











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
Dentistry professionals are in daily contact with many different types of dental materials, either during patient care or laboratory work. Such materials contain potential allergens that can potentially trigger an allergic reaction, which may impact everyday activities. It is crucial to understand how allergies come to be, given that they affect approximately 25% of the population in developed countries. In the United States of America (USA) alone, 54% of the population has had at least one allergic reaction. Importantly, the prevalence of allergy seems to be on the rise (1). An allergy can be defined as an abnormal and exaggerated immune reaction that occurs when an exogenous substance is recognized as an allergen, to which other people do not normally present a reaction (2). The term "hypersensitivity" refers to an excessive or inadequate immune response to environmental antigens, usually non-pathogenic, that causes tissue inflammation and organic malfunctions (3,4,5,6,7).
Hypersensitivity reactions were described by Gell and Coombs in 1963 and classified into four distinct clinical and immunological manifestations: types I, II, III, and IV (8, 9,10,11,12,13,14). Type I, II, and III reactions are rapid (from minutes to a few hours after re-exposure to an antigen), whereas type IV reactions require 24 to 48 hours to manifest, so they are referred to as delayed hypersensitivity reactions (8-9,14).
According to recent studies, the incidence of allergic reactions to dental materials has been increasing. Some of these materials include local anesthetics, latex, cement, acrylics, and adhesives (15,16,17,18,19,20). For example, latex gloves can cause allergic dermatitis (15). Allergic dermatitis repre- sents approximately 30% of environment-related occupational dermatoses (21). Many of the materials mentioned above are mixed with acryla- tes that contain inhibitors (e.g., hydroquinone), activators (e.g., tertiary amines), crosslinking agents (e.g., formaldehyde, responsible for inflammatory allergic reactions in patients with acrylic dentures), and initiators (e.g., benzoyl peroxide), which have been shown to be sensitizing substances (17-18,22,23,24).
It is important to address food and drug allergies, given that there has been cross-reactivity between certain foods and latex and certain foods and some medications (25,26,27,28,29,30,31,32). In dentistry, the use of a wide variety of materials has increased the frequency of allergic reactions during consultations (33-34).
This research may be useful for the development of appropriate measures in the work environment since the development of allergic manifestations can affect the professional and personal life of dentists. The study aimed to determine the prevalence and characteristics of the different kinds of atopy present in dentists working in Costa Rica.
Materials and methods
Bibliographic research
A search and analysis of the literature related to the subject was made using PubMed and Google Scholar, as well as databases available at the University of Costa Rica (UCR) Library System for Documentation and Information (SIBDI). The search keywords that were used included: alginate, allergies, allergic, allergy, asthma, atopy, chlorhexidine, conjunctivitis, cross-reactivity, dental materials, dental stone, dentists, dermatitis, dermal, dermatological, drug reactions, food allergies, health care worker, hypersensitivity, immune system, latex, latex-fruit syndrome, lidocaine, local anesthetics, medications, methacrylate, prevalence, pathophysiology, and rhinitis.
Study population
The study population consisted of a cohort of 664 dentists surveyed at the academic congres- ses organized by the College of Dental Surgeons of Costa Rica (CDSCR) and the Academic Congress of Dentistry Faculty of the UCR in 2016. The dentists had to be duly incorporated into the CDSCR, and they completed a self-reported questionnaire for data collection (care was taken to ensure that each applicant answered the survey only once). The surveys were handed out and collected at each of the congress events, which were held all around the country, and were, therefore, a representative sample of all dentists in Costa Rica.
Survey instrument
The survey instrument was applied as a physical questionnaire to the participating subjects. It was reviewed and corrected by an allergist, immunologist, and biostatistics specialist. This questionnaire was validated through a pilot study (unpublished data). Informed consent was needed for the formal application of the questionnaire, and was approved by the Scientific Ethics Committee of the UCR (resolution VI-6209- 2014, session N281, September 24, 2014). The questionnaire was registered at the Vice-Rectory of Research of the UCR, under the code 440-B5-
376. The CDSCR granted the approval and assis- tance permit to collect the necessary information of dentists at different academic congresses that were carried out in 2016. All participating subjects consented to participate.
The questionnaire collected data such as demographic information, history of exposure to dental environments and dental materials, familial and personal history of allergic disorders, and descriptions of allergic manifestations to foods, medicines, and dental materials.
