











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Resin composites offer improved esthetic properties, convenience and good chemical binding to the teeth but have several disadvantages including the development of secondary caries over time, fracture, discoloration and inadequate contour (1,2). Most failures occur many years after placement of the composite restoration and may result from secondary caries, fracture of restoration, tooth fracture, discoloration and breakdown in marginal integrity (3). In the case of a restoration failure due to such reasons, repairing only the defective portion instead of completely removing the existing restoration is a viable long-term solution and a safe and effective treatment strategy (4,5).
A major concern when repairing old and damaged composite restorations is whether the repair material bonds adequately to the existing restorations. Determining the type and composition of the composite resin in the tooth represents a challenge while repairing composite restoration in the dental clinic. Different companies have products with a variety of compositions and it is known that the type of resin used in these products is one of the main factors that affect the bonding strength during the repair process (6). In recent years, bulk-fill composites have been introduced as a novel addition to the existing portfolio, which can be applied with a greater layer thickness and are claimed to better adapt to the cavity due to their fluent structure and, eliminate the undesirable aspects of the layering technique such as air entrapment and contamination, and improve patient and physician comfort with ease of manipulation (7,8,9). However, there is a limited number of studies on the use of bulk-fill composites for repairing other composites in the clinical setting (10,11).
In parallel with the advances in composite resin systems, there have also been improvements in the light curing units used for polymerization. As a result of these developments, Light Emitting Diode (LED) light devices were introduced, offering better and more efficient polymerization in a shorter time compared to Quartz-Tungsten-Halogen (QTH) light devices (12). In a study using LED and halogen light devices, LED light device was shown to have superior properties in comparison to conventional halogen light device despite both having equivalent light intensity (13). Currently, new generation LED light devices offering deeper and uniform polymerization and third generation LED curing lights are on the market, the latter being also efficient for photoinitiators other than camphorquinone because of their wide range of wavelengths.
While many studies are available in the literature on the effect of light sources on the physical, mechanical and chemical properties of resin composites, there are no studies investigating their effect on the bond strength of different composites repaired with bulk-fill composite. The aim of this study was to evaluate and compare the effects of different light sources on shear bond strength when a bulk-fill composite was used for the repair of 6 different composite resins exposed to same surface treatment procedures. Our null hypothesis is that light sources will not have an impact on repair bond strength.
Materials and methods
PREPARATION OF SPECIMENS
The sample size was determined in consultation with Cumhuriyet University Faculty of Medicine, Department of Biostatistics. It was estimated that a sample size of 126 specimens (n=7 per group) would be needed for the study at α=0.05, β=0.10 and (1-β)=0.90 to achieve a power of 90%. For the study, specimens were divided into 6 groups each having 21 specimens and a total of 126 acrylic blocks were obtained with a cavity depth of 2mm and a diameter of 6 mm on one surface. Then, the cavities were filled with six different composite materials: Group 1: Filtek Z550 (A2, 3M ESPE, St. Paul, MN, USA), Group 2: Filtek Ultimate (A2, 3M ESPE, St. Paul, MN, USA), Group 3: Admira Ormocer (A2, VOCO, Cuxhaven, Germany), Group 4: Ceram.X Spheretec One (A2, Dentsply, Milford, USA), Group 5: Kalore (A2, GC Corporation, Tokyo, Japan) and Group 6: Filtek Bulk Fill (A2, 3M ESPE, St. Paul, MN, USA). The type, contents of the composites and manufacturer information are shown in Table 1. Following placement of composite resins into the cavities, polymerization was performed using a LED light source (Elipar DeepCure-S, 3M ESPE, St. Paul, MN, USA) with an output intensity of 1470 mW/ cm² at a distance of 1mm for 20 seconds. Then, all of the composite specimens were immersed in distilled water for 24 hours at 37 ºC and subjected to 5,000 thermal cycles (Thermocyler, Gökçeler Makine, Sivas, Turkey). Thermal cycle consisted of a dwell time of 30 seconds and a transfer time of 5 seconds in water baths at 5ºC and 55ºC (±2ºC) sequentially. Afterwards, the specimens were removed from the thermocyler and roughened with a diamond fissure bur (Meisinger 837G, Hager & Meisinger GmbH, Neuss, Germany) for 3 seconds under water cooling for surface preparation. The bur was replaced after every 4 samples. Then, surfaces of the specimens were rinsed with air-water spray for 10 seconds and dried. For final surface cleaning and to achieve additional surface roughness, a 37% phosphoric acid solution (Scotchbond Universal Etchant, 3M ESPE, St. Paul, MN, USA) was applied for 30 seconds. Following acid treatment, all surfaces were rinsed with a water spray for 15 seconds and dried with an air spray for 10 seconds.
