate education as their main resource of knowledge on child abuse (p=0.000). Those who were married (45 participants, 44.1%) and had 5-10 (27 participants, 51.9%) and >10 years' (25 participants, 37.3%) experience in practice pointed out online resources and those with an experience of >10 years (24 participants, 35.8%) stated that they did not use any resources as well (p=0.000).
The proportion of the participants' answers for in which circumstances should dentists report cases of child abuse to an authority were 59.0% (108 participants) for recurrent cases, 55.2% (101 participants) for all cases even if abuse is merely suspected, 54.6% (100 participants) for violent cases. Although no participants said that child abuse should not be reported under no circumstances, 19 participants (10.4%) had no knowledge.
Table 4 shows the presentation of the participants' answers for the information questions on the social signs and symptoms of child abuse. The majority (69.9-98.9%) of participants gave correct answers. On the other hand, especially in information questions ''If the parent says the child has been injured by his or her brother, child abuse may be suspected.'' and ''Child abuse is mainly associated with the poverty-related stresses and rarely occurs among middle- or high-income families.'', the correct answer rates were lower than the other questions. The proportion of the participants with only correct answers was 43.7% (80 participants).
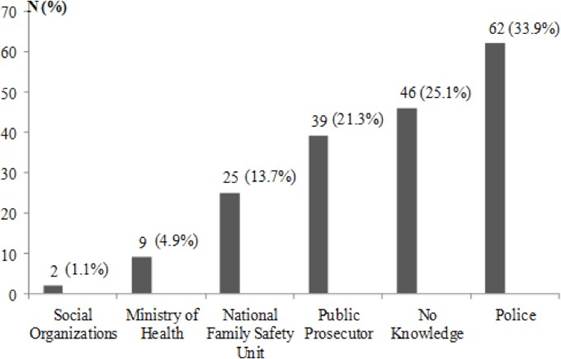
Figure 1 The presentation of the participants' answers for the question where to report a case of child abuse.
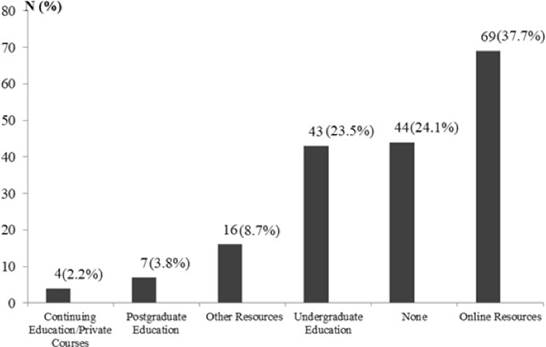
Table 4 The presentation of the participants's answers for the information questions on the social signs and symptoms of child abuse.
| Information questions | - | Participants |
|---|---|---|
| - | -N | % |
| Abused children will usually tell this subject to someone soon. | - | - |
| True | 29 | 15.8 |
| §False | 154 | 84.2 |
| Child abuse is mainly associated with the poverty-related stresses and rarely occurs among middle- or high-income families. | - | - |
| True | 44 | 24.0 |
| §False | 139 | 76.0 |
| In most cases of physical violence, the abuser is a person whom the child knows well from his or her environment. | - | - |
| §True | 169 | 92.3 |
| False | 14 | 7.7 |
| If a child says that an adult has harmed him or her, this accusation should be investigated. | - | - |
| §True | 181 | 98.9 |
| False | 2 | 1.1 |
| If the family has not requested medical treatment for their injured child, child abuse may be suspected. | - | - |
| §True | 174 | 95.1 |
| False | 9 | 4.9 |
| If the parent says the child has been injured by himself or herself, child abuse may be suspected. | - | - |
| §True | 160 | 87.4 |
| False | 23 | 12.6 |
| If the parent says the child has been injured by his or her brother, child abuse may be suspected. | - | - |
| §True | 128 | 69.9 |
| False | 55 | 30.1 |
| The best way to deal with suspected child abuse cases is to confront parents and directly accuse them of abuse. | - | - |
| True | 19 | 10.4 |
| §False | 164 | 89.6 |
§Correct answer.