Statistical analyses
A descriptive cross-sectional study with inferential analysis was carried out based on surveys conducted in 2016 of dentists. The prevalence of allergies to different materials, medications, and foods was evaluated.
The statistical methods used were the crossing of variables, frequency distributions, and comparison of the means based on the analysis of variance (ANOVA). The statistical analysis was carried out using the Statistical Package for the Social Sciences version 13.0 and Microsoft Excel. An ANOVA was used to test the following hypothesis:
H0: The averages in the populations are equal.
H1: At least one of the averages is different.
Since there were two distributions of nominal and ordinal variables, the homogeneity test of the Kolmogorov Smirnov statistic was performed. This tests whether two groups come from populations with the same distribution. The Students t-test was used to test for 95% confidence in the following hypothesis of the difference in the averages:
H0: The difference in the percentage of prevalence in atopy is equal to 0.
H1: The difference is different from 0.
Results
A cross-sectional study was performed on 664 out of the 5,223 dentists incorporated in the CDSCR. The average age of the dentists was 37.5 years (95% CI), ranging from 20 to 78 years, with a median age of 35 years. No statistically significant difference was found between the mean ages of males and females (39 and 36.8 years, respectively) (Table 1).
Depending on which university the dentists attended, there was a statistically significant difference regarding age (p=0.0001). Dentists who graduated from the UCR had a higher average age than all the other university graduates (see Table 2).
The average time of exposure to the dentistry environment was determined as 16 years (95% CI). When compared, age and time of exposure to dentistry-related environments had a high and positive correlation of 0.742 (p=0.0001), indicating that as age increases, so does the time of exposure.
About a third of the dentists (36%) reported having a chronic illness, with dyslipidemia being the most common, followed by arterial hypertension, and obesity (Figure 1). If the dentists were younger than 35 years, there was a 30% prevalence of some chronic illness, while those older than 35 years had a 45% prevalence of illness; this difference was statistically significant (p=0.0001).
Dentists reported having a history of allergies before studying dentistry in 39% of cases, a prevalence of 42% in females and 32% in males. This difference was statistically significant (p=0.01). The most common allergic reactions reported were rhinitis (25.9%), dermatologic manifestation (20.9%), and asthma (10.1%). Almost two-thirds (61%) of the dentists surveyed reported having first-degree relatives who had presented some type of allergic reaction, with rhinitis being the most common (Figure 2 and Figure 3). These two factors, a history of prior allergies, and familial allergy history, had a low yet positive correlation with the development of allergies to food, medicines, and dental materials (Table 3).
The dentists surveyed reported a prevalence of 20.9% for food allergies, 14% in males, and 24% in females. This difference was statistically significant (p=0.005). The types of foods that produced the greatest number of allergic manifestations were lactose, shrimps, tomatoes, and pineapples. Gastrointestinal manifestations were more prevalent when associated with lactose, but the other foods mentioned primarily caused an allergic dermatitis reaction. All manifestations appeared within the first 120 min of food ingestion.
Medication allergies were reported by 19% of dentists. Penicillin and nonsteroidal anti-inflammatory drugs (NSAIDs) were reported to be more likely to induce allergic reactions. Female dentists had a 21% prevalence of medication allergies, whereas males reported only a 14% prevalence, resulting in a statistically significant difference (p=0.03). The reactions reported always occurred within the first 120 min of exposure, with the most common being dermatologic manifestations.
Allergies to dental materials were reported in 26% of dentists, with a statistically significant difference by sex (p=0.0001), with a 16% prevalence in males and 31% prevalence in females. Most allergic reactions were caused by latex and acrylics. Dermatitis was the most common manifestation reported, always within the first 120 min of exposure.
