











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
Temporomandibular joint dysfunction syndrome (TMD) is a term used to describe a series of clinical problems related to the temporomandibular joint (TMJ) and the masticatory muscles and other associated structures.Commonly related to trauma, neoplasia, stress, anxiety, occlusal interference, poorly positioned teeth, bruxism, tooth loss, poor bone base ratio, parafunctional movements, harmful habits, and intrinsic temporomandibular joint problems, which may or may not appear in combination (1). The main signs and symptoms are muscle and joint pain, noises in the joints (cracking and/or clicking), restriction of jaw range of motion, and changes in jaw movement pattern. It can present with tinnitus, vertigo, lack of muscular coordination and biomechanical imbalance of the cervical region (2). In addition, a variety of other symptoms can occur, such as abnormal swallowing and tenderness of the hyoid bone; these symptoms can compromise quality of life and even sleep. In severe cases, a headache occurs, as well as possible neck pain, vertigo, ear pain, muscle fatigue in the orofacial and cervical region in the skull region (1,3,4).
Epidemiological studies show that approximately 75% of the population has a DTM sign and 33% have at least one symptom (4). A specific etiology for DTM problems has not been identified (5).
Authors agree that substantial reduction in mouth opening and movements are strong indicators of DTM, as well as helping to distinguish between DTM and non DTM patients. Currently, the clinical examination is the "gold standard" for the diagnosis of DTM and involves the assessment of mandibular movements, palpation of masticatory muscles and the use of the stethoscope to evaluate joint sounds (6). According to the criterio of the American Association of Oral and Maxillofacial Surgeons ≥40mm maximum mouth opening without pain are classified as: clinically no degree of joint dysfunction and below this measure, it is considered with DTM (7). According to the main origin of pain and based on the presence or absence of joint noises, they have been classi- fied into myogenic, arthrogenic disorders and degenerative joint disease (8). The criteria for evaluating patients with DTM, under any therapy are: muscle and joint palpation and the range of mouth opening. Pain is considered the basis of every diagnosis and therapeutic approach. Muscle pain is an important clinical sign, in the affected muscle, which is present in most patients with orofacial pain and evaluated by palpation examination identifying trigger points (PT) or measuring instruments. During the clinical evaluation, the amount of pain experienced must be evaluated. The visual analog scale (VAS) is typically used to determine the level of pain (9).
Primary treatments should be conservative and reversible, and should focus on the control and reduction of symptoms. Nonsteroidal anti-inflammatory drugs remain the first rational treatment option for patients with pain of inflammatory origin, such as arthralgia. Piroxicam administered daily for 10 days has shown a reduction in the levels of several cytokinin (IL-1β, IL-2, IL-2R, IL-4, IL-6, TNFα, IFN-α) in patients with acute inflammation, showing no side effects (10). Other treatment modalities (including NSAIDs), consist of the use of pain relievers, muscle relaxants, cryotherapy, heat therapy, physical therapy, bite plates, chewing exercises, psychotherapy, acupuncture, manual therapy, ultrasound, relaxation, transcutaneous electrical nerve stimulation (TENS), low intensity laser therapy (LLLT), or ''photo modulation'' therapy. The LLLT has been brought under the spotlight ''recently'' due to its easy application, short treatment time, and few contraindications (1,3,4,11).
The effects of LLLT that have been highlighted are analgesics and anti-inflammatories (11). According to various studies, LLLT has shown beneficial results with respect to pain derived from DTM (2,3,4,11,12,13,14,15,16); it resulted in the immediate reduction of painful symptoms and a greater range of movements mandibular in the treated group (12). However, for others the LLLT has not shown be more effective than other therapies to simultaneously resolve both pain and impairment of orofacial functions in DTM (13).