The section of participants' attitudes on cases of child abuse
Questions about the importance of detecting, recording and reporting cases of child abuse were agreed by almost all of the participants. However, 39.3% of the participants found themselves inadequate in detecting cases of child abuse. The courses on child abuse in the faculties of dentistry were not accepted as adequate by the majority of participants. Dentists in the public sector more frequently stated that ''Dentists should be legally obliged to report child abuse.'' (145 participants, 96.1%) (p=0.003) and ''It is important to provide child abuse training in the work environment.'' (148 participants, 98.0%) (p=0.007). The exhibition of the dentists' attitudes on cases of child abuse is presented in Table 5.
The most commonly stated reasons were hesitancy to identify the case as child abuse, lack of information about referral procedures, and lack of sufficient background information on the case of abuse. Table 6 shows the exhibition of the dentists' attitudes about the reasons for low rate of reporting on child abuse.
Table 5 The exhibition of the dentists' attitudes on cases of child abuse.
| Attitude | Agree N(%) | Neutral N(%) | Disagree N(%) |
|---|---|---|---|
| It is important to detect and report child abuse. | 182(99.5) | 1(0.5) | 0(0.0) |
| It is important to record the signs and symptoms of abuse in the patient's file. | 180(98.4) | 2(1.1) | 1(0.5) |
| It is important to report child abuse to a legal authority. | 178(97.3) | 5(2.7) | 0(0.0) |
| It is important to ask the child about his or her current injury. | 177(96.7) | 6(3.3) | 0(0.0) |
| It is important to provide child abuse training in the work environment. | 176(96.2) | 7(3.8) | 0(0.0) |
| Dentists have ethical responsibility to report child abuse. | 175(95.6) | 6(3.3) | 2(1.1) |
| Dentists play an important role in identifying and reporting cases of child abuse. | 172(94.0) | 8(4.4) | 3(1.6) |
| Dentists should be legally obliged to report child abuse. | 171(93.5) | 11(6.0) | 1(0.5) |
| As a dentist, I can detect cases of child abuse. | 111(60.7) | 58(31.7) | 14(7.6) |
| In the Faculty of Dentistry where I studied, the courses given on child abuse were sufficient. | 19(10.4) | 29(15.8) | 135(73.8) |
Table 6 The exhibition of the dentists' attitudes about the reasons for low rate of reporting on child abuse.
| Reason | Participants | - |
|---|---|---|
| - | N | % |
| Hesitancy to identify the case as child abuse | 155 | 84.7 |
| Lack of information about referral procedures | 130 | 71.0 |
| Lack of sufficient background information on the case of abuse | 123 | 67.2 |
| Possibility of the child being ill-treated by family | 97 | 53.0 |
| Fear of provocation of parents | 84 | 45.9 |
| Fear of being sued | 73 | 39.9 |
| Possibility of harm to professional life | 64 | 35.0 |
| No legal obligation | 47 | 25.7 |
| Lack of time | 32 | 17.5 |
| No responsibility of the dentist | 30 | 16.4 |
All dentists who participated in this study stated that they needed more training on child abuse. Among them, 170 participants (92.9%) emphasized the need on referral procedures to relevant authorities, 170 (92.9%) on legal aspects and 153 (83.6%) on signs and symptoms. While 121 participants (66.1%) requested verbal training, 23 (12.6%) had request for written and 38 (20.8%) for both verbal and written training.
The section of participants' experiences on child abuse
Only 12 participants (6.6%) stated that they have ever suspected a case of child abuse once or twice throughout their professional lives and never found out if their suspicions were to be confirmed or not. Of the 12 participants; 7 (58.3%) inquired the subject through the child and/or family, 6 (50.0%) recorded signs and symptoms and their suspicion in the child's file, 8 (66.7%) observed the child for this suspicion in later appointments and 6 (50.0%) checked the consistency of the explanations given by the parents and/or the child with their clinical findings. In cases where child abuse was suspected, dentists in private practice (6 participants, 100.0%) mostly inquired the subject through the child and/or family (p=0.003) and female dentists (7 participants, 87.5%) mostly followed up and observed the child in later appointments (p=0.030).
As for the procedures to be followed when child abuse is suspected, 23 participants (12.6%) did not know whether their institution provided these procedures. Whereas the institution of 29 participants (15.8%) provided such procedures and that of 131 participants (71.6%) did not. Dentists who were married (76 participants, 74.5%) mostly stated that their institution did not provide the procedures (p=0.025).
Those who have inadequate information in terms of the level of knowledge and attitudes on child abuse are presented with % and p values in Table 7.