Table 1 Group distribution according to sex and age between Dentists in Costa Rica 2016.
| Quinquennial age groupsq | Sex | - | - | - | Total | - |
|---|---|---|---|---|---|---|
| - | Women | - | Male | - | - | - |
| - | # | % | # | % | # | % |
| 20-24 | 20 | 4.4 | 9 | 4.4 | 29 | 4.4 |
| 25-29 | 91 | 20 | 39 | 19.2 | 130 | 19.7 |
| 30-34 | 112 | 24.6 | 40 | 19.7 | 152 | 23.1 |
| 35-39 | 100 | 21.9 | 46 | 22.7 | 146 | 22.2 |
| 40-44 | 50 | 11 | 19 | 9.4 | 69 | 10.5 |
| 45-49 | 23 | 5 | 10 | 4.9 | 33 | 5 |
| 50-54 | 20 | 4.4 | 9 | 4.4 | 29 | 4.4 |
| 55-59 | 20 | 4.4 | 11 | 5.4 | 31 | 4.7 |
| 60-64 | 14 | 3.1 | 12 | 5.9 | 26 | 3.9 |
| 65+ | 6 | 1.3 | 8 | 3.9 | 14 | 2.1 |
| Total | 456 | 100 | 203 | 100 | 659 | 100 |
Source: Survey instrument applied to dentist cohort in 2016.
Table 2 Mean graduation age from different universities between Dentists in Costa Rica.
| University | Average age (years) | N | Standard deviation |
|---|---|---|---|
| UCR | 41.3 | 343 | 12.1 |
| Latina | 32 | 144 | 6.1 |
| Ulacit | 32.6 | 109 | 5.7 |
| Veritas FACO | 35.8 | 37 | 6.5 |
| Foreign | 49.1 | 9 | 11.1 |
| UIA | 35.2 | 16 | 3.1 |
| Total | 37.5 | 658 | 10.7 |
Source: Survey instrument applied to dentist cohort in 2016.
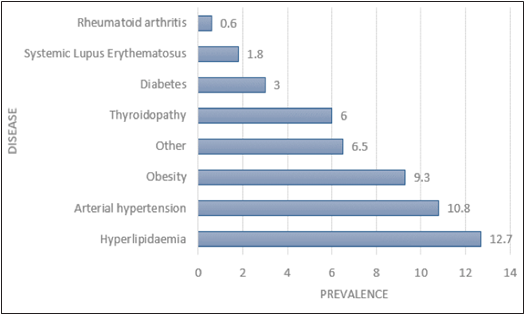
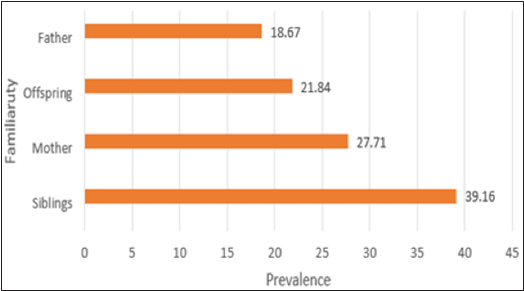
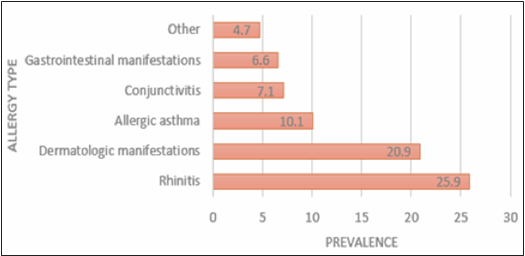
Table 3 Correlation of allergy prevalence between Dentists in Costa Rica 2016.
| - | - | Prior allergy | Food | Drugs | Dental materials | Chronic Illness | Allergic familial history |
|---|---|---|---|---|---|---|---|
| Prior allergy | Bilateral significance | 1 | 0.310 | 0.241 | 0.259 | -0.004 | *- |
| - | correlation | - | 0 | 0 | 0 | 0-916 | *- |
| - | N | 664 | 657 | 662 | 664 | 664 | *- |
| Food | Bilateral significance | 0.310 | 1 | 0.243 | 0.255 | 0.073 | 0.163 |
| - | correlation | 0 | - | 0 | 0 | 0.061 | 0 |
| - | N | 657 | 657 | 657 | 657 | 657 | 657 |
| Drugs | Bilateral significance | 0.241 | 0.243 | 1 | 0.096 | 0.141 | 0.000 |
| - | correlation | 0 | - | - | 0.014 | 0 | 0.176 |
| - | N | 662 | 657 | 662 | 662 | 662 | 0 |
| Dental materials | Bilateral significance | 0.259 | 0.255 | 0.096 | 1 | 0.016 | 0.133 |
| - | correlation | 0 | 0 | 0.014 | - | 0.685 | 0 |
| - | N | 664 | 657 | 662 | 664 | 664 | 664 |
| Chronic Illness | Bilateral significance | -0.004 | 0.073 | 0.141 | 0.016 | 1 | *- |
| - | correlation | 0.916 | 0.061 | 0 | 0.685 | - | *- |
| - | N | 664 | 657 | 662 | 662 | 664 | *- |
| Allergic familial history | Bilateral significance | *- | 0.163 | 0.176 | 0.133 | *- | 1 |
| - | correlation | *- | 0 | 0 | 0 | *- | - |
| - | N | *- | 657 | 662 | 664 | *- | 664 |
Source: Survey instrument applied to dentist cohort in 2016.
