











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkINTRODUCTION
The Palatal Fissure or also called the Palatine Cleft, is one of the anomalies or craniofacial malformations of congenital origin with the highest incidence worldwide, primarily affecting the society of low or low economic resources, occurring in one of every 500 to 700 live births.
It occurs more frequently in the female sex and does not keep or is related to the mother's age. This malformation can affect the back of the palate (only the uvula) and give the appearance of a fish tail; to prolong and affect both the soft palate and the hard palate. And it is because of the absence of the union or fusion of the lateral processes of the palate, with each other, or with the nasal septum or with the primary palate, during the embryonic development of the fetus, in intrauterine life.
The alveolus palatal lip fissure or known as FLAP, is a congenital malformation that occurs between the area of the mouth and lips, since it is the result of the lack of union of the central and lateral processes of the face during embryonic development, being congenital and multifactorial etiology. Part of the factors that are related to this malformation is the low feeding of folic acid, as well as the excess ingestion or consumption of alcoholic beverages, tobacco or drugs consumed during the period of pregnancy or embryonic development. Children born with this condition have a not very optimal quality of life and emotionally are affected, as are the parents of children (1).
According to Tirador, Madera, & González (2), indicate that of the facial skull malformations that the human being suffers most frequently is the cleft lip and cleft palate, due to the prevalence of these conditions vary according to the geographical situation, for Asians its dependence is 1/300, for Africans it is 1/2,500 and in European countries, such as France, it is 1/700 births.
In a Latin American collaborative study of congenital malformations (ECLAMC) in the period 1982-1990 a global rate for cleft lip 10.49×10000 was found, calling attention to the high frequency in Bolivia (23.7), Ecuador (14,96) and Paraguay (13.3), probably because their populations are mixed with Indian race. However, lower rates were found in Venezuela (7.92), Peru (8.94), Uruguay (9.37) and Brazil (10.12), all ×10000 inhabitants that are explained by the mixture with the black race of their populations (3).
There is a significant number of investigations that seek to determine specific genes, how they are inherited, and the causes of the ethnic differences detected. Teratogens that directly affect the embryo have also been identified, such as drugs and toxins for agricultural and industrial use. These noxas can also affect parental gametes and therefore the rest of their offspring. Maternal age and diseases during pregnancy seem to play a role in their pathogenesis (4).
As mentioned earlier, this anomaly is a congenital malformation, which corresponds to a structural alteration that occurs from the moment of the patient's birth, and depending on the structures that it encompasses or affects, will alter the vital functions such as: food, hearing, phonation, swallowing and even breathing it. Therefore, it is the duty of the Professional Health Personnel to try to help solve these great inconveniences that affects both babies and their parents; to later integrate the patient into their social environment, thus improving their lifestyle and making it totally normal.
The literature indicates that the Palatal Fissure is of multifactorial origin, including several etiological factors, such as: the consumption of alcohol, tobacco and drugs; self-medication (anxiolytics, barbiturates, anticonvulsants); infections caused by bacterial and viral diseases, such as measles, toxoplasmosis, rubella; also a nutritional deficiency, and radiation; being considered teratogenic or environmental agents.
This anomaly presents between 10 and 40% of genetic base and family history, where it indicates that parents who have had children with this malformation have a high percentage of risk of suffering from this disorder again. It is important to note that the Palatal Fissure can go hand in hand with another Syndrome, such as the Trisomy of Chromosome 13 (Bartholin-Patau Syndrome), or also Pierre Robín Syndrome, which has a triad: micrognathia, cleft palate and glossoptosis; causing severe damage.
We can point out that one of the characteristics of these patients is that they have a remarkable malnutrition, and this is caused by the difficulty to feed, because they cannot exert enough pressure to suck the breast or bottle milk, because it has an almost zero ability to perform the suction reflex by the permanent communication of the oral cavity, with the nasal cavity; resulting in liquids or food entering the larynx, causing the risk of causing a broncho aspiration.
Given this need, it is necessary to develop a device or apparatus capable of momentarily sealing the palatal fissure, in order to prevent the diversion of food and restore the sucking reflex in the nursing patient.
In the current titration work, a clinical case of a 5-month-old female patient is described and analyzed, presenting a Unilateral Palatal Fissure (right side) who attended the National Maxillo-Facial Rehabilitation Foundation (FUNARMARF) and that it has considerable malnutrition (3.69 kg) due to the inability to perform the Suction reflex. Therefore, it was made and designed an acrylic plate called Obturator, with the main objective of avoiding oral-nasal communication, facilitating suction, swallowing and a considerable improvement in your daily diet.
We conclude by pointing out that the use of a device capable of sealing the Palatal Fissure is effective, since it acts as an adjunct in the breastfeeding and feeding of the child, allowing to improve the nutritional status of these patients.
CASE REPORT
5-month-old female patient, from a family with low socio-economic status, without medication administration, or systemic disease, with a family history of a craniofacial malformation; Presents Unilateral Palatal Fissure of the right side, even without eruption of temporary pieces. The mother expressed as a reason for the consultation "My daughter cannot take the tit and I need help." The physical examination can show that the patient presented malnutrition, due to the difficulty in feeding, due to a bad or almost zero suction capacity (3.69 kg of weight).
It has a unilateral hard and soft palate fissure, with cleft lip (right side) Figure 1, Figure 2, Figure 3, Figure 4, Figure 5.