Table 7 The association between some factors and the participants' knowledge and attitudes on child abuse.
| - | Female (%) | Male (%) | Single (%) | Married (%) | Yes (%) | No (%) | Public (%) | Private (%) | <5 (%) | 5-10 (%) | >10 (%) | Generalist (%) | Specialist (Any area) (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Legal obligation to report cases of child abuse | - | - | - | - | 81.3 0.019* | 94.2 | - | - | 96.8 | 92.3 | 77.6 0.011* | - | - |
| Signs and symptoms of child abuse | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Bruises | - | - | - | - | 85.0 0.039* | 94.2 | - | - | 98.4 | 86.5 0.022* | 85.7 0.022* | - | - |
| Burn scars | - | - | - | - | 71.3 0.011* | 86.4 | - | - | 90.6 | 73.0 0.027* | 74.6 0.027* | - | - |
| Shy personality | - | - | - | - | - | - | - | - | 40.6 | 30.7 0.001* | 28.3 0.001* | - | - |
| No knowledge | - | - | 0.0 | 7.8 0.010* | 8.8 0.011* | 1.0 | - | - | - | - | - | 9.6 0.004* | 1.6 |
| What dentists should do when faced with a case of child abuse | - | - | - | - | - | - | - | - | - | - | - | - | - |
| To record the signs and symptoms and the suspicion in the child's file | - | - | - | - | - | - | - | - | - | - | - | - | - |
| To check the consistency of the explanations given by the parents and/or the child with their clinical findings | 79.3 | 54.9 0.000* | - | - | - | - | - | - | 78.1 | 55.7 0.037* | 65.6 0.037* | - | - |
| To consult the case with a doctor, colleague or institution representative | - | - | - | - | - | - | - | - | 68.7 | 46.1 0.036* | 52.2 0.036* | - | - |
| No knowledge | 3.3 | 11.0 0.042* | - | - | - | - | - | - | - | - | - | - | - |
| Which cases of child abuse dentists should report to legal authorities | - | - | - | - | - | - | - | - | - | - | - | - | - |
| In all cases even if abuse is merely suspected | - | - | - | - | - | - | 59.6 | 34.4 0.009* | 59.3 | 65.3 | 43.2 0.039* | - | - |
| Recurrent cases | 66.3 | 51.6 0.044* | - | - | - | - | - | - | - | - | - | - | - |
| Some information questions about the level of knowledge on child abuse | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Child abuse is mainly associated with the poverty-related stresses and rarely occurs among middle- or high-income families. | 17.4 | 30.8 0.034* | - | - | 16.3 | 30.1 0.030* | - | - | 35.9 0.006* | 25.0 0.006* | 11.9 | - | - |
| If the family has not requested medical treatment for their injured child, child abuse may be suspected. | - | - | 98.8 | 92.2 0.040* | - | - | - | - | - | - | - | - | - |
| The reasons for low rate of reporting on child abuse | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Lack of information about referral procedures | 81.5 0.002* | 60.4 | 82.7 0.002* | 61.8 | 60.0 | 79.6 0.004* | 74.2 0.042* | 56.3 | 82.8 0.036* | 65.3 | 64.1 | - | - |
| Lack of time | - | - | 24.7 0.022* | 11.8 | 10.0 | 23.3 0.019* | - | - | 25.0 0.007* | 23.0 0.007* | 5.9 | - | - |
| Possibility of harm to professional life | - | - | 43.2 0.037* | 28.4 | - | - | - | - | - | - | - | - | - |
| On what subject child abuse training | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Signs and symptoms | - | - | 76.5 | 90.1 0.013* | - | - | - | - | - | - | - | - | - |
| Referral procedures to relevant authorities | - | - | - | - | - | - | 95.4 0.019* | 83.9 | - | - | - | - |
p<0.05 and %: Those who have inadequate information in terms of the level of knowledge and attitudes on child abuse.
%: Those who have adequate information in terms of the level of knowledge and attitudes on child abuse.
Discussion
Considering studies about dentists not being adequately informed on their legal obligation to report (5,10), the results of this study suggests a high awareness among the participating dentists on the legal obligation of dentists to report cases of child abuse in Turkey. Nevertheless, lack of knowledge on this legal obligation which was observed at dentists who have more experience and children emphasizes the need to periodically update information on this subject through various resources.
