











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
In recent years, the patient demand for aesthetic restorations has led to the development of new composite resin technologies. Despite advances in resin-based composite materials, there are lingering disadvantages that affect the longevity of composite resin restorations. Polymerization shrinkage, incompatibility of thermal expansion, resistance to erosion and abrasion, marginal leakage, and recurrent caries, are the most frequently reported problems of composite restorations (1,2,3). The most common problems with composite resins as a restorative material in daily clinical practice are the difficulty of controlling the depth of cure and polymerization shrinkage (4). To overcome these problems, it is recommended that composite resins be applied in 2mm thick layers (5). However, it is known that layering and curing of composite resins of limited thickness is time consuming, the bonding between the layers is weakened, and the risk of contamination to these applied layers is increased. This situation adversely affects the mechanical and physical properties of the material used (6,7).
Recently introduced bulk-fill composite resins include the possibility of applying a thickness of up to 4 to 6mm, while reducing problems related to polymerization depth and polymerization shrinkage shown by conventional composite resins (8). In bulk-fill composite resins, alternative and more reactive photo initiators are used to improve polymerization depth, and to increase the translucency of the material. Further, the filler content is reduced and the size of the filler particles is increased (9). In addition, some chemical modifications have been made to reduce polymerization shrinkage stress, such as increasing the molecular weight of the monomers in their contents, adding new stress-relieving monomers, and including methacrylate monomers (10). The innovative polymerization initiation system results in shortened light curing time and increased depth of cure. These materials combined with a high filler content have resulted in low polymerization shrinkage, allowing the application of thicker resin composite layers (10,11).
In addition, preheating of resin-based composites has been introduced to improve the handling properties of composite resins. Preheating reduces the viscosity of composites and increases their flowability. This method reduces microleakage and void formation by providing more impermeable marginal adaptation (12). Preheating composites can be recommended for each type of composite restoration. This method is recommended, especially in deep cavities of posterior teeth, where good adaptation and polymerization should be more sufficient in deeper layers of the material (13). Temperature has a significant effect on the efficiency of polymerization. The higher mobility of monomers caused by the increased temperature facilitates crosslinking between polymer chains and results in a high conversion degree. This results in improved mechanical and physical properties of preheated composites, such as increased fracture strength and surface hardness (12).
Microhardness tests, which are known as a reliable method, are used to determine the depth of cure of resin-based composites (14,15). The Knoop hardness test and Vickers hardness (VHN) test show a strong correlation with the tests used to determine the degree of conversion. However, it is known that the International Organization for Standardization’s (ISO) evaluation of the scrapping method overestimates the depth of cure of composites (14,15,16). The ratio of microhardness values from bottom to top surface (B/T) is taken as an estimate of completion of polymerization at a given depth from the light source. When the bottom microhardness measurements of a resin-based composite is 80% or higher than the top surface measurements of the same sample, the composite is sufficiently cured for clinical use (15,16).
The purpose of this study was to obtain more information about bulk-fill resin composite materials by analyzing the effect of different bulk-fill composites and one microhybrid composite resin on the basis of Vickers surface microhardness and depth of cure. There is not much data in the existing literature regarding the preheating of bulk-fill composite resins. Based on these data, the aim of the present study was to investigate the effect of preheating on bulk-fill composite resins in respect to microhardness and depth of cure by examining both preheated and nonheated (at room temperature) immediately after polymerization (baseline), and again after 24 hours. The following null hypotheses were considered in our study:
There is no difference between the microhardness values of nonheated and preheated composite resins.
There is no difference between the bulk-fill composite resins and the microhybrid composite resin in terms of microhardness and depth of cure.
There is no difference between the microhardness of composite resins when measured at baseline and after 24 hours.
Materials and methods
Three commercial bulk-fill resin-based composite materials and one microhybrid resin- based composite were evaluated in this study. Admira® Fusion x-tra (AFX) is an ormocer-based, high viscosity, bulk-fill composite resin; SDR Plus (SDR) and Estelite Bulk Fill Flow (EST) are low viscosity, bulk-fill resin composites; G-ænial Posterior (GP) is a urethane dimethacrylate- based microhybrid composite. The manufacturer information and properties of the composite resin materials used in the study are shown in Table 1.
