











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
The histiocyte is a cell of the immune system that includes macrophages and dendritic cells, one of the main dendritic cells are the Langerhans cells (1). These cells reside in the basal and super basal layers of the epidermis and epithelial of urogenital, respiratory and gastric tract, the proliferation of mature histiocytes and an inflammatory infiltrate can emerge in any organ causing Langerhans Cells Histiocytosis (LCH) formerly known histiocytosis X (2). This disorder is of unknown etiology, and accordingly with the number of lesions and sites involved, LCH is categorized as single or multisystemic disease (3,4).
LCH is a rare proliferative disorder, more common in males and it occurs in 1 to 2 newborns per million per year (5). The incidence in children<15 years is 4 to 5 cases per million per year (6). Apparently, the risk is influenced by the ethnicity; some studies in the United States of America showed an increased risk in Hispanic children (n=162; OR: 1.51; 95% CI: 1.02-2.25) (7).
Although there is no sufficient evidence, according to Venkatramani R. et al, (2012) it is more likely to report family history of cancer (OR 2.5), parental occupational exposure to metal, granites, or wood dust (OR 2.48), and infections during infancy (OR 2.76) (8). LCH can affect any organ of the body, but those frequently affected in children is the skeletal system (80%), skin (33%), the pituitary gland (25%), liver, spleen, hematopoietic system or lungs (15% each), lymph nodes (5-10%) or the central nervous system (2-4%) (4,9). The most common site of bone involvement is the skull, particularly the jaws. The oral manifestations frequently intraosseous lesions, affection of posterior area of mandible, anterior mandible, soft tissues of buccal mucosa, gingiva and tongue (9,10). Eden P., et al., reported in a case series (n=13), 7 of the cases showed intra osseous lesion in the posterior region of the jaw and oral mucosal involvement (tongue, buccal mucosa and gingiva) (11).
The diagnose of LCH is challenging since the manifestations are common to other diseases, in the infant stage. Skin lesions typically manifests as vesicles, pustules, or both, which can be mistaken for varicella (12). Since oral manifestations are frequent, bone lesions are commonly asymptomatic but depending of the size of the lesion can include dull pain, limited range of movement, periodontal disease or tooth loss. Other lesions should be suspected in the differential diagnosis such as odontogenic tumor, osteomyelitis, granuloma, other malignant neoplasms (13,19). Due to the challenges for the diagnose of LCH is recommended a clinical-radiological-histopathological analysis, and always confirmation by immunohistochemistry (10,14,15).
The treatment choice depends on the lesion presentations. Surgical curettage if the lesion is solitary, radiotherapy or chemotherapy are also recommended (4,9,10). The intralesional infiltration of corticosteroids has been reported to effective to unifocal bone lesions, however, is also recommended adjunctive chemotherapy to prevent relapses (16). The overall prognosis for this rare disease is good and is better in children over adults, with 5-year relative survival rates of 90% vs 70%, respectively; and relapses can occur in a third of the patients (14,20,21,22). However, it depends on involvement of risk organs like bone marrow, liver and spleen (18).
The case of LCH we report affected an 8-year-old boy, who was firstly diagnosed with a dental infection. As we mentioned previously, oral lesions can be the first sign of LCH, and dentists may be the first to detect this disease, allowing an early diagnosis and referral to the appropriate specialist, thus avoiding a wrong diagnosis and the advance of this disease that in the severe cases can be fatal.
Case report
An 8-year-old male and his mother referred that in May of 2019 they noticed an increase of volume on the left mandible region and a loss of 5 kg in the previous 6 months. In June 11th 2019, he was taken to the general dental practitioner, who performed odontotomy of primary first and second molars, the diagnosis was infection and was prescribed to take antibiotics for 14 days. The evolution was torpid, so in June 27th of 2019, the boy was referred to the Maxillofacial Surgery Department of General Hospital Boca del Rio.