As in other studies (5,9,10), bruises on the skin were pointed out as the most common symptom of abuse and other symptoms were found in similar frequency. However, it should not be ignored that bruises may occur due to accidents and systemic diseases, and the location, size, shape, color of the bruise, and age and activity status of the child should be carefully evaluated in terms of diagnosis (25). Only 4.4% of the dentists in this study stated that they had no knowledge about the symptoms of child abuse; shy personality, indifferent parents, and stubborn child were reported to a lesser extent as signs of abuse. That the dentists who were long-time experienced, married and had children did not know the symptoms or all the symptoms of child abuse suggests that information was forgot- ten over time, was not up to date, or these dentists did not keep up with technological developments. Living conditions and responsibilities becoming more challenging with age might be an explanation for this.
Studies evaluating the knowledge of dentists on where to report child abuse cases vary in results depending on countries. Studies in Saudi Arabia and Italy reported a lack of information on the part of dentists about what authorities to seek to report cases of child abuse (9,12). In the study conducted in Saudi Arabia, the levels of knowledge of participants were found satisfactory (5). This study also showed a lack of information of the participating dentists for where to report the cases of child abuse. These differences between countries may be reflecting the varying degrees of effectiveness of the respective laws and legal obligations.
In a similar study, Mogaddam et al. (9) mentioned undergraduate education as the main resource of information on child abuse, while in the current study online resources appeared as the main resource. Differences in the education system and preferences on ways to access information may be responsible for this result. Educational backgrounds related to the topic of child abuse of the dentists included in this study vary. Although this topic did not take a part as a stand- alone topic in the undergraduate curriculum, it was commonly mentioned under other topics of Forensic Medicine and Paediatric Dentistry in dental schools in Turkey and it was under the control of each dental school. The topic was added to the Turkish undergraduate dental education core curriculum and Paediatric Dentistry core curriculum in 2014 and 2011, respectively. As these regulations can be considered new, their impact on the dentists' education can be observed later. Furthermore, if the topic of child abuse is detailed along with clinical settings in the dental curriculum, the knowledge, awareness, and responsibility levels of dentists are increased, and children can be kept away from abuse.
At a study by Owais et al. (10), 30.0% of 342 dentists considered themselves inadequate in identifying child abuse. This rate was 52.2% for 113 dentists in the study of Al-Dabaan et al. (5). As to this study, 39.3% of the dentists found themselves inadequate in detecting child abuse cases. The education on child abuse in the faculty of dentistry was found to be insufficient by the participants of this study, as was in the study with 193 dentists by Al-Amad et al. (4). According to the study conducted by John et al. (8) in Australia, 79.0% of 347 dentists requested written training on the referral procedures to relevant authorities, and legal aspects. Cukovic-Bagic et al. (13) stated that 80.0% of 510 dentists in Croatia required further training in identifying and reporting of child abuse. Furthermore, the studies by Al-Dabaan et al. (5) reported that 92.9% of 113 dentists in Saudi Arabia and Al-Habsi et al. (6) 66.7% of 105 dentists in London required further training on child abuse. All dentists in this study requested more verbal training on the signs and symptoms, referral procedures to relevant authorities, and legal aspects. In light of the demands of dentists from different countries and the proportion of the participants of this study stated that they had no knowledge on what to do in case of child abuse, it is crucial to provide training, especially in undergraduate education, on reporting procedures and legal matters pertaining to child abuse.
Even though dentists should have an important role in diagnosing and reporting child abuse, studies conducted in various countries between 1978 and 2016 showed that the ratio of the cases suspected by dentists was between 8.0-67.0% and even less than half of these were reported (4,5,6,7,8,9,10,11,26,27,28,29). According to the study on child abuse and domestic violence in Turkey, 45% of children between the ages of 7-18 were subjected to physical abuse and 51% to emotional abuse (2). In a study in which 212 paediatric dentists in Turkey participated, it was found that 43.9% of the participants suspected child abuse cases in their professional life, but only 12.7% reported it (30). In another study conducted with a total of 1020 specialists, academics and dental PhD students in Turkey, the suspected rate of child abuse cases was reported as 17% and the reporting rate as 1% (31). From among the dentists participating in this study, only 6.6% ever suspected of a child abuse, but did not report it. Considering the rates of child abuse, it is understood that the rates of suspicion and reporting of child abuse cases are low in Turkey as in other countries. In the question regarding the circumstances a dentist should report a case of child abuse to legal authorities, none of the participants selected the option of 'Under no circumstances,' yet the other options were selected at a rate of 50.0%, which suggests a failure to report.
