











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkINTRODUCTION
Early childhood caries (ECC) is a chronic multifactorial infectious disease and one of the most common diseases in children (1). Despite preventive practices to prevent tooth decay, ECC continues to be a worldwide health problem (2). In the last 6 months, the Turkey Statistical Institute data (2019) have revealed an age range of 0-6 years in group- treated diseases, with oral and dental diseases ranking as one of the top five diseases at 6.4%. A review by Baltaci et al. (3) documented the prevalence of early childhood caries in Turkey at between 40.7% and 69.8%.
The American Academy of Pediatric Dentistry (AAPD) and the American Dental Association (ADA) recommend that children have their first dental visit (FDV) within six months of eruption of the first primary tooth and no later than 12 months of age (4). Early visits are important for the child to gain familiarity with the dental clinic and dentist, as this reduces dental anxiety in young children. The FDV of children is also an important opportunity for the parents to address their own anxieties and fears about dental care, as these can be inadvertently transmitted to the child (5).
Early visits for infants and their families offer a chance to educate and inform parents about the oral health of their children. The caregivers can be provided with dental guidance in the form of information on infant oral hygiene and oral habits, home-based and office-based fluoride therapies, dietary counseling, caries risk evaluations, and prevention of dental injuries (6). Infancy dental examinations can diagnose dental disease early, thereby increasing the possibility of using conservative nonsurgical caries management techniques, including remineralization and fluoride varnish for early lesion arrest (7). Conservative treatments can delay or prevent any need for surgical intervention, thereby minimizing the risk of adverse outcomes by eliminating or postponing more extreme and resource-intensive behavior management techniques, such as moderate and deep sedation and general anesthesia (8).
Early dental visits are expected to improve oral health and reduce the child’s future dental risk. Untreated dental problems increase in severity and intensify the need for more extensive and costly treatment; therefore, timely intervention has great potential to reduce the costs of dental treatment (9). One of the most important aims of the FDV is to diagnose and control tooth decay, which can often be observed shortly after the tooth eruption (10). In Turkey, 19% of children start school with dental caries in their permanent dentition. An average of 4.5-5 caries occur in the deciduous teeth in the 6-8 year age group, and the prevalence exceeds 80% (11).
Despite the importance of early dental visits, the FDV age is usually over 1 year old (12,13,14,15). The primary purpose of this study was to present the parameters of age, reasons for the visit, behavioral response, and caries status at the FDV.
The secondary aim was to evaluate the factors affecting these parameters.
MATERIALS AND METHODS
Ethical approval was obtained for this study (Decision number: TUTF-BAEK 2020/122), and 325 children who applied to Trakya University, Faculty of Dentistry, Department of Pediatric Dentistry for their FDV between December 2019 and March 2020 were included. A signed informed consent form was obtained from the parents of each child. Children who had not undergone any dental procedure from another dentist were also included in the study. Children who had any mental/physical disability were excluded from the study.
Parents were asked to fill out a questionnaire consisting of 3 sections that requested sociodemographic information about the family, information about the child’s medical history and brushing habits, and specific information about the FDV. Information about family income was a part of the sociodemographic information section. Family income less than 2000 Turkish Lira (TL) was classified as low, between 2000 and 6700 TL was classified as medium, and more than 6700 TL was classified as high. The age of the children at the FDV, the person who brought the child to the clinic, and the main reasons for the FDV were questions included in the section on specific information about the FDV.
Children were clinically examined with a curved probe and dental mirror under a dental reflector light. Two examiners evaluated the caries status of each child to record the decayed-missing- filled-teeth (DMFT) scores (16). The study group included ages with both primary and mixed dentition, so the summation of both primary (dmft) and permanent (DMFT) values was also reported and presented as dmft/DMFT. This summed value was also used for linear regression analyses. The behavioral responses during the first examination were evaluated according to the FBRS (17) in the patients who were over 3 years of age.
STATISTICAL ANALYSIS
Statistical analyses were conducted using the IBM SPSS 21.0 program. Beside descriptive statistics, a stepwise linear regression test was used to determine factors affecting the dmft/ DMFT score, age, and behavioral response at the FDV. A p value less than 0.05 was accepted as statistically significant.