Repair procedure
Following surface treatment procedures, all groups were divided into three subgroups (a,b,c) according to the light source used for polymerization (n=7). Detailed information on the light devices used for the study (manufacturer, light intensity, curing time) is given in Table 2. Then, an adhesive system (Single Bond Universal, 3M ESPE, St. Paul, MN, USA) was applied on the surfaces of the specimens for 15 seconds using a disposable bonding brush by rubbing and to remove the solvent, the surfaces were dried with air using the air-water spray for at least 10 seconds until no more activity was observed on the adhesive. After applying the adhesive, a previously prepared cylindrical transparent tube with an internal diameter of 3mm and a height of 4mm was placed in the center of the dental restoration. Then, polymerization was performed for 20 seconds in each group using their assigned light sources to fix the tubes onto the composite: ValoLED light source and standard power (Ultradent, South Jordan, UT, USA) for Groups 1a, 2a, 3a, 4a, 5a, 6a; Elipar DeepCure-S LED light source for Groups 1b, 2b, 3b, 4b, 5b, 6b and Hilux 250 QTH light source (Benlioğlu Dental, Ankara, Turkey) for Groups 1c, 2c, 3c, 4c, 5c, 6c. Subsequent to adhesive application, bulk-fill composite resin (Filtek Bulk Fill) was carefully placed into the tubes at a single step using a compule tip gun at a depth of 4 mm and slightly condensed with the plugger and then polymerized with aforementioned 3 different light sources for 20 seconds with LED light sources and 40 seconds with halogen light source. During polymerization, the light intensity of all light devices was verified using a radiometer (Peng Lim Enterprise Co, LTD, Taiwan) after every 5 specimens. At one hour after polymerization, plastic molds were cut using a scalpel and the tubes were removed from the composite (Figure 1). Following the repair procedure, the specimens were aged in distilled water at 37 ºC for 4 weeks and then subjected to shear bond strength test.
Table 1 Composite resins used in this study.
| Composite Resins | Type | Contents | Filler ratio weight-volume | Manufacturer |
|---|---|---|---|---|
| Filtek Z550 | Nanohybrid | Bis-GMA, UDMA, Bis-EMA, PEGDMA, TEGDMA, Zirconia, Silica | 81.8-67.8 | 3M ESPE, St. Paul, MN, USA |
| Filtek Ultimate | Nanofilled | Bis-GMA, UDMA, Bis-EMA, PEGDMA, TEGDMA, Zirconia, Silica | 78.5-63.3 | 3M ESPE, St. Paul, MN, USA |
| Admira | Ormocer | Bis-GMA, UDMA, Organic modified ceramic, silica | 79-56 | VOCO, Cuxhaven, GERMANY |
| Ceram.X SphereTEC One | Nanoceramic | Methacrylate modified polysiloxane, dimethacrylate, Barium-aluminum borosilicate glass, functional prepolymerized silicon dioxide | 77-55 | Dentsply, Milford, USA |
| Kalore | Nanohybrid | UDMA, DX-511 (UDMA), Bis-EMA lanthanide fluoride, strontium glass, barium glass, fluoroalumina silicate glass, silicon dioxide | 82-69 | GC Corporation, Tokyo, JAPAN |
| Filtek Bulk Fill | Bulk-fill | Bis-GMA, Bis-EMA, UDMA, Zirconia, Silica, Ytterbium trifluoride | 76,5-58,4 | 3M ESPE, St. Paul, MN, USA |
*Bis-GMA: Bisphenol A-diglycidyl methacrylate; UDMA: urethane dimethacrylate; Bis-EMA: ethoxylated bisphenol A glycol dimethacrylate; PEGDMA: polyethylene glycol dimethacrylate; TEGDMA: triethylene glycol dimethacrylate.