Discussion
This study aimed to determine the prevalence and type of allergies in Costa Rican dentists. Data was collected regarding allergic reactions associated with food, drugs, and dental materials and analyzed, taking into account the hereditary factors and associated systemic conditions that may influence an immune response.
The immune system can recognize the bodys own cells, as well as pathogens and toxins, once it has been exposed to them. Moreover, it can defend against these external aggressions, meaning re-exposure will elicit an immune response (2,35).
Immune responses can be classified as innate and acquired (8,35,36,37), depending on the type of reactions triggered (2,8,36,37,38,39). Innate responses are immediate but nonspecific reactions, meaning that the same mechanism is used against all pathogens (5,36,37,38,39,40). Acquired responses involve a different unique reaction to each pathogen. However, these are not immediate, in contrast to innate reactions, which are immediate (2,5, 8,36,39-40). The acquired immune system has four specific characteristics: antigenic specificity, antigenic diversity, immunologic memory, and the ability to recognize what is exogenous (5,36, 39-40). Antigens are molecules that stimulate the immune system to generate antibodies or initiate a cell-mediated response (5). Antibodies, also known as immunoglobulins (Ig), are produced by mature B lymphocytes (plasma cells). Antibodies bind antigens for protection against pathogens, and there are five types: IgA, IgD, IgE, IgG, and IgM (5).
Hypersensitivity reactions can be classified depending on the cells and the chemical mediators involved, as well as the delay and severity of the reaction. Type I hypersensitivity is a fast reaction mediated by TH2-lymphocytes, IgE, and mast cells, which leads to the release of pro-inflammatory cytokines (6,14,45-46). It occurs a few minutes after the binding of the antigen to an antibody in patients previously sensitized to the antigen (14,45,47-48). The immediate hypersensitivity of type I is a systemic response to residual proteins, a reaction classified as an allergy (14,45). This type of hypersensitivity can occur as a systemic or localized reaction (6,37). Local reactions differ depending on the entry point of the allergen, localized skin swelling, nasal and conjunctival secretions, and asthma (6,37). Anaphylaxis is a systemic reaction caused by the release of histamine and other mediators (48-49). It has a sudden onset and lasts less than 24 h, producing life-threatening symptoms such as laryngeal edema, angioedema, obstruction of the lower airway, hypotension or circulatory collapse, vomiting, diarrhea, and urticari (14,48,49,50,51).
A type I hypersensitivity reaction has two well-defined phases: an early-stage that presents vasodilation that increases vascular permeability and smooth muscle spasm or glandular secretion, and a delayed reaction that occurs without additional exposure to the allergen and where eosinophils, neutrophils, basophils, mast cells, and lymphocytes infiltrate the tissue, causing destruction (7,37,47-48,52). The early-stage symptoms are observed between 5 and 30 min (up to 1-2 h) after antigen exposure, and they tend to disap- pear after 60 min. In contrast, the delayed phase begins within 2-4 h and lasts up to 24 h, lasting up to several days (6,37,48,53). Patients with these characteristics have more elevated serum levels of IgE and IL-4 producing TH2-lymphocytes than the general population and a positive family history of allergy (37). Typical examples of type I hypersen- sitivity include asthma, rhinitis, anaphylaxis, some types of dermatitis and conjunctivitis, gastrointestinal reactions, latex allergy, food allergies, and drug allergies (14,15,16,17).