RESULTS
The mean age of the children was 7.20±2.78 years (range: 0.46-13.06 years); 166 patients (51.1%) were female and 159 (48.9%) were male. The age and sex distributions of the patients are shown in Table 1. The majority of the children belonged to families with middle (57.2%) and low (35.2%) monthly incomes. The education levels of the parents are presented in Table 2.
The person who brought the child to the clinic was most frequently the mother (55.4%), followed by the father (24.6%), and then both parents (17.8%). Only 2.1% of the patients were brought to the clinic by other relatives. The parents of 94.8% of the patients were alive and living together, whereas 4.9% of the parents were divorced and 1 patient (0.3%) had lost his father. The majority of the children (56.9%) came from outside the city, followed by patients from the city center (28.9%) and districts (14.2%).
In total, 216 patients (66.5%) were referred by other dentists and 14 (4.3%) by pediatricians, while the remaining 95 reported that they came to our clinic by their own preference (29.2%). The reasons for the patients coming to the clinic are shown in Figure 1. The most common reason was dental caries in 33.5% of the patients, followed by toothache (29.5%), and abscess formation (12.3%). The mean dmft, DMFT, and dmft/DMFT values of the patients were 6.7±4.7; 1.4±2.0 and 8.1±4.4, respectively.
Twenty (6.2%) of the children reported a history of systemic disease which are listed in Table 3. Overall, 65.5% of the children used antibiotics before 2 years of age. In 92.5% of these children, the reason for antibiotic use was upper respiratory tract infections. The most commonly used antibiotic was penicillin, in 74.6% of the cases, followed by cephalosporins, in 19.7% of the cases. In total, 93.8% of the children used antibiotics between the ages of 2 and 8 years. In 84.3% of those children, the reason was upper respiratory tract infections, and 95.1% of the cases used penicillin.
Behavior assessment results according to the FBRS are shown in Figure 2. The majority of the children showed positive behavior (46.7%). The information about the toothbrushing habits of the patients and the use of toothpaste are presented in Table 4.
The regression analysis for the determination of factors that could affect the age of the first dental visit revealed that higher maternal education level (p=0.007) and higher dmft/DMFT score (p<0.001) were associated with a significant decrease in the age of admission.
The regression analysis for the determination of the factors that may affect the behavior scale indicated that a farther home to hospital distance (p=0.006) and a higher dmft/DMFT score (p=0.011) negatively affected the child’s behavior, while a higher age (p<0.001) positively affected the behavior.
The regression analysis for the determination of factors that could affect the dmft/DMFT score indicated a significantly lower dmft/DMFT score with increasing monthly family income level (p<0.001) and frequency of toothbrushing (p=0.027). In addition, patients with divorced parents (p=0.002) and those who came to the clinic on their own preference rather than being referred (p=0.006) had significantly lower dmft/DMFT scores.
Table 1 Age and sex distribution of the participants
| - | Female | Male | Total |
|---|---|---|---|
| Mean Age ± SD* | 7.48 ± 2.69 | 6.92 ± 2.85 | 7.20± 2.78 |
| <1 | 1 (0.6%) | 1 (0.6%) | 2 (0.6%) |
| 1-3 | 6 (3.6%) | 10 (6.3%) | 16 (4.9%) |
| 3-6 | 50 (30.1%) | 58 (36.5%) | 108 (33.2%) |
| 6-9 | 60 (36.1%) | 52 (32.7%) | 112 (34.5%) |
| 9-12 | 39 (23.5%) | 31 (19.5%) | 70 (21.5%) |
| >12 | 10 (6%) | 7 (4.4%) | 17 (5.2%) |
Percentages corresponds to the ratios in the column.