All 80 (n=10) samples were produced using a Teflon mold measuring 2mm thick and 8mm in diameter. Half of these, including samples from each composite group, were subject to preheating, while the other half were prepared at room temperature (24±1°C). The U.S. Pharmacopoeia has defined room temperature as 20-25 degrees Celsius (17). The temperature change was controlled by the ventilation system of the laboratory. Room temperature was measured with a digital thermometer (Digital Thermometer, Atago Co., Tokyo, Japan). Composite syringes or capsules were preheated in groups with the aid of a composite heating device (Ena Heat, Micerium S.p.A. Avegno GE, Italy) in T2 mode at 55°C for 10 minutes (13). The exposure time of the capsule or syringe composites in the heating device was equal for all samples. For this purpose, syringes, as many as the number of capsules, were kept in the device. All preheated composite materials were placed in the Teflon mold within 45 seconds after being removed from the heating device (18). The Teflon mold, glass table, and hand tools were heated to 37°C before composite resins were placed (18). The samples were polymerized with a LED light device (Elipar S10, 3M Espe, St. Paul, MN, USA) with a high intensity 430-480nm wavelength and 1200 mW/cm² light power for 20 seconds. The power output of the light device was checked with a radiometer (LED radiometer, SDI Limited, Victoria, Australia) after each use. In order to standardize the distance of light reaching the samples, the LED device was placed in full contact with the glass layer on the upper surface, and polymerization was achieved.
All samples were polished with 600-800- 1000-1200 grit silicon carbide sand paper, respectively, in circular motions with finger pressure for 3 minutes (15). Silicon carbide paper was used to standardize and eliminate the oxygen inhibition layer. Polishing was done by a single operator.
A microhardness tester (HMV-G Micro Vickers Hardness Tester, Shimadzu Corporation, Kyoto, Japan) was used to determine the VHN. The samples were then placed on the table of the test device, and a 100-gram (980.7mN) load was applied to the sample on the table with a dwell time of 15 seconds. The VHN was measured from the top and bottom surfaces of the samples at three points distributed equally with the help of millimetric paper. After each measurement, the samples were kept in distilled water in a separated and carefully numbered arrangement. VHN values were measured after preheating immediately after the samples were produced, and after being stored for 24 hours in distilled water at 37°C in an oven (Memmert UN 110, Schwabach, Germany). The microhardness measurements obtained were recorded. The values on the top and bottom surfaces were calculated by taking the average of the three measured points.
The depth of cure values of the composite resins were obtained by calculating the hardness ratio for each sample. This ratio was calculated by dividing the average VHN values of the bottom surface of each sample by the mean of the top surface (VHN) according to the following equation: Depth of cure (hardness ratio)=VHN bottom surface/ VHN top surface (15).
Table 1 The manufacturer information and properties of the composite resin materials used in the study.
| Material | Manufacturer | Classification | Composition | Filler content ((wt%-vol%)) | Filler size | SHADE/LOT # |
|---|---|---|---|---|---|---|
| G-ænial POSTERIOR | GC Dental Products Corp, Aichi, Japan | Micro HDR Hybrid | UDMA, Strontium glass, lanthanoid fluoride, Silica glass, Fumed silica, Pigments, Catalysts | 77/65 | 16-17 µ | A3 /1909121 |
| Admira® Fusion x-tra | VOCO, Cuxhaven, Germany | ORMOCER® | Ormocer matrix, Ba-Al-Si-glass, Silica nanoparticles, SiO2, glass ceramic | 84/69 | 20-40 nm | Universal / 1807658 |
| Estelite BULK FILL Flow | Tokuyama Dental Corporations, Tokyo, Japan | Bulk-fill flowable | Bis-GMA, Bis- MPEPP, TEGDMA, Supranano spherical filler Silica, Zirconia, Ytterbium trifluoride. | 70 /56 | 200nm | A3 /093E00 |
| SDR Plus | Dentsply Sirona, Konstanz, Germany | Bulk-fill flowable | Modified UDMA, Bis-EMA, TEGDMA, Ba-Al-F-B-Si-glass, Sr-Al-F-Si-glass | 68/45 | Mean 4.2 µ | Universal / 079161 |
UDMA: Urethane dimethacrylate. Bis-GMA: Bisphenol A-glycidyl methacrylate. Bis-MPEPP: Bisphenole A ethoxylate dimethacrylate.
