











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
PermalinkIntroduction
The maxillary canine is of great functional and aesthetic importance (1), but it is also one of the most commonly impacted teeth, second only to third molars (2). The incidence of impaction has been reported to vary between 1.0% and 2.2% (3,4). In 70-85% of impactions, the tooth is palatally located while others are either buccally impacted or in line with the maxillary arch (5,6,7). Careful supervision and early diagnosis of disturbances in canine eruption are considered important (7,8).
Early determination of maxillary canine displacement in relation to the surrounding structures is based primarily on radiographic examination. It has been emphasized that the angulation and location of the palatally displaced maxillary canines (PDCs) could play a role in determining the potential risks of lateral incisor resorption (9,10). Other possible complications associated with PDCs include migration or external root resorption of the displaced tooth or adjacent teeth, referred pain, malposition of the adjacent teeth, dentigerous cyst formation, loss of arch length, or a combination of these factors (8). Accordingly, various methods have been suggested for treating PDCs, some that involve interceptive approaches while others combine orthodontic and surgical strategies. The preferred treatment approach has generally been based on the canine position, as well as the patient’s age (11,12,13). Several factors are known to predict the difficulty associated with PDC treatment, such as displacement of the tooth from the occlusal plane, angulation of the tooth to the midline, the amount of overlapping of the neighboring teeth, and transposition with a lateral incisor or first premolar tooth (14,15). Although CBCT is seem to be the golden standart for the diagnose of PDCs, recents studies showed that panoromic radiographs could be considered good enough for rendering PDC position, so the need for 3D information is not crucial for treatment planning (16). Therefore, reliable predictions of successfully aligning PDCs and orthodontic treatment duration would be advantageous in the decision-making process for these patients (17).
Although several studies describe the possible relationships between the impacted canines and craniofacial morphology, few of them focused on determining the association of PDCs with lateral cephalometric parameters (18,19,20). Hence, this prospective study aimed to (i) assess the relationship between the initial position of PDC teeth on the panoramic radiograph -without additional imaging techniques- and craniofacial morphology, and (ii) characterize the predictors for treatment duration based on the initial positions of the PDCs.
Subjects and methods
Ethical approval was obtained from the Suleyman Demirel University (Isparta, Turkey) Ethical Committee of Clinical Investigations (approval no: 207), and consent forms were signed by all patients before the commencement of this prospective study. The study was set up as described below: It was planned to collect patients with PDCs and to perform analyses on their pretreatment cephalometric, panoramic radiographs and dental casts and to compare to a Class I control group; secondly, to perform standardized closed eruption technique for treating the PDCs; finally, to investigate the correlation between initial characteristics of PDCs and treatment duration. Power analysis was used for sample size calculation and the study’s power was estimated to be 90% with at least 20 subjects for each group (40 totally).
Initially, all patients who applied for the orthodontic treatment were assessed regarding the presence of PDC clinically (palpation) and radiographically (panoramic and cephalometric) until minimum 20 patients with unilateral or bilateral PDC were collected for the study group. Totally, 465 orthodontic patients (Caucasian population) were assessed and 23 patients with PDC (mean age: 16.6±4.1) on at least one side were included to the study through 2 years. The following inclusion criteria were applied for this group: no previous orthodontic treatment; permanent dentition (presence of all permanent teeth in the oral cavity except third molars and PDCs); requiring fixed orthodontic treatment or planned non-extraction fixed orthodontic therapy; good oral hygiene (no caries, no dental plaque accumulation and healthy periodontal tissues with generalized probing depths ≤ 3mm) and good cooperation. Patients with cleft lip and palate or other syndromes, systemic diseases such as hyperthyroidism, hypothyroidism, hyper and hypo parathyroidism, diabetes mellitus, rhomatoid artritis and medication usage which might affect bone formation and also tooth eruption process, supernumerary teeth, traumatic injuries, or other impacted teeth were not included to the study. Hence, 23 patients who were identified with a PDC that required an orthodontic-surgical treatment approach comprised the PDC group (21 female, 2 male). Afterwards, a Class I control group (23 patients), which required nonextraction fixed orthodontic treatment was established to compare the initial dental and skeletal features of the patients to PDC group. Consequently, the panoramic and cephalometric radiographs and dental casts of 46 patients constituted the study material.