*SD: Standard deviation
Table 2 Education level of children’s parents (highest degree obtained).
| - | Mother | Father |
|---|---|---|
| Illiterate | 15(4.6%) | 3(0.9%) |
| Primary school | 147(45.2%) | 136(41.8%) |
| High school | 123(37.8%) | 140(43.1%) |
| University | 36(11.2%) | 44(13.1%) |
| Master/Doctorate | 4(1.2%) | 2(0.6%) |
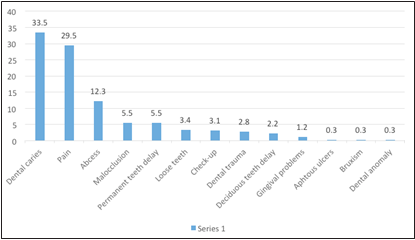
Table 3 Systemic diseases reported by children’s parents during FDV.
| Disease | N (%) |
|---|---|
| Epilepsy | 5 (25) |
| Asthma | 4 (20) |
| Anemia | 2 (10) |
| Throid diseases | 2 (10) |
| Other | 7 (35) |
| Total | 20 (100) |
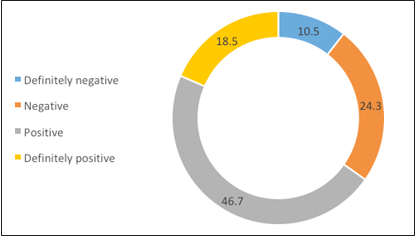
Table 4 Tooth brushing habits and toothpaste use among pediatric patients in FDV.
| Tooth brushing frequency | - |
| Never | 18(5.5%) |
| Once or Twice a week | 173(53.2%) |
| Once a day | 99(30.5%) |
| Twice a day | 35(10.8%) |
| Toothpaste usage | - |
| Yes | 294(95.8%) |
| No | 13(4.2%) |
| Toothpaste ingredient | - |
| Containing Fluoride | 170(57.8%) |
| Non-containing Fluoride | 48(16.3%) |
| Unknown | 76(25.9%) |
DISCUSSION
As in other medical branches, preventive dental methods have become important in today's health policy. The importance of early diagnosis and treatment of diseases that cannot be prevented is a universally accepted reality. For these reasons, the importance of early and regular dental visits cannot be denied.
In the present study, the mean age of FDV was 7.20±2.78 years, whereas other studies on FDV have reported mean ages between 3.79 and 7.90 years (12,14,18). The FDV of patients under the age of 1 year was reported in previous studies as between 0.63 and 8.00% of the population. In the present study, only 0.6% of the children were under 1 year of age. An FDV at less than 3 years of age was reported in 3.00-40.50% of the population in previous studies (13,19,20,21), whereas the rate was 5.5% in the present study. Other reports have stated that most of the children were aged between 6 and 9 years (12,19) or 3 and 6 years (13,15) at FDV. In the present study, 34.5% of the patients attending their FDV were between ages of 6 and 9 years and 33.2% were between the ages of 3 and 6 years, in agreement with the previous literature. However, these findings obviously indicate that we are quite far from the target in terms of early dental visits. In addition, in this study, we found that higher dmft/DMFT scores were associated with lower FDV ages. The increasing numbers of caries again clearly emphasize the importance of an earlier visit to the dentist.
In the literature, the most common cause of the FDV is dental caries or toothache. Studies reporting dental caries as the most common cause reported that 34.9-59.9% of the FDVs were due to caries (13,18,21). Studies reporting tooth pain as the most common cause reported that 33.1-34.9% of the FDVs were due to pain (12,14,15,20). These two reasons constituted 42.6-61.1% of the reasons for the FDV (12,14,15,20,21). In this study, the most common reason for the FDV was dental caries in 33.5% of patients, followed by toothache (29.5%), with these two reasons accounting for 64% of the total FDVs. Patients who attended our clinic for control purposes constituted only 3.1% of the total study group. In the literature, the group of patients who came for control purposes was typically between 2.6 and 54.3% (12,13,14,15,18, 20,21,22). The results of the present study show that the routine control examinations that we expect to see as the most common cause of FDVs constitute a very low fraction of applications, in accordance with the literature data.
In this study, the most common education level of both mothers and fathers was primary school. A similar study conducted by Sanguida et al. (19) reported a good overall education level of the parents, with 85% of them having completed high school and above, with most parents unaware of the FDV time, regardless of education level. However, Efe et al. (23) reported that mothers with a high educational level had children with more certain knowledge about oro-dental health, and 86.1% of the children of those parents said that they had learned to brush their teeth from their parents. In this study, higher maternal education level was associated with a significant decrease in the age of the FDV. This may reflect the fact that mothers with higher education levels are more likely to be aware of the control examination recommendations or to react earlier to lesions in the child's mouth.