TEGDMA: Triethylene glycol dimethacrylate. Bis-EMA: Ethoxylated bisphenol-A dimethacrylate. Ba-Al-Si-glass: Barium-Aluminium-Silicon- glass. SiO2: Silicon dioxide. Ba-Al-F-B-Si-glass: Barium-Aluminium-Fluorine- Boron-Silicon-glass. Sr-Al-F-Si-glass: Strontium-Aluminium- Fluorine-Silicon-glass.
Statistical analysis
The data were analyzed using the IBM SPSS V23 software. The normal distribution compliance was examined through the Shapiro Wilk test. The generalized linear model method was used to examine the effects of material, process, surface, and time main effects and interactions on microhardness values. Further, the Duncan test was used for multiple comparisons. The analysis results are presented as mean and standard deviation for quantitative data. The level of significance was taken as p<0.05.
Results
A descriptive analysis of the VHN values and hardness ratios is summarized in Table 2. This table includes top and bottom surface VHN values, baseline and 24-hour measurements, and hardness ratios of all groups. In addition, the mean and standard deviations of nonheated and preheated VHN values are presented in Figure 1. VHN values of the preheated and nonheated groups showed statistically significant differences in all groups (p<0.001). While microhardness increased after the preheating procedure in AFX, EST, and SDR, the VHN values decreased in GP.
The mean and standard deviations of the VHN values are shown in Table 3. A statistically significant difference was found among the baseline VHN values of all the groups (p<0.001). The highest VHN value was obtained from the AFX material, while the lowest was obtained from the SDR material. There was also a statistical difference between all groups in the measurements after 24 hours. AFX showed the highest VHN value, while SDR showed the lowest VHN value. However, there were no difference noted between the baseline and 24-hour VHN values in SDR and GP. The VHN value of EST after 24 hours increased, while that of AFX decreased.
The mean and standard deviations of the hardness ratios are presented in Table 3. AFX and EST showed the highest ratios, while there was no statistically significant difference between AFX and EST (p>0.001). Further, there was no statistically significant difference between GP and SDR (p< 0.001).
According to multiple comparisons, this study revealed a statistically significant effect of material-process-time-surface interaction on VHN values (p<0.001). While the highest VHN value was obtained at the baseline top surface of the AFX with preheating, the lowest average value was obtained at the 24-hour bottom surface of the nonheated SDR sample. The comparison of microhardness values between material, surfaces, process, and time are shown in Table 4.
Table 2 Descriptive analysis of VHN values and hardness ratio.
| - | Material | Mean±SD Microhardness at baseline | - | - | Mean±SD Microhardness at 24h | - | - |
|---|---|---|---|---|---|---|---|
| - | - | Top | Bottom | Hardness ratio at baseline | Top | Bottom | Hardness ratio at 24h |
| - | GP | 29.1 ± 2.0 | 28.8 ± 2.9 | 0.994 ± 0.117 | 31.3 ± 2.1 | 29.1 ± 2.1 | 0.932 ± 0.078 |
| Non-heated | AFX | 44.8 ± 3.7 | 44.9 ± 3.9 | 1.011 ± 0.129 | 40.2 ± 3.8 | 40.6 ± 2.6 | 1.017 ± 0.102 |