All PDCs were surgically exposed and a closed eruption technique was performed, which involved a flap raised to expose the palatal surface of the canine crown, and removal of sufficient bone surrounding the canine tooth. A bonded button was attached with a 0.010" ligature wire onto the exposed tooth, and the flap was replaced and sutured. A light force (80-100 gr) was applied in vertical or distovertical direction by using orthodontic elastics attached to a lower removable appliance which provided anchorage and bite jumping (Figure 1a-i). The elastic traction continued until the canine erupted into the oral cavity. The participants were asked to use their intraoral elastics minimum 16-18 hours a day and note the daily usage. The notes of the patients were controlled in every appointment. When a patient missed an appointment; a new appointment was arranged as soon as possible. When the patient missed two ensuing appointments, he/ she excluded from the study. Fixed orthodontic appliances (Roth system, 0.018" slot; Omniarch, Dentsply GAC, USA) were applied to the maxillary dentition, for both groups. The upper arch was aligned using 0.014-0.018" round NiTi wires, followed by 0.016×0.022 and 0.017×0.025” NiTi rectangular archwires, respectively. The lower arch was bonded following the eruption of the canine into the cavity, and the final alignment of all teeth was achieved. A periodontal evaluation was performed following the debonding procedure. Treatment duration was measured in months and calculated as the time spent from the rising of the flap to reach to the impacted canine and first orthodontic force application to the alignment of the PDC into the dental arch (this point is defined as the application of 0.014 NiTi wires to the upper arch including the PDCs). Total duration of the fixed orthodontic treatment was not calculated to eliminate the effects of other teeth arrangements following canine alignment.
All patients had normal-shaped lateral incisors, except for one case with peg-shaped lateral incisors. The PDC was extracted in 1 case, owing to the risk of root resorption of the adjacent teeth and not included to the study group.
Pre-and post-treatment radiographic and dental parameters were measured by the second author (EB). All parameters are defined below.
Lateral cephalometric measurements
SNA°, SNB°, ANB°, SN-GoGn°, SN-PP°, and PP-MP° angles were measured cephalometrically. In addition, sagittal inclinations of the PDCs’ were determined. This parameter was defined as the angle between the longitudinal axis of the PDC and the palatal plane (C-PP°). The C-PP° angle was measured only in the PDC group since it was not possible to view the sagittal angulation of the erupted canine accurately in the Class I control group (Figure 2).
Panoaramic radiographic parameters
The following measurements which were described by Ericson and Kurol (7) and also used for classifying PDCs in recent studies as modified versions (21) were performed on the panoramic radiographs (Figure 3):
α angle: medial inclination of the crown of the permanent canine to the midline;
d distance: the distance from the cusp tip of the permanent canine to the occlusal line;
sector: the medial position of the crown of the displaced canine with respect to the central and lateral incisors. Five sectors, with sector I indicating the position of the crown of the displaced canine to be posterior to the distal aspect of the lateral incisor, and sector V indicating a position in correspondence with the mesial half of the upper central incisor, were defined.
Dental cast parameters
Crowding or diastema: Arch length-tooth size discrepancies were calculated.
Intermolar and interalveolar widths: Maxillary intermolar width was measured as the distance between mesiobuccal cusp tips of the maxillary first right and left first molars. Maxillary interalveolar width was measured as the distance between the mucogingival junctions above the mesiobuccal cusp tips of the maxillary right and left permanent first molars, using a caliper with 0.5 mm accuracy.