The gallium arsenide laser is the most effective in the treatment of pain, inflammation and functional disorders in muscles, tendons, joints and profound dysfunctional problems in general. Reaching from 30 to 50mm in depth, depending on the type of tissue. It emits an infrared ray with a wavelength around 904nm. They always operate in very short pulses (100-200ns) commonly called ''super-pulse''. This pulsation constant simplifies the treatment time considerably and increases the safety for patients (14). The proposed mechanism of action is the increase in the production of β-endorphins, a triphosphate, which can result in muscle relaxation. ATP synthesis, enhanced by LLLT, leads to hyperpolarization and stimulus blocking, which decreases the induction of painful stimuli. In addition, inhibition of prostaglandin E2 and interleukin 1 beta will reduce pain induction. The improvement of circulation in peripheral blood vessels also plays an important role in reducing pain, accelerating the elimination of catabolites in the tissues (7,15).
Materials and methods
A controlled clinical trial (double-blind-randomized) was carried out in 30 patients, who presented DTM problems of arthrogenic etiology, who were admitted to the Clinic of Temporomandibular Dysfunction-Faculty of Dentistry, UASLP, México. Carrying out lower risk therapeutic procedures, respecting the norms dictated by the OMS and the Helsinki Conference in reference to experimental medical research carried out in humans. With acceptance of the Institutional Research Ethics Committee (CEIFE/022/09), the patients were informed of the purposes and risks of the study, verbally and through informed consent, signed voluntarily their participation.
Patients with a family hereditary history of cancer, pacemakers, hypertension, epilepsy, pregnant or lactating, with thyroid diseases, hypersensitivity to the drug formula (piroxicam), with gastric ulcer, hemorrhage or anticoagulant treatment, with kidney damage, with severe laterognathia (5mm or more) or patients with systemic hypermobility syndrome were excluded. Likewise, intra observer consistency was evaluated in the expert for the examination of positions and movements. For this, 15 patients who attended were selected, each of these patients was reviewed by the expert on 2 separate occasions. The R2.11.1 program was used: intraclass correlation coefficient analysis, Lin's concordance coefficient and repeatability coefficient of all measured variables were performed. The digital pressure used (in TMJ and orofacial muscles, initially) was calibrated and assessed bilaterally for 2 seconds using a digital scale (2 pounds for extraoral muscles/1 pound for intraoral and TMJ). All of these evaluations returned ranges from good to perfect. Except for consistency tests, pressure on the extraoral muscles, with a poor range. This leads to elimination of myogenic patients (characterized by pain in mandibular movements or in its function, and confirmation in its location, to palpation in masticatory muscles: masseter, temporal) giving way alone, to patients of the arthrogenic group (30 patients). Finally, selecting both sexes, between 18 and 60 years, mouth opening less than 40mm, joint pain of more than 6 months, audible click(s) when opening and closing the mouth, present to palpation by placing index fingers (calibrated/ consistency tests) in ATM zones (evaluation in both joints), without sounds of crepitus, nor mandibular blockage (subluxation or joint blocks).
Randomization was carried out using a list of block numbers (random) previously made (package R 2.9.1) that corresponded to the experimental group ''A'' (active LT+NSAID) and to the control group ''B'' (Non-active LT-''passive''+NSAIDs) according to the order of appearance of each patient, being marked (canceled), giving rise to the next one. For blinding (double blind), the evaluator was asked to leave the clinic for the 'application' of treatment (as appropriate). The application protocol was simulated in the control group (supposed laser application and lens placement) without being turned on (passive). Later, the clinical assessment was made. This was done at each visit by an expert (after clinical calibration-intra observer consistency tests). The evaluator was blinded to the hypothesis and the application.