| - | EST | 34.7 ± 2.4 | 35.9 ± 2.4 | 1.035 ± 0.057 | 38.1 ± 1.7 | 38.5 ± 1.2 | 1.013 ± 0.046 |
| - | SDR | 22.9 ± 1.9 | 21.6 ± 1.3 | 0.943 ± 0.041 | 22.6 ± 0.8 | 21.4 ± 0.9 | 0.950 ± 0.039 |
| - | GP | 29.6 ± 1.8 | 27.7 ± 3.0 | 0.939 ± 0.117 | 28.9 ± 2.0 | 27.4 ± 2.3 | 0.948 ± 0.050 |
| Preheated | AFX | 48.6 ± 5.6 | 47.8 ± 3.9 | 0.991 ± 0.102 | 43.0 ± 5.8 | 42.8 ± 2.8 | 1.011 ± 0.149 |
| - | EST | 37.3 ± 1.7 | 39.3 ± 2.3 | 1.053 ± 0.060 | 37.5 ± 0.6 | 38.0 ± 1.7 | 1.012 ± 0.047 |
| - | SDR | 24.3 ± 0.8 | 23.3 ± 1.6 | 0.958 ± 0.064 | 22.8 ± 0.7 | 22.7 ± 0.9 | 0.997 ± 0.040 |
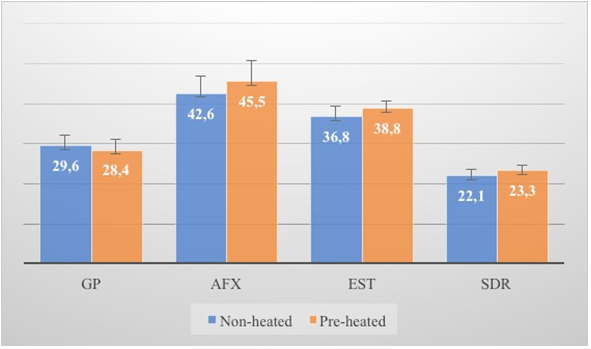
Table 3 The mean and standard deviations of VHN values and hardness ratios
| Material | Mean±SD Microhardness at baseline | Mean±SD Microhardness at 24h | Mean±SD Hardness ratio |
|---|---|---|---|
| GP | 28.8 ± 2.5ᴮ | 29.2 ± 2.5ᴮ | 0.953 ± 0.094ª |
| AFX | 46.5 ± 4.5ᴰ | 41.6 ± 4.0 | 1.007 ± 0.118ᵇ |
| EST | 36.8 ± 2.8ᴱ | 38.0 ± 1.4 | 1.028 ± 0.054ᵇ |
| SDR | 23.0 ± 1.7ᴬ | 22.4 ± 1.0ᴬ | 0.962 ± 0.051ª |

 A-H: No difference between interactions with the same letter. a-b: No difference between groups with the same letter.
A-H: No difference between interactions with the same letter. a-b: No difference between groups with the same letter.
Table 4 Correlation analysis of microhardness values.
| - | Test statistics * | Sd | p |
|---|---|---|---|
| Material | 5433.236 | 3 | <0.001 |
| Process | 17.07 | 1 | <0.001 |
| Time | 16.885 | 1 | <0.001 |
| Surface | 2.340 | 1 | 0.126 |
| Material * Process | 32.048 | 3 | <0.001 |
| Material * Time | 84.330 | 3 | <0.001 |
| Material * Surface | 14.147 | 3 | 0.003 |
| Process * Time | 13.335 | 1 | <0.001 |
| Process * Surface | 0.008 | 1 | 0.928 |
| Time * Surface | 0.217 | 1 | 0.642 |
| Material * Process * Time | 5.174 | 3 | 0.159 |
| Material * Process * Surface | 1.842 | 3 | 0.606 |
| Material * Time * Surface | 2.529 | 3 | 0.470 |
| Process * Time * Surface | 0.492 | 1 | 0.483 |
| Material * Process * Time * Surface | 1.116 | 3 | 0.773 |
*Wald Chi-square test statistic, Sd: Degrees of freedom.
Discussion
In this study, the microhardness and depth of cure of preheated and nonheated bulk-fill composite materials were compared with each other and with a microhybrid composite resin. While the preheating process increased the VHN values of AFX, EST, and SDR, only in the GP group did VHN values decrease after preheating in this study. At the same time, the VHN values of preheated and nonheated groups showed statistically significant differences in all groups. Therefore, the first null hypothesis, that there is no difference between microhardness values of nonheated and preheated composite resins, was rejected.
Increased temperature decreases viscosity, increases free radical mobility, and increases the frequency of conflicts between the active group and free radicals. As a result, the degree of conversion is improved. This is expressed by the increased microhardness of the composite resin (18). Such findings can be multifactorial. One of these factors is the difference in the chemical composition of the resin monomer, which affects the surface microhardness of composite resins (19). The monomer compositions of all composite resins used in this study were different from each other.