Atopy refers to the genetically and environ- mentally determined predisposition to develop clinically expressed disorders, including allergic rhinitis, atopic dermatitis, eczema, and allergic asthma, regulated through immune phenomena in which many cells (i.e., mast cells, eosinophils, and T lymphocytes) and associated cytokines, chemokines, and neuropeptides play a role (58). Atopy is considered a hereditary condition that predisposes a patient to series of IgE-mediated responses and alterations in cellular immunity and vascular reactivity (59-60). The surveyed dentists indicated that 39% had allergies prior to dental school, with a statistically significant difference by sex (p=0.01). This can be considered high compared to what Torres Fernan (60) reported in his study, that is, 10 to 15% of the world population suffe- red from an allergic disease. The results obtai- ned in this investigation share the same behavior as described by Risenga et al. and Thong et al., where females have a higher prevalence of allergic reactions than males (61,62). According to Ngo et al., this is because females have greater humoral and cellular activities in immune reactions than males (63).
Some factors increase the risk of developing an allergic reaction, such as gender, tobacco smoke, poor hygiene, familial or personal history of allergies, respiratory viral infections, some endotoxins, pets, environmental pollutants, and indoor or outdoor allergens (25,26,27,28,29,30,31,32,33,34,64). Several prospective studies have confirmed that obesity is a risk factor for asthma or allergic disease. Many of these studies also considered the dietary factors and level of physical activity, demonstrating that asthma is specifically associated with obesity and not with a lack of physical activity or type of diet (30,38,39,40,41,48,49,50,51,64). Patients with obesity have a higher prevalence of asthma, thus having an increased risk of having exacerbated inflammatory reactions (41,48,49,50,51,64). More than a third (36%) of the dentists interviewed suffered from a chronic disease. The most reported chronic diseases were dyslipidemia and obesity, which tended to appear more frequently as age increased. In an investiga- tion conducted in Canada, Chen et al. also reported that obesity affects the occurrence of allergies. They found that adipokines and cytokines secreted by the adipose system intervene in the immune response, decreasing tolerance to different agents that may attack the body (48,65).
In a study of 3,327 children aged 2-14 years carried out in Wuhan, China, obesity increased the prevalence of allergic rhinitis and atopic derma- titis, especially in girls, suggesting a difference depending on weight and sex (64). In this study, a low positive correlation was found between having a chronic illness and developing food allergies (r=0.073), medication allergies (r=0.141), and allergies related to dental materials (r=0.016).
A history of family allergies is an important risk factor for the predisposition of allergic reactions (7). Approximately 12-15% of the general population is at risk of suffering from an allergic disease. In contrast, there is a 19% risk of having an allergic reaction if a parent suffers from some type of allergy. If both parents are atopic, their offsprings risk is 19%-42%, whereas if both parents have the same allergic disease, the risk increases to 42%-72% (17,36,66). A statistically significant positive correlation was observed between the allergic antecedents prior to starting dental school and having relatives with a history of atopy (61%). One study managed to relate the R576 allele with greater IgE values in patients with relatives with atopy (67). Gershwin et al. mentio- ned an increase in the predisposition of aller gic disease when there is a personal and family history of allergies (19). In an analysis conducted by Cooke and Van der Veer, cited by Zubeldia (43), 504 individuals with allergic disease were compa red with 76 non-allergic controls. They found that half of the people with allergies had a family history of allergies, while in the second group, only 14% had such a family history. All of the above findings are in agreement with our study results, where the prevalence of allergy in a first-degree relative has a low and positive correlation that is statistically significant with the development of allergies.
Drugs can cause type I reactions (mediated by IgE) and type IV reactions (mediated by T cells) (62,68-69). The immediate reactions are more related to antibiotics and NSAIDs, which can result in urticaria, angioedema, bronchospasm, or even cardiovascular collapse. In contrast, delayed reactions are more related to anticonvulsants, sulphas, and some medications for AIDS treatment (19,20,21,22,68-69). Medication-related allergies were also reported by some dentists, particularly to penicillin and NSAIDs. Beta-lactam antibiotics are the main cause of medication-related allergic reactions, followed by NSAIDs. There is no clear reason why some medications cause more allergies than others, which may be related to the frequency of use in the general population (43). According to Zubeldia (43), Gómez (70), and Yang (36), beta-lactam antibiotics are the main cause of allergic reactions to medications (approximately 50% of cases), followed by NSAIDs, which represent 39% of reactions (43). The incidence of allergy to penicillin in the general population is 1-10% (43), while the prevalence ranges between 10-12% (71,72,73,74). This study found a significant difference by sex (p=0.03) in cases of penicillin allergy reported in dentists, with a higher prevalence of cases in females (21%) than in males (14%); Albin et al. (72) found that females were associated with a higher rate of reported allergy cases, although Ponvert et al. (74) postulates that age, sex, and personal history of atopy are not significant risk factors for developing hypersensitivity to beta-lactam antibiotics.