On the other hand, an LLLT (Gallium Arsenide-Quantum ® IR810, therapeutic laser, Laser Systems, Qro, MX.) was used with the following specifications: main power: 120v, output optical power: 100-200 mw, wavelength: 810 nm, emission: PW=Pulsed (1-10,000 Hz), Divergence: 7.9°, Dose: 10 jouls-cm². The treatment consis- ted of five laser applications (three times, the first week and two the following week). One month later, the follow-up appointment was given, with a total of six appointments. The patient located the area of pain in the TMJ and the LLLT was applied on two occasions, one in a punctual manner (1.44 minutes) with the mouth closed and another, with the mouth semi-open with the ''sweeping'' techni- que at each of the ATMs. The clinical evaluation was carried out at each appointment, after placing the LLLT in the same way in the two groups. The dose is the most important parameter, it refers to the amount of energy per unit area in a tissue. In the calculation, the area was measured in cm². In the following formula, the ''D'' is the measurement in Joules per square centimeter (J/cm²) and is calculated as follows: Pxt/A=(100 mW x 104 seg.)1 cm² =10 Joules/cm² It is therefore recommended to use the laser 3-4 times a week, with moderate doses. Others recommend at least one application per week (14,16), coinciding with the treatment scheme carried out.
ABM, joint capsule (by means of VAS with millimeter ''ruler''), right and left laterality, protrusion (with vernier caliper), pathological noises (by stethoscope/number of sounds) in TMJ and count of capsules (NSAIDs) ingested for each group were evaluated. Regarding the ABM, the patient was asked to open his mouth as much as possible (without pain) and the measurement was made from incisal edge to incisal edge in the central area. The joint capsule force was digitally applied in the central-lateral part in order to find a PT, later it marked a line on a ruler, using VAS (0 to 100mm). The right and left laterality were recorded, that is; the movement of the jaw to the side to which it moves (working: right or left). A reference line was drawn in the upper central anterior teeth, going down to the lower anterior teeth on the buccal aspect, the patient was asked to bring his jaw to one side, as far as possible and another reference line was again marked with the same characteristic than the previous one, then the patient was asked to do the same, to the opposite side and marking a third line again. These lines corresponded to the laterality that were recorded. The protrusion was also registered, that is; movement carried out by the jaw when it is brought forward. A line was placed in the area of premolars from the upper to the lower, when it is in occlusion. Following this, the patient was asked to bring his jaw as far forward as possi- ble and another reference line was again marked, the distance between the lines being the recorded protrusion. The number of pathological joint noises (clicks) was recorded, using a stethoscope in the two joints, the patient was instructed to make repeated opening and closing movements. With a minimum: 0 (zero noises) and a maximum: 4 noises at the ATMs. Concerning the medication, in both cases the same presentation and dose of the NSAID (Piroxicam- 20mg tablet-oral use) was used at ''free demand'' (1 tablet every 12 hours/ maximum). The patient was monitored after finishing their treatment (in both groups) for one more months, in order to evaluate the changes produced and accumulation, if applicable.
A descriptive analysis of the data obtained with the statistical program, ''R'' version 2.11.1, was carried out with a confidence level of 95%, carrying out a mixed model analysis with the nlme package. A value of P<0.05 was considered significant. For the sample size, the following formula was considered: Number of factors x 10; therefore: 3 factors (treatment, age, sex) x 10=30 patients (15 patients per group).
Results
Among the 30 patients that were selected, 28 finished the treatment, two of them were lost to follow-up (appointment 6) of the experimental group. All patients had signs and symptoms of the arthrogenic group. The gender distribution of DTM was 20 women (80%) and 6 men (20%). The most frequent age in which DTM occurs was in the 20 to 30 years old interval with 10 patients (33.3%) with a mean of the 2 groups of 30.80 years old.
To establish the similarity and comparability of the groups studied, parametric and non-parametric tests were performed, depending on the normality of the data. The quantitative variables were analyzed by the: Student's t test, for variables with normal distribution or U Mann-Whitney-Wilcoxon test. Fisher's exact test was performed to analyze the qualitative variables. In demographic variables, both groups were similar concerning age and sex (P=077, P=065 respecti- vely) (Table 1).
Table 1 Data of the patients of the two groups of all the baseline variables.
∝Student's t; *U Mann-Whitney-Wilcoxon; ΩFisher's exact test; IQR= Interquartile range.