Studies have stated that there is a correlation between monomer conversion and hardness values (18,20). On average, it has been reported that composite resins can achieve 50% to 70% monomer conversion at room temperature (18). During polymerization, monomer conversion begins the moment the material is exposed to light. As the reaction proceeds, the viscosity of the composite resin increases through the formation and growth of polymer chains, resulting in reduced molecular motion. It prevents the polymerization process from being completed as the movement of the molecules in the glassy state becomes limited with increasing viscosity (21,22). Conversely, preheated composites display increased monomer mobility as a result of higher thermal energy, resulting in less viscosity and improved molecular motion (21,23). Yan et al. (20) stated that the microhardness test is more sensitive than Fourier transform infrared spectroscopy in identifying small changes in monomer conversion after 24 hours. In their study, Daronch, et al. (24) reported that the monomer conversion of preheated composites is superior to that obtained with resin composites polymerized at room temperature. In our study, a positive correlation was found between the preheating process and the microhardness of the bulk-fill composite resins (Figure 1).
Eliades et al. (25) found that hardness values increased as inorganic filler content increased. It was also stated that the morphology and distribution of filler particles, particle shape and density, monomer type and ratio, crosslinking of polymers, and the degree of conversion can be responsible for the variance in surface microhardness values between different materials tested (19, 26). In the present study, statistically significant differences were obtained between the tested composites in terms of surface microhardness and depth of cure. Therefore, the second null hypothesis was rejected. According to the results of the statistical analysis, while the highest microhardness value was obtained from the AFX material and the lowest microhardness value was obtained from the SDR material, statistically different microhardness values were observed among all material groups. In the current study, varying microhardness values of the tested materials may be due to the difference in the chemical composition of the organic resin matrix and the amount of filler.
AFX material has a high filler content (84% by weight) compared to other composite materials evaluated, and it is produced using ormocer technology. The ormocer matrix contains inorganic-organic copolymers instead of conventional monomers such as BisGMA or TEGDMA, which are usually used in dental resins, and are synthesized by the sol gel process. These materials contain inorganic silanized filler particles and inorganic- organic co-polymers (27). Also, in ormocers, the use of larger monomer molecules has been indicated to reduce polymerization shrinkage and wear, resulting in less monomer leaching (28).
It has been reported that flowable bulk-fill composites show lower surface microhardness values than high-viscosity bulk-fill composites (29). The viscosity of the composite is related to the type of resin matrix (30). Bis-GMA has a strong intramolecular hydrogen bonding of hydroxyl groups, and it is considered the most viscous and least flexible monomer among dental resin monomers. UDMA contains a hydrogen bond between the amine and carbonyl groups and is also a viscous resin monomer. However, the viscosity of UDMA is much lower than that of Bis-GMA due to weak hydrogen bonding (31). The most viscous Bis-GMA is also the least flexible; UDMA and TEGDMA are the least viscous (30, 32). Paralleling this information, the present study showed that the EST group containing Bis-GMA had higher microhardness values than GP and SDR samples. Similar to our findings, a recent study comparing the microhardness values of four bulk-fill composite resins at different light intensities concluded that the flowable SDR showed the lowest microhardness values (33). The SDR group had the lowest filler content (68%) by weight, while it contained modified UDMA and TEGDMA. The difference between the microhardness values obtained from these groups may be related to the amount and type of filler. Also, the significant difference between the surface microhardness values of AFX and SDR bulk-fill composite materials can be attributed to the difference in monomer viscosity.
Both direct and indirect methods have been proposed to evaluate the depth of cure, which correlates well with the degree of conversion and microhardness of resin composites. However, other methods, such as optical microscopy and scraping tests, have been shown to overestimate the depth of cure (16,34). Flury et al.’s study on six composite resins compared the depth of cure for bulk-fill composite materials with the depth of cure determined by the Vickers microhardness profiles. They stated that the ISO 4049: 2000 method (scraping method) calculates more than the depth of cure determined by Vickers hardness profiles (16). Therefore, curing efficiency was evaluated by measuring both the top and bottom surfaces to obtain the Vickers microhardness value of the samples in this study. All the top/bottom surface hardness ratios were found to be above 0.8. The highest hardness ratios were obtained in AFX (1.007) and EST (1.028), while GP (0.953) and SDR (0.962) showed lower values. These results showed sufficient polymerization across the sample with a thickness of 2mm (23,35). The values obtained in the study are consistent with previous studies investigating the depth of cure of composite resins (10,13). As a result, they can be sufficiently polymerized at 2mm in both bulk-fill and conventional composite materials regardless of the composite type and the temperature of the material and are suitable for clinical use under experimental conditions.