The explanations suggested for the low rate of diagnosis and reporting of child abuse by dentists mostly include inadequacy and hesitancy in recognizing the findings of abuse, insufficient knowledge and training on the subject, fear of being sued, possibility of harm to professional life, fear of causing harm to the child or family, and privacy concerns (4,5,6,7,8,9,10,11,32). In the current study, the most common reasons for the low rate of reporting cases of child abuse appear as hesitancy to identify the case as child abuse, lack of information about referral procedures, and lack of sufficient background information on the case of abuse. It is also a reflection of this situation that only less than half of the participants answered all questions about the social signs and symptoms of child abuse correctly.
In their study, Owais et al. (10) determined a statistically significant difference between the reporting rates of dentists in private practice and those employed by a university. According to this, most dentists working in private practice selected the option of not reporting. Furthermore, Azevedo et al. (28) found that dentists working at universities were more likely to suspect child abuse. However, some studies concluded that there was no statistically significant difference between dentists' knowledge level on child abuse and the institution they work in, their clinical experience and specialization (32) or between dentists' suspicion of child abuse and their gender, clinical experience and specialization (11) or between dentists' reporting of a suspected case of child abuse and their workplace, education and duration of experience in the profession (30). On the other hand, Manea et al. (12) identified the female gender as a factor affecting attitudes on child abuse. In another study, performed by Mogaddam et al. (9), it was reported that the vast majority of dentists with the profile of older in age, female and employed at a university were able to correctly identify the signs and symptoms of child abuse and to take action upon a suspicion. The majority of dentists working in a university were also found to know better the circumstances where a child abuse report must be made. This study showed that dentists who had children and long-time clinical experience did not have sufficient knowledge about the legal obligations and signs and symptoms of child abuse. As for the knowledge on what should be done and which circumstances should be reported when faced with a case of child abuse, dentists who were male and had long-time clinical experience displayed the same inadequacy. Inadequate under- graduate education on the subject and forgetting of current information with age may have caused this situation. Besides, in a study in which high school students' perceptions of violence were evaluated, it was found that gender affected the tendency of violence and male students had more tendencies to violence. This finding was explained by the fact that, despite the importance and tolerance given to the male child in the society in question, the child experiences more violence due to the rebellious behavior during adolescence and tends to experience violence in the face of problems (33). Therefore, it should be noted that male dentists' identification, diagnosis and reporting of cases of child abuse can be influenced by the effect of gender on tendency of cultural violence. The fact that special dentists are more knowledgeable about the signs and symptoms of child abuse as compared to general dentists is indicative of the positive effects of specialization education in a university, both in terms of learning from the institution and from colleagues and also staying up to date with information and to follow the literature. Upon a glance at the reasons of low report rates in cases of child abuse, it was understood that dentists who were female, single, childless, working in the public sector and little clinical experienced were more concerned. This may be related to the low level of awareness, experience and education of younger dentists about the subject. It is also important that physical and emotional punishment for disciplining the child in the family is considered normal and not seen as an abuse in Turkish society in which the dentists participating in this study live (24). Considering that the dentists' perceptions of violence are influenced by cultural characteristics, changing beliefs and attitudes towards the violence through education is also important in preventing, diagnosing and reporting child abuse.
Child abuse is a serious public health problem and health-care providers are considered to have an important role to recognize and report cases of abuse. Early intervention and protection of children from further violence can only be possible through awareness-raising studies. In this respect, this study was carried out to present the knowledge levels, attitudes, and experiences of dentists about child abuse. However, this study has some limitations. One of these is that it presents data on dentists affiliated with a single city. Although it covers a limited area, it is important in terms of the current situation for handling child abuse cases of a group of dentists from Turkey. Another one is that dentists providing care to the paedia- tric patients were included in the study, but the average number of children provided care by each dentist was not known. As the number of paediatric patients provided care increases, the experience on the subject may increase, and accordingly, the need to update the level of knowledge and attitude may arise. On the other hand, considering that the current lack of knowledge of the dentists in our study was due to individual characteristics and the education curriculum, it could be stated that the number of children provided care might not have affected the situation.
Conclusions
The lack of adequate knowledge about child abuse, the failure to report suspected cases to authorities and the need of more training neces- sitates arrangements in undergraduate education. Further, verbal training programs on referral procedures to relevant authorities, legal aspects and signs and symptoms to increase the knowledge, awareness, and responsibility levels of dentists appear to be a critically important topic. Regular updates of relevant information through diverse resources should also not be neglected.