Regarding mandibular functional baseline parameters, such as: the main output variable ABM (to evaluate the efficacy of LT in DTM and to distinguish between those with DTM), they indicated no statistical differences in the experimental groups compared to control (P=0.14). The same for other functional variables such as: left laterality, right laterality, or protrusion (P=.19, P=0.20, P=0.96 respectively). Likewise, for pain interpreted by the patient, when performing digital palpation in both joints using VAS, there were not statistically difference (right, P=0.9; left, P=0.3). The same in case of left and right noises, when the two groups were initially compared, indicating that they were similar groups (right, P=0.64; left, P=0.21). Once the similarity between groups was established, we proceeded with results and inferential analysis. The baseline measurement, the mean found for ABM in the experimental group was 26.2mm with a 95% CI of 22.3 and 30.2mm, and at the last appointment a mean of 32.4mm with a 95% CI of 27.6 and 37.2mm. (Figure 1). In control group at the first appointment, the mean was 30.2mm with a 95% CI of 26.2 and 34.1mm. At the last appointment, a mean of 38.1mm with a 95% CI of 34.8 and 41.51mm.
The mean found for right laterality in experi- mental group was 6.13mm at the first appointment with a 95% CI of 4.88 to 7.38mm, at the last appointment there was a mean of 8.46mm with a 95% CI of 7.21 to 9.72mm. In control group at first appointment, the mean was 7.20mm with a 95% CI of 5.97 to 8.42mm, at the last appointment a mean of 8.60mm with a 95% CI of 7.34 to 9.85mm was presented. The mean found for left laterality in experimental group was 7.06mm in the first appointment with a 95% CI of 5.67 to 8.46mm, at the last appointment a mean of 9.00mm with a 95% CI of 7.58 to 10.42 mm was presented. In control group at the first appointment, the mean was 8.40mm with a 95% CI of 6.80 to 9.99mm. At the last appointment, a mean of 8.46mm was presented with a 95% CI of 6.95 to 9.97mm. Both are presented in Figure 2.
The mean found for protrusion in experimental group was 5.96mm at the first appointment with a 95% CI of 4.70 to 7.22mm, at the last appointment a mean of 6.53mm with a 95% CI of 5.35 to 7.71mm was presented. In the control group at the first appointment, the mean was 5.93mm with a 95% CI of 4.85 to 7.01mm. At the last appointment, a mean of 6.73mm was presented with a 95% CI of 5.74 to 7.72mm (Figure 3).
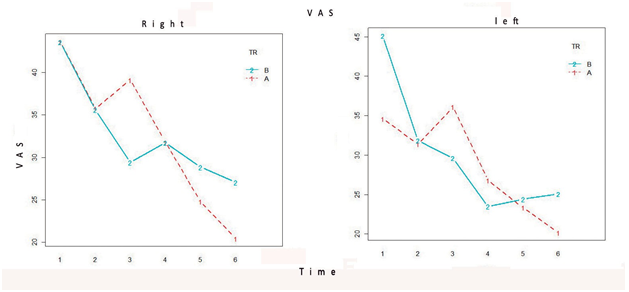
For the evaluation of the right joint capsule by VAS, 43.60mm was obtained in experimental group at the first appointment with a 95% CI of 26.93 to 60.27mm, at the last appointment a mean of 20.47mm was presented with a 95% CI of 9.18 to 31.75mm. In control group, at the first appointment, the mean was 43.53mm with a 95% CI from 30.16 to 56.90mm, at the last appointment a mean of 27.07mm with a 95% CI from 11.77 to 42.36 was presented. For the evaluation of the left joint capsule using VAS in experimental group it was 34.60mm at the first appointment with a 95% CI of 20.10 to 49.09mm, at the last appointment a mean of 20.20mm with a 95% CI of 8.95 to 31.45mm was presented. In control group at the first appointment, the mean was 45.13mm with a 95% CI of 29.33 to 60.93 mm, at the last appointment a mean of 25.07mm was presented with a 95% CI of 13.31 to 36.82 mm (Figure 4).
Regarding the NSAID that was offered, only 9 patients ever took piroxicam (30%), of these; 19 piroxicam tablets in group A (13%) and 24 tablets in group B (16%). No adverse reactions were reported in either group.