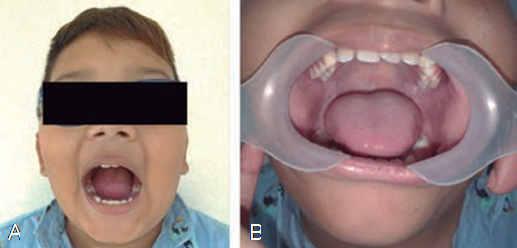
On physical examination, the patient exhibited good general health status, his weight and height were 42 kg and 142 cm (96th percentile), normal mental status, no lymphadenopathy was found, the parents report no history of chronic degenerative diseases, medication use, allergies or previous surgeries (Figure 1). The patient was cooperative, oral cavity presented without alterations and in mixed dentition. During the extraoral examination, an increase in volume was observed in the parotid region of approximately 3x3 cm, well defined, indurated and normal skin. The patient complained of pain during palpation and chewing.
Based on the clinical data and medical history, the maxillofacial surgeon indicated a lateral skull radiograph (Figure 2), where atypical bone lysis was observed according to the age of the patient. Then a computed tomography was requested to determine the limits and three- dimensional characteristics of the lesion, where cortical expansion with bone lysis was observed Figure 3), which led to a presumptive diagnosis of a malignant tumor in the mandibular angle to be determined, also laboratory tests were requested showing increased levels of alkaline phosphatase (212 U/l), serum phosphatase (6.9 mg/dl) and serum calcium (10.7 g/dl). According to clinical, imaging and laboratory examination, the maxillo- facial surgeon performed incisional biopsy in June of 2019. The patient underwent general anesthesia with orotracheal intubation, carried out via an intraoral approach with an incision in the left anterior border of the mandible branch dissecting to the mandibular angle of the external fase and performing an ostectomy with a low-speed handpiece at the site of the lesion, bone tissue was obtained for histopathological analysis.
The hematoxylin and eosin stained histolo- gic study revealed inflammatory infiltrate mainly consisting of Langerhans cells (Figure 4). Immuno- histochemical examination showed positive CD68, protein S100, CD1a and negative CKAE1/AE3 (Figure 5). Bone scan was indicated to discard other skeletal and extra-skeletal lesions. No evidence of other bone lesion was detected. Based on examinations LCH was diagnosed and confirmed. The patient was remitted with the pediatric oncology specialist and treated with chemotherapy and is in follow-up with no signs of side effects (Figure 6). In March of 2020, no new lesions have been observed since his last treatment.
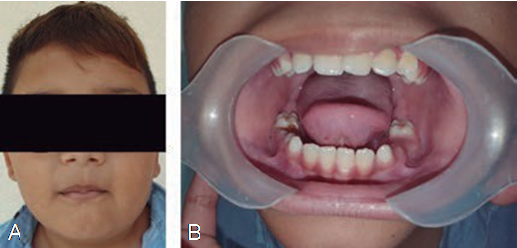
Figure 1 First clinical examination. (A) Facial view on the first visit, (B) Normal clinical appearance of intraoral tissues.

Figure 2 Left mandibular oblique radiograph. Well-defined ovoid radiolucent image is observed in the left mandibular angle.
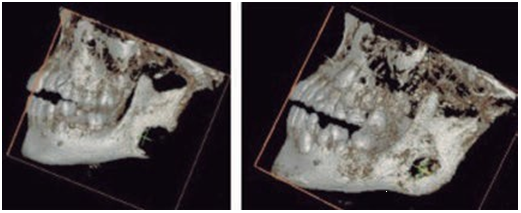
Figure 3 Tomography with 3D reconstruction left lateral view. (A) A well-defined hypodense image measuring 2.3 x 2.4 cm is observed in the left mandibular angle, compatible with an osteolytic lesion (pre operative). (B) Bone regeneration is observed at the edge of the left mandibular angle secondary to chemotherapy, 8 months after diagnosis.
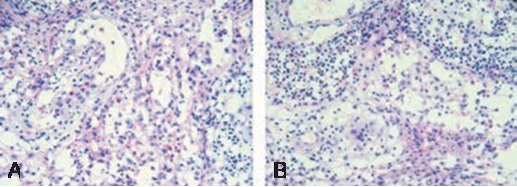
Figure 4 (A) Histopathology examination demonstrate a diffuse infiltration of mononuclear cells that resemble histiocytes, these cells have indistinct cytoplasmic borders and rounded or dentate vesicular nuclei, typically a variable number of eosinophils are interspersed between the cells with a histiocytic appearance histiocytes (haematoxylin-eosin). (B) Plasma cells and lymphocytes are observed along with areas of hemorrhage, all supported by a stroma of collagen fibers (haematoxylin-eosin).