Figure 2 Front Image. Cleft palate (right side), depression of the nasal wing on the same side. Braquifacial biotype. Lateral image presents slight concave profile.

Figure 3 Upper jaw. Complex palatal fissure, hard palate and soft palate, with unilateral cleft lip. Compressed right jaw

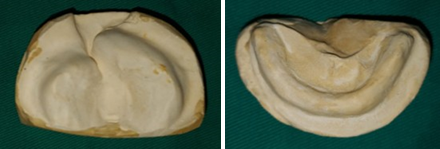
Figure 5 Superior Model. Complex Palatal Fissure. Maxilla Compressed (right side). Bottom Model No eruption of temporary pieces.
Several actions or treatments were determined to treat the present case:
Palatal Fissure Shutter (mediate).
Correct position of the mother at the time of breastfeeding of the child (immediate).
Surgical surgery, to correct the cleft palate and cleft lip (mediate).
Early maxilofacial orthopedic treatment (mediate).
The prognosis of the treatment provided is favorable. But it should be noted that, like any other dental treatment, it must go to the mother's help and collaboration, with the correct use of the device at the time of feeding her baby, with the main objective of recovering and stimulating the sucking reflex in her, thus favoring her daily diet.
SHUTTER DEVELOPMENT PROCESS
Once the Informed Consent is signed by the mother, where she is informed and indicated about the treatment to be provided to her baby, and accepts to voluntarily participate in the procedure and elaboration of an apparatus called “Three- dimensional Palatal Fissure Shutter”, the whose main objective is to restore the sucking reflex at the time of taking the bottle, favoring and facilitating its daily feeding. In addition to stimulating the closure of the palatal processes and guiding the growth of the segments, in the future to obtain better surgical results.
IMPRESSION TAKING
The first step in the development of our Shutter, was the choice of the individual cuvette, which is self-curing acrylic and should be according to the measure of the patient's mouth. The impression was taken with Addition Silicone (Putty), from the Exaflex brand, due to the advantages offered by the material, such as ease of handling, good dimensional stability, longer working time, rapid polymerization and also the consistency of the same, preventing the material from entering beyond the palatal fissure Figure 6.
It is important to note that the material should not be handled with latex gloves, because they can alter its properties and modify the impression. Therefore, nitrile gloves should be worn, or if they are not available to them, the material can be mixed without gloves.
To proceed with the impression, the baby sat on the mother's legs and proceeded to introduce the tray with the impression material already mixed. Polymerization was expected and the cuvette was removed Figure 7.
Once the impression was taken, the work model was obtained, making the respective emptying with stone plaster (Type III), taking into account that 1 hour was expected because the addition silicone eliminates oxygen and can lead to that air bubbles form in the final model Figure 8.