Finally, multiple regression analysis of repeated measures and mixed models was performed to explain the observed final mouth opening, finding that only the initial mouth opening and the observation time were important in the final model. The variables gender, age, treatment, and the treatment: time interaction were not significant for this model.
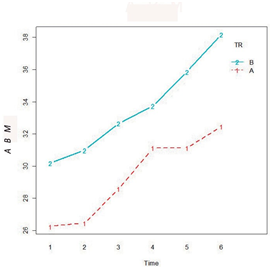
Figure 1 Graph showing ABM (in mm) over time (citations/6), red line (experimental) and blue line (control).
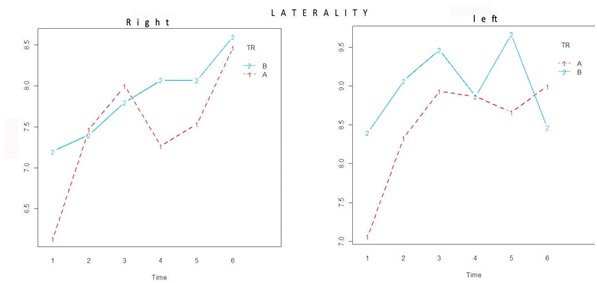
Figure 2 Graphs showing the laterality (in mm) in time, right and left (citations) of the two groups, red line ''A'' (experimental) and blue line ''B'' (control).
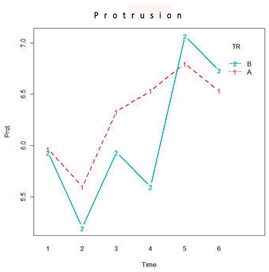
Figure 3 Graph showing protrusion (in mm) in the two groups over time (citations), red line ''A'' (experimental) and blue line ''B'' (control).
Discussion
Studies have been concluded that LLLT has no detrimental effect on patients and could be a good option for patients interested in non-invasive therapy. It has been considered as a complementary option for the treatment of DTM, due to its effects: biostimulants, regenerative, analgesic and anti-inflammatory (16,17). However, in present study the results indicated that LLLT was not effective in treating DTM, functional parameters (ABM, laterality, protrusion) nor in reducing joint capsule pain (VAS) or TMJ noise compared to control group (NSAID), perhaps due to the "application protocol" used (irradiated dose, type of laser, wavelength, number of sessions) among others. One factor that can be found is that the dose irradiated with LT is very diverse, according to a meta-analysis, from 1.5 J/cm² to 112.5 J/cm² (3). In this study and in accordance with the dose recommendation (10 Joules/cm²) as the most important parameter. As well as the number of applications per week (3 to 4 times), we were able to note that the results were not positive in any of the variables measured, including VAS (pain reduction) or improvement in oral function (ABM, laterality, protrusion) (14).
In recent meta-analysis, the results of the DTM function, evaluated in terms of maximum active and passive vertical opening, lateral excursions and protrusion, indicated that the general effect favored LLLT over placebo but with a great diversity of parameters of irradiation (3). Other studies suggest that LLLT is effective for pain reduction in 6 sessions applied in 3 weeks, 1W, but without bone abnormalities (but with unclear methodology and a small sample) (15). As well as to improve orofacial function in patients with DTM, although with very different application schemes and types of lasers (GaAlAs, GaAs, HeNe, Nd: YAG, Diode laser, etc.) (3,4,12,14,15,16,17,18). In other study, two LLLT types and irradiations (two LED/experi- mental groups and one infrared/control) were compared in three groups. The first two with 18 J/cm², 9 J/per point and a third control group with 105 J/cm² and 4.2 J/per point. The irradiation parameters in the experimental groups were: the red LED group (630±10nm, 150mw) and the LED group (850±10nm, 300mw/cm²). The control group received infrared laser (780nm) with 70mw, 1.7 W/cm², applied in eight sessions, twice a week for the three groups. They concluded that there was a significant reduction in pain and an increase in maximum oral opening for all groups (P≥0.05). However, there was no significant difference between the different laser groups (19).