Table 2 Light sources used in this study.
| Light Sources | Manufacturer | Type | Wavelenghts | Light Intensity | Curing Time |
|---|---|---|---|---|---|
| Hilux 250 | Benlioğlu Dental Ankara, TURKEY | QTH | 390-480 nm | 500 mW/cm² | 40 s |
| VALO Cordless | Ultradent, USA | 3th generation LED | 395-480 nm | (Standard Mode) 1000 mW/cm² | 20 s |
| Elipar DeepCure-S | 3M ESPE, St. Paul, MN, USA | 2nd generation LED | 430- 480 nm | 1470 mW/cm² | 20 s |

Shear bond strength test
Shear bond strength test was performed using a universal testing machine (LF Plus, LLOYD Instruments, Ametek Inc., UK). The movable breaking apparatus to be used for the test was specially manufactured by an external provider on order using a lathe with a thickness of 1 mm and no sharp edges as required by ISO TR 11405 specifications. The fracture apparatus was placed at a perpendicular angle to the composite/composite repair surface of the specimens and the specimens were subjected to shear bond strength testing at a 0.5mm/min crosshead speed. Forces exerted during the loading were measured in Newton (N) units and values obtained were converted to Megapascal (MPa) units using Nexygen Software (Ametek Inc., UK) software and recorded for each specimen.
Examination of failure surface anddetermination of mode of failure
Following shear bond strength testing, failure surfaces of all specimens were examined under a stereomicroscope (Nikon SMZ800, Tokyo, Japan) at X30 magnification. After examination, failure modes were identified and recorded. Mode of failure was classified as adhesive, cohesive or mixed type. Adhesive failure was considered when the fracture was at the bonding interface of repair composite and the composite in the acrylic block, cohesive failure of the restorative material was considered when the fracture involved only the composite in the acrylic block, cohesive failure of the repair material was considered when the fracture occurred entirely in the repair composite and combinations of adhesive and cohesive failures were defined as mixed type failure.
SEM (Scanning Electron Microscope) analysis
After stereomicroscopic examination of all specimens, SEM analyses were conducted for a detailed assessment of failure surfaces using a SEM device (TESCAN MIRA3, Brno, Czech Republic) at X100 and X1000 magnifications. Prior to SEM analyses, failure surfaces of the specimens were coated with 90 A° thick gold/palladium using a coating device (Quorum Q150R ES, East Sussex, UK).
Statistical analysis
The study data were entered into a statistical software (IBM SPSS Statistics for Windows, Version 22.0, IBM Corp. Released 2017. Armonk, NY, USA). One-way analysis of variance (ANOVA) was used for data analysis when the assumptions for parametric testing were met. Pairwise comparisons among means were conducted using the Tukey HSD test. The margin of error was set at 0.05.
Results
Shear bond strength values
Statistical analyses of the study data showed that the light sources had an impact on shear bond strength of the composites exposed to same surface treatments and repair procedures. In the present study where 6 different composites were repaired with a bulk-filled composite using 3 different light sources, shear bond strength values differed significantly among groups (p<0.05). The mean shear bond strength values of the composites and associated standard deviations and between-group differences are presented in Table 3 by the light sources.
Except for the group involving repair of the Kalore composite, repair shear bond strength values obtained by 3 different light sources were statistically different among all groups. The highest bond strength values were found in all groups when Elipar DeepCure-S was used. Excluding Kalore repair group, shear bond strength values were in the following order: Elipar DeepCure-S > Valo > Hilux 250. In the Kalore composite group, a statistical difference was observed between DeepCure-S and Hilux 250 in terms of shear bond strength values but shear bond strength values did not differ among other LCUs (Table 3).