DELIMITATION OF THE PROSTHETIC AREA
After obtaining the work model, with a pencil the area to be acrylated was delimited and designed (delimitation of the prosthetic area). In addition, with the help of a lighter, melted wax was added at the end of the palatal fissure, to prevent the acrylate from covering the deepest area of the fissure. Relief zones were also performed.
It should be noted that to design the Shutter, it was decided to do something ingenious and different, where 2 wires were added that would help hold and maintain it in the correct position, thus fulfilling its function, to restore the pediatric patient's suction reflex and to it time to avoid possible broncho aspiration of the device. In addition, a special hat was adapted to hold the Shutter in the mouth Figure 9.
ACRYLATED
Before performing the acrylation, insulation was placed on the surface of the work model, so that we can remove it and prevent it from adhering to it. Then the preparation of the acrylic was carried out in a dappen glass; once it enters the plastic stage a ball was formed with the hands and with the help of 2 glass tiles (with insulation) a thin and uniform layer of acrylic was created, which was placed on the model and the folds of 0.9mm orthodontic wire Figure 10.
It is important to emphasize that we must try to obtain a good polish and shine of these acrylic devices, since in addition to favoring the retention and adhesion of the Obturator to the surface of the palate, it also prevents and decreases the accumulation of bacterial plaque in the roughness, therefore it does not have an unpleasant smell and/or possible lesions at the level of the patient's oral cavity Figure. 11.
SHUTTER ADAPTATION
To complete the preparation, we proceeded to test and adapt the Shutter in the patient's mouth, noting that there is no discomfort. Existing literature and evidence mention us that we must make a hole in the front part of the obturator, in order to pass a dental floss as a precaution and, if necessary, be able to remove it easily.
As already mentioned, this Shutter had lateral wires which gave it stability and managed to maintain an indicated position. Those wires must be attached to a cap, but they were replaced by something ingenious and of our authorship. Although the literature does not mention this method, a baby hat was used and modified; to which 2 brooches (of female bra) were added and cooked on each side, which will help hold the device while the baby is feeding, thus recovering or stimulating the sucking reflex and at the same time improving its feeding Figure 12, Figure 13.

Figure 9 Delimitation of the prosthetic area and relief zone formation, plus double 0.036 orthodontic wire to adapt the Shutter.

Figure 10 Shutter acrylation and Placement of the 0.8 mm orthodontic wire folds on each side and add a little more acrylic with the drip technique, in order to hold them.



DISCUSSION
The Palatine Fissures are a real inconvenience for society in general, since they affect worldwide, 1 in 700 live births, with those of low socioeconomic status being the most affected; and given the main difficulty that these patients present to be fed (either directly from the mother's breast or through bottles), due to the inability to exercise or perform the suction reflex, which will give way to a poor state of nutritional health of the infant (severe malnutrition), stunted growth and despair on the part of the parents.
Given this need and problem it is important to be able to offer and provide an immediate treatment that helps to solve it. This is achieved thanks to the help of the Obturator, which seals the palatal fissure by reestablishing and returning the suction capacity in it, and in addition to preventing the passage of liquids into the nostril and subsequently avoiding an accident, such as bronchoaspiration (5).
Bedón & Villota in 2012 (6) they point out in their published article, that “with respect to the treatment of unilateral fissures, sealing plates were used, whose only benefit was to improve the patient's diet. The analysis of the position of the segments in the planes of the space, was overlooked and the repercussion was made notice to the dental eruption that was crowded".
In the article published by Bravo Rivera, Muñoz, & Torres in 2015 (7), about preoperative orthopedics in fissured children, where they treated a 4-month-old patient with Bilateral Palatal Lip Fissure, to which a Shutter was made, along with a nasal guardian Indicating that the sealing plate also "allows the separation of oral and nasal cavities, aimed at minimizing the penetration of food into the nasal cavity, reducing adverse effects on the nasal mucosa and facilitating feeding".
Olivares & Morales in 2012 (8) we emphasize in his work, that Gallardo M in 2002, conducted a study based on the benefits of employment, and the non-employment of these palatine shutters. Finding a very important difference in the body mass of patients at 6 months. Favoring in this way in their nutritional health status. In addition, (5) indicate that in this way it helps to solve multiple problems in feeding and breathing in these pediatric patients, also recommending the use of Shutters.
CONCLUSIONS
The present research work is concluded by pointing out that the Three-dimensional Shutter is an effective treatment, mainly in patients who present with a craniofacial malformation, such as the Palatal Fissure, since given the difficulty of being able to exert the sucking reflex in the infant, proceeded to place the device or apparatus in the oral cavity and its effectiveness was verified, observing that the pediatric patient was able to feed correctly.
It should be noted that after the placement of the Palatine Obturator on the gingival mucosa of the upper jaw of the patient it was possible to achieve a completely hermetic closure around the nipple of the bottle, being able to exert sufficient negative intraoral pressure, stimulating and recovering the capacity or Suction reflex of our patient.
The initial body weight of the patient was 3.69 kg (8.1lbs) and after 28 days using the respective Shutter a marked improvement was seen, gaining almost twice its weight (2.5kg more), having a current weight 6.19 km (13.6lbs); in this way obtaining totally favorable results in the nutritional status of it, being an excellent adjuvant in the feeding process in these patients.
Finally, it should be noted that thanks to the use and placement of the device in the oral cavity, a closure of the buconasal communication was achieved, preventing the passage or deflection of food and liquids into the nostrils, preventing inconvenience from occurring such as nasal regurgitation, asphyxiation, air intake or possible broncho-aspiration when feeding the patient.