On the other hand, one of the possible reasons for the negative results that have been reported is the use of extremely low doses. The number of treatment sessions is another parameter that does not have an elaborate consensus. Most of the studies report 10 to 20 treatment sessions; however, doses higher than 700 mw applied it in 6 sessions with "positive" results, but did not include a control group (4,20). The significant reduction in pain reduction in masticatory myalgic muscles has also been recorded after the use of LLLT in various modalities ("photo modulation") and even a single application of LLLT, but without changes in ABM (9). The diversity of the ''application protocols'' can be clearly noted (20,21).
Others have documented that LLLT promotes positive effects in DTM, despite the differences due to: wavelength and energy density (dose) (13). Regarding the wavelength, the present study agreed with this report, in that; was not effective, using a similar application protocol with parameters of: 810nm, but with 3.4 J/cm² (in 4 points) and in sore muscles (it does not mention how many) and an increase to 12 sessions, three per week (against 5 sessions in our study), using 50 mw (half of what we used in our study) but this did not reduce pain, nor did it increase mouth opening (22). Other studies do not observe differences between groups or with limited results (21,22,23). In contrast, in a recent meta-analysis that concluded that LLLT can significantly improve the range of movements of the jaw of patients with DTM but has limited efficacy in reducing pain (24).
For ABM, in this study, there were no statistically significant differences between the groups studied, based on the mean periods. The average of the first ABM appointment in the experimental group was 26.2mm, in the last appointment a mean of 32.4mm was presented. In the control group at the first appointment, the mean was 30.2mm. At the last appointment, a mean of 38.1mm was presented. Coinciding with Shobha et al., when they compare LLLT (Gallium aluminum arsenide, 810nm, 0.1W) against placebo, but in 8 sessions for reduction of TMJ pain during function, suggesting that LLLT does not is better and what; LLLT applications ''tailored'' or ''more personalized'' will have to be carried out taking into consideration the multifactorial aspect of the DTM (25).
For Chellappa and Thirupathy, when compared transcutaneous electrical nerve stimulation (TENS) and LLLT (Diode laser, 672nm, 3 J per site, in four of them, 2 weekly) but in a variety of DTM problems (recurrent pain, chronic, reciprocal clicking, restriction to open the mouth or deviation of the jaw) significant improvement in the range of motion and pain relief was observed for both therapies. After analyzing the two methods, the values obtained after LLLT were significantly higher than those obtained after TENS therapy (P<0.01), including painless mouth opening (26). Regarding laterality and protrusion, we did not find significant statistical differences in this study, coinciding with others (21) as they did not find satisfactory results in lateral mandibular movements with an infrared laser, but with different parameters (780 nm, 30 mw, 10 s, 6.3 J/cm²) at three ATM points in 6 sessions. It can also be found where the LLLT, if it is effective in this regard (4,12,24) in this last meta-analysis 14 controlled clinical trials were analyzed, which indicated a significant increase in mandibular movements (ABM, protrusion and lateral movements) in patients with DTM.
Regarding the left and right VAS, there were no statistically significant differences between the groups analyzed, coinciding with others (21,23) or limited in chronic pain (24). However, for others, the effect in general favors LLLT, as shown by several studies (1,2,3,4,12,15,16,18,19,20,26,27,28). Other meta-analysis mentions the data found from 643 participants in 17 studies, which indicated a statistically significant reduction in total pain scores in the LLLT versus placebo groups but according to these reports at high reported doses (52.5 or 105 J/cm²). Whether the LLLT depends on the irradiation (dose) applied or no is still under debate. Sixty patients with Painful Myofacial Syndrome (having at least 1 active pain point in the masseter or temporal muscle) treated with GaAlAs laser (780 nm), applied continuously, twice a week, for four weeks. The energy (dose) was established at 25 J/cm², 60 J/cm² and 105 J/cm², respectively (in 3 groups). And 3 other groups were treated with placebo applications. Pain scores were evaluated. There were no significant differences between the application regimens used (P>0.05). Pain remission was time dependent (P<0.001). The analge- sic effect was similar in the LT groups and control groups (28). Regarding joint sounds, in our study no differences in the groups studied were found; however, as described by Sayed et al. a decrease in joint sounds, after 6 applications (3 times a week for 2 weeks) of LLLT (gallium arsenide; 904nm, 0.6 W, 60s, 4 J/cm²) in 20 patients, mostly of myogenic origin and 8 mostly of arthrogenic origin, ranging from 18.21% at the first appointment to 55.04% at the last appointment (sixth appointment). However, they did not have a control group; likewise, the sample size was ''small'' (20 individuals at the end) and 8 who left the study (4).