Among all light curing devices, the highest bulk-fill repair bond strength values were observed for the Kalore group. Comparing the bond strength of the composites repaired with bulk-fill composite, shear bond strength values were significantly different between Kalore and Ceram.X One (p<0.05) but there was no significant difference in bond strength among other composites. A graphical representation of repair shear bond strength values for the composites and light sources are presented in Figure 2.
Modes of failure
The modes of failure identified in he study groups are presented in Table 4. Among all groups, the most common mode of failure was cohesive failure of the restoration, followed by mixed type. Adhesive failure was the least common. None of the groups showed cohesive failure of the repair material.
Analysis of sem images
SEM images of the failure modes captured at various magnifications for composite surfaces of different composites are shown in Figure 3.
Table 3 Shear bond strength means (in MPa) and standard deviations for different light sources.
| Groups | Valo Cordless (a) | Elipar DeepCure-S (b) | Hilux 250 (c) |
|---|---|---|---|
| Filtek Z550 (1) | 18.97 ᴬ,ᵃᵇ (1.64) | 21.81 ᴮ,ᵃᵇ (1.32) | 16.53 ᶜ,ᵃᵇ (2.11) |
| Filtek Ultimate (2) | 18.37 ᴬ,ᵃᵇ (1.48) | 20.41 ᴮ,ᵃᵇ (0.89) | 16.51 ᶜ,ᵃᵇ (0.90) |
| Admira (3) | 18.38 ᴬ,ᵃᵇ (1.30) | 20.27 ᴮ,ᵃᵇ (1.13) | 16.44 ᶜ,ᵃᵇ (1.52) |
| Ceram.X One (4) | 17.99 ᴬ,ᵃ (1.48) | 20.04 ᴮ,ᵃ (1.49) | 15.67 ᶜ,ᵃ (0.80) |
| Kalore (5) | 20.87 ᴬᴮ,ᵇ (1.81) | 22.20 ᴬ,ᵇ (1.70) | 18.69 ᴮ,ᵇ (2.14) |
| Filtek Bulk Fill (6) | 19.03 ᴬ,ᵃᵇ (1.57) | 21.14 ᴮ,ᵃᵇ (1.29) | 16.83 ᶜ,ᵃᵇ (0.87) |
*Different lowercase superscripts in rows and uppercase superscripts in columns indicate statistically significant differences.
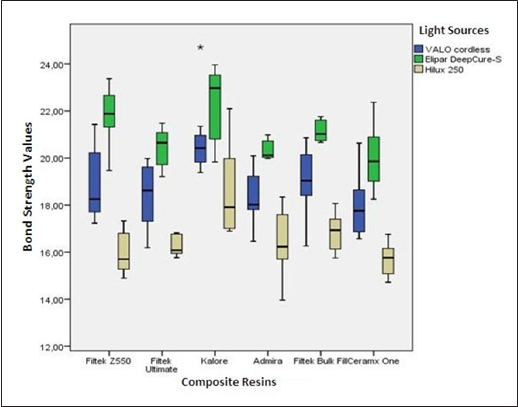
Table 4 Distribution of failure modes.