Statistical analyses
Data analysis was performed using SPSS for Windows, version 17.0 (SPSS, Inc., Chicago, IL, USA). Kolmogorov-Smirnov’s test was used to examine the data normality. The Student’s t-test, Mann-Whitney U test and Kruskal-Wallis test were used to compare variables that were not normally distributed while ANOVA was used for the normally distributed data. Post hoc Tukey’s HSD or Conover’s nonparametric multiple comparison tests were used for further comparisons when required. Nominal data were analyzed using Pearson’s chi-square test. Degrees of association between continuous variables were evaluated by Spearman’s rank correlation analysis. Statistical significance was set at p<0.05.
Results
Twenty-three patients who were identified with a PDC that required an orthodontic-surgical treatment approach comprised the PDC group (21 female, 2 male). A total of 30 PDCs were involved in this group (16 unilateral, 7 bilateral). This prospective study revealed that the prevalence rate of PDC was 5% of the orthodontic patient population within 2 years. The male:female ratio was 1:10.5 in the PDC group. This group exhibited 2.3 times more frequent unilateral impactions than bilateral occurrence. Right-left distribution of the unilateral impactions was almost equal (right: 9, left: 7). Table 1 presents the descriptive statistics of the parameters for the PDC and Class I control groups. The distribution of the PDCs according to the sector (Figure 4) demonstrated the PDCs were mostly located (30%) in sector III.
A comparison of the mean values of the parameters showed statistically significant differences in certain characteristics. The PDC group had greater SNA° (p<0.01), SNB° (p<0.05), and PP-MP° (p<0.05) angles and a smaller SN- GoGn° angle (p<0.01) compared with the Class I control group. Also, Class I control group had smaller arch length discrepancies, α angle, and d distance (p<0.001) while both the alveolar and molar arch widths and SN-PP° angle were similar between the groups (Table 2).
Locations of the PDC regarding sector were divided into 3 groups (sector I/II; sector III; and sector IV/V) and tested for intergroup differences with respect to all the other parameters. There was no significant difference between the groups for any of the parameters, except the SN-GoGn° angle, which was smaller in the sector IV/V group than sector I/II group (p<0.05). In addition, the treatment duration was significantly longer in the sector IV/V group than those of the other groups (Table 3).
When relationships between α angle and all other cephalometric and dental parameters were investigated, no correlation was found, except the SN-GoGn° angle. This angle showed a negative correlation with the angulation of the PDC (p<0.01). Treatment duration was also positively correlated with α angle (p<0.001). There was no correlation between d distance and other parameters. However, d distance was positively correlated with treatment duration (p<0.001). Canine inclination on the sagittal plane (C-PP°) was negatively correlated with intermolar arch width and ANB° (p<0.05) but not associated with the treatment duration (Table 4).
When periodontal recordings were evaluated, gingival hyperplasia on the canine teeth was determined in three cases and referred to the periodontology clinics for gingivectomy. Gingival recession or alveolar bone loss were not observed in the patients.

Figure 1 A-C: Pretreatment intraoral images of a patient with bilateral PDC, D-F: closed eruption technique and lower removable appliances, G-I: post treatment intraoral views.
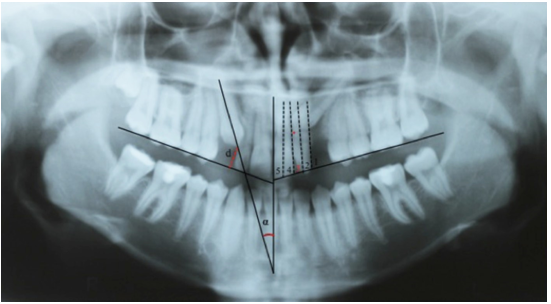
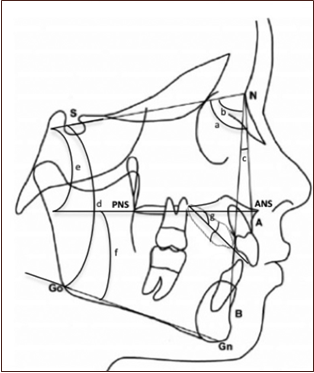
Figure 3 Parameters measured on the lateral cephalometric radiography. a: SNA°; b: SNB°; c: ANB°; d: SN-GoGn°; e: SN-PP°, f: PP-MP°, g: C-PP°.