The top surface microhardness value of any resin composite material is expected to differ from the values obtained from the bottom surface due to the difference in monomer reactivity and filler/matrix refractive index mismatch (36). In this study, no statistically significant surface effect on microhardness values was found (see Table 4). In our study, the thickness of the samples was designated at 2mm, which is the same thickness as the composite restorations applied in clinical situations using the layered placement technique (22,30). This can be explained by the fact that bulk-fill composite resins, due to their high translucency, allow photopolymerizing light to penetrate deeper and cause more polymerization of the resin composite monomers (1). However, the hardness ratio of the GP group, which is a microhybrid composite, was not different from that of SDR, which is a bulk fill composite. GP has the highest filler particle size among the composite groups evaluated in the study. Since some studies have shown that translucency increases when filler particle size increases, it is well known that smaller filler particles emit more light than larger filler particles. Such light scattering reduces the amount of incident light transmitted through the composite resin and can, thus, adversely affect the physical and mechanical properties of the resin composites (37). Surface hardness will improve over time after the light-curing period, contributing to post-irradiation polymerization (38). There are conflicting reports regarding polymerization kinetics after light curing of composite resins. While some researchers have stated that polymerization speed reaches its maximum value within the first few minutes after irradiation (22,35), others have reported that a significant part of the reaction could occur during the first 24 hours (39).
In this study, microhardness measurements were calculated immediately after polymerization and at 24 hours after polymerization. Alshali et al. (26), in their study that measured the top and bottom microhardness of bulk-fill and conventional composite resins at baseline and after 24 hours, showed that all materials tested exhibited a significant increase in microhardness values after 24 hours. It is thought that the most important contribution to the post-irradiation polymerization of Bis-GMA-based resin composites is provided by the amount of TEGDMA co-monomer (40). In the present study, the microhardness values of EST, which contain Bis-GMA and TEGDMA, increased statistically above the baseline after 24 hours. However, there was no difference between baseline and 24-hour VHN values of GP and SDR. Interestingly, the VHN values of AFX decreased after 24 hours. Therefore, the third null hypothesis was partially rejected. It is likely that other factors, such as the monomer content, the initial conversion degree of the materials, and the presence of free radicals, can also importantly affect the microhardness of the materials being evaluated (26).
Although preheated composite resins exhibit an increased degree of transformation, light curing is not immediately applied because clinically, the material must be placed in the cavity and formed. During this process, preheated composites cool down, and their properties change accordingly. Daronch et al. (41) found that the surface temperature of composite resins decreased by 35-40% at 40 seconds after preheating to 60°C. In another study, researchers stated that after 45 seconds, the average temperature drop varied between 5.2°C and 8.7°C (18). In this study, the temperature of the composite during placement was not recorded. However, a more important issue is that the reduced viscosity of the preheated composite materials provides better adaptation to the cavity walls.
The current study has some limitations. Studies on several mechanical properties of preheating bulk-fill composite resins applied with 4mm or 6mm bulk layers can also be considered. Kelic et al. compared the microhardness values of low viscosity and high viscosity bulk-fill composites with samples of 2mm and 4mm thickness, and found no difference between the microhardness values (30). However, in this study, the researchers considered standardizing the specimens by applying different composite resin materials in a single layer to obtain uniform thickness. At the same time, the specimens were polymerized only from the top side to mimic the clinical situation. This means that polymerization has less effect on the behavior of the material, and therefore, the filler particle type and content (percentage) play a greater role (42). Additionally, long-term clinical studies are recommended to evaluate the clinical performance of these materials.
Conclusion
According to the results of this in vitro study, the microhardness values of the baseline and the 24-hour measurement differed according to the materials. All tested materials reached a 2mm thick curing depth (according to microhardness measurements). The preheating procedure increased the microhardness values of all bulk-fill composites. The composition of the tested composite resins affected their microhardness values.