Even without establishing a protocol for TMJ pain, even with different groups within it, this report compares 3 groups with the use of piroxicam against LLLT (group: L/Laser, group: Pi/piroxicam and the group: Lpi/Laser+piroxicam), but indicates that there were no significant differences between the groups (P>0.1) (10).
Regarding the taking of the drug in this study, we found contrasting data, since when the drug intake was recorded (relatively low) and the degree of pain that had occurred in the last days (relatively high, according to some patients). No patient exceeded the recommended dose indications. The variable ''time'' in our study suggests an important role for the remission of DTM problems of arthrogenic etiology or similar classifications. Also described as "placebo" or "self-limiting effect" (28,29). When the use of piroxicam as an adjuvant to conservative treatment has been analyzed, it does not seem to significantly influence the result of conservative treatment. As an example, in this report, the experimental group (14 subjects) received conventional therapy (bite plane, occlusal readjustment, tranquility) with 10 mg of the drug orally, twice a day; and the control group (12 subjects) received the same treatment and a placebo (control group/12 subjects). The subjective reactions (subjective dysfunction and subjective pain) and objective (objective dysfunctional parameters/Helkimo index), almost all changed in the same positive way for the two groups. Only subjective pain symptoms decreased significantly more in the drug group (29). In contrast, according to this author, a combination of NSAIDs and physiotherapy for 4 weeks is effective as the primary treatment of patients with disc displacement without reduction and without bone changes. There was a 60% improvement in the treatment group compared to 33% in the control group over the full 4 weeks (7). If, pharmacotherapy with NSAIDs (naproxen) is compared against LLLT, in myofacial pain disorder syndrome, the naproxen group, neither the intensity of the pain, nor the maximum opening of the mouth had a significant improvement. While in the LT group, ABM increased and pain intensity decreased (P<0.05) (30). A placebo effect of LLLT (for the use of ''high technology'') has been reported, one month after the follow-up (31) as well as cumula- tive, which suggests a gradual improvement and reduction of pain at 15, 30, 60 days, remaining until after one year (21), which could not be identified in this study in the LLLT group (at 30 days of follow-up). This author reports that, at 30-days follow-up, the use of piroxicam was more effective than the use of LLLT, even when LLLT and piroxicam were combined (10). The joint sounds are due to a more complex effect that could not be resolved in the majority of our patients with TL.
Conclusion
In this study, we did not find statistical differences between the groups studied in terms of clinical functional parameters (ABM, protrusion, right and left laterality) nor in the mandibular parameters of arthralgia evaluated by the VAS scale. This study indicates that LT was not an effective tool (with parameters used) for the treatment of the measured variables, in patients with DTM of arthrogenic etiology.
Author contribution statement
Conception and designing of study: J.C.M., A.P.G., A.G.M.
Literature review: J.C.M., A.P.G., A.G.M.
Methodology and validation: J.C.M., A.P.G., A.G.M. Formal analysis: A.G.M.
Investigation and data collection: J.C.M.
Data analysis and interpretation: J.C.M., A.P.G., A.G.M. Resources: J.C.M.
Writing-original draft preparation: J.C.M., A.P.G., A.G.M.
Writing-review & editing: Josué J.C.M., A.P.G., A.G.M.
Supervision: A.P.G.
Project administration: A.P.G.
Funding acquisition: J.C.M., A.P.G.