About 26% of dentists in this study reported having an allergic reaction to dental materials. Dermatitis was the most frequent, and even more so when associated with the use of latex gloves. Globally, the prevalence of latex allergy in the general population has been reported to range between 6-12%, while in health professionals, it can range between 3-22% (75,83). According to Amasekera et al. and others, the time in contact with different dental materials is a risk factor for developing allergies to these materials (84,91). The more dentists come into contact with materials, the higher the probability of sensitization and, therefore, the higher the likelihood that an allergic reaction will occur. Ahmed et al. (92) claimed that frequent exposure to latex products is significantly correlated with a higher prevalence of allergy to latex gloves in health workers. According to Boyce et al., other materials such as acrylic generate a localized immune response that is almost always limited to the contact area of the skin (93). The possibility of contact dermatitis that is not mediated by IgE should always be considered. It is often believed that the allergic reactions that health workers have are, in general, due to latex. Specific tests such as patch testing must be carried out, given that the allergen could be due to another reason (88). Mikov et al. (89) showed that not all reactions are due to latex, but in some cases, acrylate macromolecules can cross through latex, resulting in an allergic reaction. The reaction to acrylics is due to direct contact with the skin or mucosa and is attributed mostly to the non-polymerized monomers in these materials (94-95). The monomers can cause clinical cases of dermatitis and even neuropathies in the fingers or hands (56, 59).
Pimentel (86) indicated that dentists are a population at risk of developing allergies due to frequent contact with dental materials that can trigger type I hypersensitivity reactions mediated by IgE. Some studies showed that 40% of individuals with sensitivity to latex also have sensitization to different types of fruit. This cross-reactivity is known as latex-fruit syndrome (96-97). The main types of fruit related to this type of allergic reaction are bananas, avocados, kiwifruit, grapes, passionfruit, pineapples, peaches, papayas, walnuts, tomatoes, and cherries (65,96,97,98,99,100,101,102). It is characterized by an immediate hypersensitivity reaction to two different allergenic sources: latex and fruit. The main allergens responsible for this cross-reaction are Hev b5, Hev b6, and Hev b7, which are proteins related to the protection system of the latex plant (Hevea brasiliensis) and are also contained in avocados, papayas, pineapples, tomatoes, and other vegetables (98,102,103,104).
In this study, a low but positive correlation for dentists was found between allergy to dental materials and foods (r=0.255). About a fifth (20.9%) of the dentist population reported some type of food allergy, whereas the prevalence of food allergies varies from 2% to 8% in the general population (66). Females reported having the most allergic manifestations. According to the Spanish Society of Allergology and Clinical Immunology 2005, the foods that result in an allergic reaction most frequently are fruit, nuts, seafood, eggs, and milk (105). Similarly, dentists reported that lactose, shrimps, pineapples, and tomatoes caused the most allergic reactions. The most common allergic reaction was urticaria. Furthermore, Scurlock and Burks mentioned that urticaria is probably the most common reaction (106).
There seems to be an increase in the number of allergic reactions to food, medications, and dentistry-related materials. This could be associated with increased antigenic exposures in dental environments and cross-reactivities or repeated exposures to medication, as advocated by Baldo and Pham in 2013 (69). These findings may be helpful for developing improved health policies for dental professionals. Future research should include a larger population sample.
Conclusions
In conclusion, there is a directly proportio- nal relationship between age, time of exposure to dental environments, and the risk of developing allergic conditions to dental materials (26% in this study). A low and positive correlation was observed between the presence of a chronic illness and the predisposition to develop an allergic reaction to food, medicines, and dental materials. There was a low and positive correlation between the presence of allergies in a first-degree relative and the prevalence of allergies between dentists. There was a low and positive correlation between the development of allergies to dental materials and allergies produced by the intake of some foods such as pineapples, tomatoes, and seafood. The main adverse reactions reported in dentists due to exposure to dental materials, medicines, and/or food were gastrointestinal, skin, and respi- ratory problems.