| Light Sources | Composite Resins | Adhesive Failure | Cohesive Failure | Mixed Type Failure |
|---|---|---|---|---|
| Valo Cordless | Filtek Z550 | 2 | 4 | 1 |
| - | Filtek Ultimate | 2 | 5 | 0 |
| - | Admira | 0 | 4 | 3 |
| - | CeramX One | 0 | 4 | 3 |
| - | Kalore | 0 | 5 | 2 |
| - | Filtek Bulk Fill | 1 | 4 | 2 |
| Elipar DeepCure-S | Filtek Z550 | 0 | 4 | 3 |
| - | Filtek Ultimate | 1 | 4 | 2 |
| - | Admira | 0 | 4 | 3 |
| - | CeramX One | 1 | 5 | 1 |
| - | Kalore | 0 | 6 | 1 |
| - | Filtek Bulk Fill | 0 | 5 | 2 |
| Hilux 250 | Filtek Z550 | 2 | 4 | 1 |
| - | Filtek Ultimate | 2 | 4 | 1 |
| - | Admira | 1 | 4 | 2 |
| - | CeramX One | 2 | 3 | 2 |
| - | Kalore | 0 | 5 | 2 |
| - | Filtek Bulk Fill | 1 | 3 | 3 |
| - | TOTAL | 15 | 77 | 34 |
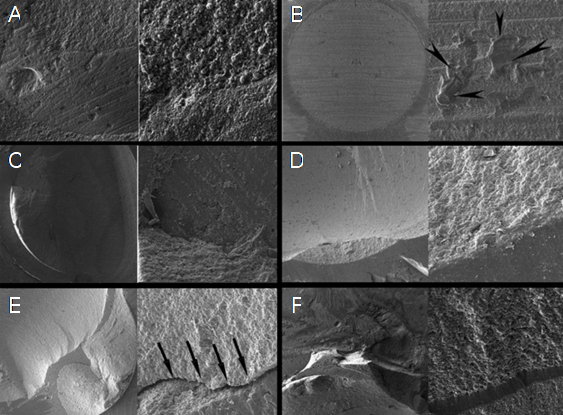
Figure 3 SEM images of different failure modes at X100 and X1000 magnification. A: Mixed type failure of CeramX One composite repair. B: Adhesive failure of CeramX One composite repair. The arrows indicate adhesive residues. C: Mixed type failure of Filtek Bulk Fill composite repair. D: Cohesive failure of Admira composite repair. E: Mixed type failure of Filtek Z550 composite repair. The arrows indicate the restorative material interface with the repair material. F: Mixed type failure of Admira Composite repair.
Discussion
In the current study investigating the effect of different light sources on the repair bond strength of different composites repaired with a bulk-fill composite resin, the light sources were found to affect bond strength. Thus, the null hypothesis was rejected.
In most of the studies involving composite repair, the restorative material repaired and the composite resins used for repair are usually the same (1,14,15,16). However, when dental restoration fails and the patient returns to the dental clinic, it may not be possible to identify which composite was used for the old dental restoration and in such cases, different composites are often adhered to each other in the repair process (17).
Physical and mechanical properties of composite resins polymerized using different light sources may be affected by the light source (18). Thus, in the current study, QTH (Hilux 250) representing the older generation of light devices, a second-generation, monowave LED (Elipar DeepCure-S) device offering a high depth of cure and a third-generation, polywave LED light source (Valo Cordless) were used for the polymerization of repair composites following the respective manufacturers’ instructions.
There are many studies that investigated the effect of light curing units on the composite- dentin bond strength, reporting conflicting results (19,20,21). However, few studies exist in literature on the effect of light devices on the repair bond strength of the composite resin. In one study (22), four different composites (Filtek Silorane, Filtek Z550, Gradia Direct Anterior, Aelite Posterior) were repaired with the same substrate, and QTH (Smart Lite), LED (Elipar FreeLight 2) and PAC (Monitex Plasma Star SP-2000) light curing units were used for polymerization. In contrast to our results, the authors did not find any difference in bond strength among composites repaired with QTH, LED and PAC light sources.
Previous studies reported that bond strength of the repaired area can be increased with improved quality of polymerization at the composite-repair interface (23,24). In the existing literature, the effectiveness of polymerization with LED and QTH light sources have been evaluated with respect to the depth of polymerization and surface hardness. A study (25) examined the effect of QTH and a second-generation LED light source on the depth of polymerization and surface hardness of three different composites and found that the second- generation LED light source provided a significantly greater depth of cure in all composites. In a different study (26), the effectiveness of a LED light curing unit (LCU) and a halogen LCU on the degree of conversion of 7 different composites was investigated and the LED LCU had superior effect on the degree of conversion versus halogen LCU in all study groups.
Consistently, QTH light source (Hilux 250) showed the lowest repair bond strength in all groups in the current study. This might be related to several factors: first, QTH light sources have a separate filter system and a very small portion of the energy generated by these light sources is converted into blue light; secondly, QTH light sources have a light intensity of 500 mw/cm², which is lower in comparison to the LED light devices used in our study, and thirdly, overheating of the system during the study might have caused energy loss and defects in lamp and filter over time.