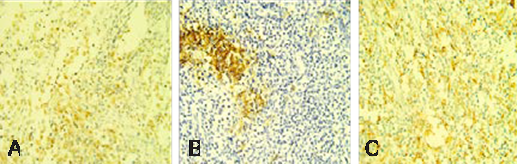
Figure 5 Immunohistochemical staining showing reactivity for (a) S-100, (b) CD1a, (c) CD68 positivity (x20).
Discussion
LCH is an inflammatory myeloid neoplasia of unknown etiology characterized by the proliferation and accumulation of Langerhans cells in a variety of organs, and a wide range of clinical manifestations (4). The incidence of oral involvement is approximately 70-90%, including intraosseous lesions, bleeding and swelling of gingiva, periodontitis-like lesion, dental mobility that can result in tooth loss (6,10,16).
In this case, an 8-year-old male presented a tumor in the left mandibular angle without any other organ involved. The maxilla and mandible are the most affected bones, founding different forms of lesions, a solitary intra-bone lesions, multiple alveolar lesions, with bone sclerosis and alveolar lesions with bone neoformation (19). The maxillary bones lesions could be manifestations of other diseases like odontogenic cyst, periapical lesions, metastatic neuroblastoma, infrabony hemangioma, fibrous dysplasia, epidermoid cyst, giant cell granuloma, Ewing’s sarcoma (23). Additionally, to the clinical findings is important to request imaging studies, histological studies and always confirmation by immunohistochemical tests.
Treatment depends upon the severity and progression of the clinical signs and symptoms, include observation for spontaneous regression in skin only LCH lesions or can be treated topical corticosteroids, a solitary lesion without involvement of risk organs can be treated with surgical curettage and intralesional corticosteroids injection, solitary lesions that involve risk bone areas or organs need a combined treatment of surgical curettage and chemotherapy, or radiotherapy, topical injection of steroid and systemic steroid therapy, in patients with multisystem LHC the treatment is more aggressive and combination of chemotherapy, radiation, corticosteroids therapy (17). The patient presented was treated with chemotherapy for 25 weeks, with a good response to the treatment.
The prognosis of LCH is related to the number of organs affected, the age of the patient, evidence suggest that the younger the patient is, the worse the prognosis, and response to initial therapy. Skin lesions tend to spontaneously resolve within months, and children with singlesystem involvement (single system LCH) tend to have better outcomes than those with multisystem involvement. The reactivation and permanente consequences (diabetes insipidus, orthopedic alterations, neurodegeneration) can occur at any age (9,10).
Because LCH is a rare disease is commonly mistreated, in this reported case it shows the clinical presentation involving mandible bone and how important is early diagnosis. Therefore, it is necessary that dentists are aware of this pathology and most importantly standardize clinical examination for detection of any abnormality, since they are frequently the first clinicians that could detect the first signs of LCH. We recommended as an initial study always an orthopantomography and in case of observing a suspicious image of bone pathology that does not coincide with the clinical examination, medical evaluation refer to the maxillofacial surgeon, who is the appropriate specialist to analyze the case and a perform, if necessary, a biopsy. In this case the tomography images did not match with another common pathology for the age, sex of the patient, clinical and medical data, therefore the maxillofacial surgeon suspected a neoplastic pathology.
Conclusion
The differential diagnosis of LCH can sometimes be difficult due to rather nonspecific manifestations, however oral manifestations are frequently the first and unique manifestations. It is important to create awareness among dentists as they could be the first clinicians to identify LCH. It is imperative to perform a correct examination clinical and medical interrogation thus avoid misdiagnosing or missing the first signs of this malignant histiocytic disease as well as other lesions with the possibility of malignancy. A recommended biopsy of all bone lesions symptomatic in the jaws is mandatory when it is not clinically associated with other dental pathology or trauma.