This study showed that the most common systemic diseases were epilepsy (25%) and asthma (20%). Penicillin was used in 74.6% of the cases. Daou et al. (18) reported the most common medical problem as allergic/asthma (15.9%), followed by ear, nose, and throat problems (12.7%). Overall, 9.1% of the children had already taken antibiotic(s) (18).
In this study, the FBRS scores revealed that the most common behavior state of children was positive (46.7%). Alshahrani et al. (15) and Viswanath et al. (24) reported that approximately 39.67% and 80% of the children, respectively, showed positive behavior at the FDV. Viswanath et al. (24) attributed this high percentage to the assessment of the state of behavior during a non-invasive procedure. In the present study, increasing age was found to have a positive effect on the behavioral status, whereas increasing distance between the hospital and home and higher dmft/DMFT scores had a negative effect. The positive effect of age on behavioral status is already well known, whereas the negative effect of a long distance between the hospital and the home may reflect a decrease in the adaptability of the child after a difficult and tiring journey. Children with a high dmft/DMFT score may also have been exposed more often to frightening rhetoric about dentists as a result of their caries being noticed by their families and their neighbors.
The study by Efe et al. (23) reported that 77.5% of the children knew that they needed to brush their teeth after meals and before going to bed. Hatipoglu et al. (25) reported that only 51.3% of the children knew about the necessity of brushing their teeth at least twice a day, while Berk et al.(26) reported that 96.3% of the children knew this. Serious differences are therefore clearly evident between these studies in terms of consciousness about brushing and this is therefore reflected in the FDV. Gökalp et al. (27) reported children brushing their teeth at least twice a day and children never brushing their teeth as 30.1% and 9.4% of their study population, respectively. The same ratios were 10.8% and 5.5% in the present study; however, although most of the children brushed their teeth (94.5%), only a small fraction (10.8%) did so at the recommended frequency.
Only 29.2% of the children participating in this study came to our clinic by their own preference, without any referral. Daou et al. (18) reported that 74.1% of their child patients came without any referral. Most of the referrals we received were from other dentists, and we believe that this is due to the fact that our hospital is a tertiary center.
Mika et al. (14) reported a mean dmf/DMF index of 3.82 for the total analyzed pediatric population during the FDV. In this study, the mean dmft, DMFT and dmft/DMFT values of the patients were 6.7±4.7, 1.4±2.0, and 8.1±4.4, respectively. These values are quite high compared to the study conducted by Mika et al. (14), but the average age at FDV for our patients was 7.2 years, while it was 3.8 in the earlier study. This shows that resistance to dental visits is higher in Turkey.
We also reported a significantly lower dmft/ DMFT score as monthly income level of the family and as frequency of toothbrushing increased. In other studies investigating the effect of socio- economic situation on caries risk, poor socio- economic status has been shown to negatively affect oral hygiene and nutrition, thereby increasing the risk of caries and a low emphasis on oral hygiene (28, 29). One of the main obstacles to dental visits handled by our interviewees was the cost of dental treatments. Due to the absence of a national oral health policy in Turkey, an oral health delivery system is lacking (30). Implementing oral health policies, such as Early Head Start programs (31) and Access to Baby and Child Dentistry (ABCD) programs (32), may have the potential to increase access to care and to improve oral health.
Lack of knowledge about the primary teeth and the importance of preventive dental visits are another important issue to be taken into consideration. Mass media, school, and parents’ dental health education can make a significant contribution in terms of raising awareness about the importance of the FDV. Patients living in rural areas are also likely to face geographic remoteness, poor or no public transportation, and poverty; therefore, they could benefit from teledentistry to obtain basic information about oral health care (33).
CONCLUSION
According to the present study results, Turkish population is far from the ideal early dental visit age target. As the knowledge level increases, the dental visit age decreases, emphasizing the importance of community education. In order to take advantage of the early dental visit, stronger health policies should be implemented to reduce the age of the first dental visit.