Photochemically, since shorter wavelength photons have more energy, it was suggested that photons will not be absorbed by the chemical initiators which do not exactly match the absorption spectrum and will be scattered (27,28). In a study by Lucey et al. (29) where they evaluated the effect of second- and third-generation LED light sources on the degree of conversion (DC) of various restorative materials, best DC values were obtained when the composite was polymerized with the second-generation LED light source using camphorquinone as the photoinitiator. Shimokawa et al. (30) investigated the effect of 4 new generation LED light devices (Bluephase 20i, Celalux 3, Elipar DeepCure-S and Valo Grand) on the polymerization characteristics of 2 different bulk-fill resin composites (Filtek Bulk Fill and Tetric EvoCeram Bulk Fill) and found that Elipar DeepCure-S achieved better polymerization and greater microhardness at the center of the bottom layer in the Filtek Bulk Fill composite in comparison to Valo Grand. In contrast to those studies, no significant difference was noted between the monowave and polywave LED light curing units (Elipar S10 and Bluephase G2) in the degree of conversion of different bulk fill composites (31).
Better repair bond strength values achieved by Elipar DeepCure-S light source in comparison to Valo light source may be explained by the fact that Elipar DeepCure-S produces a more collimated and uniform beam profile with a special fiber transmission system. Additionally, Elipar DeepCure-S light device has a single-profile wavelength with less energy and the bulk-fill composite used contained camphorquinone as the sole photoinitiator, resulting in absorption of all of the light and used for polymerization and better bonding (28,30). Finally, Elipar DeepCure-S showed the greatest light intensity (1470 mw/cm²) values among the light devices studied and this may have affected the results. LED light curing unit with a greater light intensity showed better bond strength in a study by Lima et al. (32) in which the effect of various LED light-curing units and a halogen light source on regional bond strength of resin composite to the weakened roots was assessed, which is consistent with our findings.
The resin structure of the composite resins and the content and size of the filler particles may have an impact on the repair bond strength (33). Greater repair bond strength values found in the group that Kalore is repaired with bulk fill composite may be associated with a number of factors: Kalore has a monomer that contains a rigid molecular core that is resistant to polymerization shrinkage (DX-511), higher filler ratio in comparison to other composites and less water absorption by its monomers (34). The CeramX composite exhibited lower bond strength values and this may be related to the differences in organic matrix and filler content compared to the Filtek-Bulk Fill composite structure. In addition, the filler content of the CeramX composite is lower in volume than other composite resins.
Cohesive failures were more common than adhesive failures, suggesting that bond strength and adhesion of the restorative material aged with repair composite were adequate (35,36). In our study, adhesive failure occurred most commonly in the groups exposed to the halogen light source (Hilux 250) and the least adhesive failure was observed with the use of second-generation LED light source (Elipar DeepCure-S). Additionally, no adhesive failure was detected in the groups in which the Kalore composite was repaired. In line with a previous study (36), mixed type and cohesive failures were more common in the groups with higher bond strength values and adhesive failures were typically seen in the groups with lower bond strength values in our study. Taken together, these findings suggest that the bond strength values are affected by the modes of failure.
There are no sufficient in vivo studies in the literature on the repair bond strength which is required to achieve satisfactory results in the repair of the composite resins. Nevertheless, bond strength values between 15-30 MPa for the composite resin-enamel bond are considered to be sufficient for composite repair and clinically acceptable (37,38,39). The bond strength values obtained in our study fall within this range.
Conlusion
Within the limitations of the study, the light devices were found to have an impact on the bond strength of composite resins repaired with the bulk fill composite. In addition, it was concluded that the wavelength profile of the light devices and the composite content affected repair bond strength.
Conflict of Interest: The authors declare that they have no conflict of interest.
Funding: The study was supported by the Scientific Research Project Fund of Sivas Cumhuriyet University by project number Diş-186, Sivas, Turkey.
Ethical approval: This article does not contain any studies with human participants or animals performed by any of the authors.