Table 1 Descriptive statistics for the cephalometric, panoramic radiographies and dental cast parameters in the PDC and Class I control groups.
| - | PDC Group | Control Group |
|---|---|---|
| Parameters | - | - |
| SNA (°) | 81.9±3.77° | 79.3±3.2° |
| SNB (°) | 79.6±3.18° | 77.2±3.1° |
| ANB (°) | 2.3±2.24° | 2.3±2.2° |
| SNGOGN (°) | 31.1±4.28° | 34.6±5.0° |
| SN-PP (°) | 8.1±4.51° | 10.03±3.1° |
| PP-MP (°) | 27.5±5.90° | 24.6±4.1° |
| C/PP (°) | 65.0±9.21° | - |
| Arch width (alveolar)(mm) | 34.4±3.36 mm | 35.5±2.2 mm |
| Arch width (molar)(mm) | 39.9±3.50 mm | 41.2±2.4 mm |
| Crowding (mm) | 5.8±5.11 mm | 4.1±2.9 mm |
| α angle | 33.8±18.71° | 5.3±4.5° |
| d distance (mm) | 13.0±4.10 mm | - |
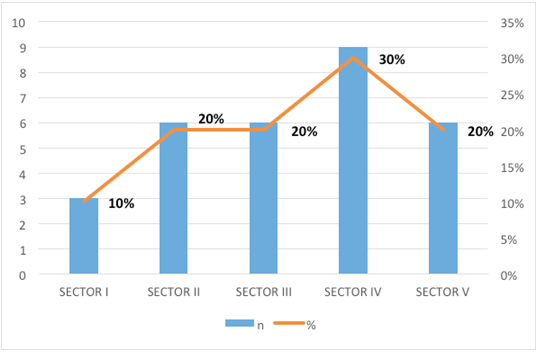
Table 2 Comparisons of the groups regarding to the clinical and radiographic parameters.
| Parameters | Control Group | PDC group | p value |
|---|---|---|---|
| Age (year) | 16.0±2.2 | 16.6±4.1 | 0.500† |
| Gender | - | - | 0.005‡ |
| Male | 11 | 2 | - |
| Female | 12 | 21 | - |
| SNA (°) | 79.3±3.2° | 81.9±3.8° | 0.010† |
| SNB (°) | 77.2±3.1° | 79.6±3.2° | 0.012 |
| ANB (°) | 2.3±2.2° | 2.3±2.2° | 0.866 |
| SNGOGN (°) | 34.6±5.0° | 31.1±4.3° | 0.006† |
| SN-PP (°) | 10.0±3.1° | 8.1±4.5° | 0.090† |
| PP-MP (°) | 24.6±4.1° | 27.5±5.9° | 0.033† |
| Alveolar Arch width (mm) | 35.5±2.2 mm | 34.4±3.4 mm | 0.199† |
| Molar arch width (mm) | 41.2±2.4 mm | 39.9±3.4 mm | 0.117† |
| Crowding (mm) | 4.1±2.9 mm | 5.8±5.1 mm | <0.001 |
| α angle | 5.3±4.5° | 33.7±18.7° | <0.001 |
| d distance | 0.6±1.3 mm | 13.0±4.1 mm | <0.001 |
† Student’s t test, ‡ Pearson’s Chi-square test, Mann Whitney U test.
Table 3 Comparisons of the sector groups regarding the clinical and radiographic parameters.
| Parameters | I-II (n=10) | III (n=9) | IV-V (n=16) | p-value |
|---|---|---|---|---|
| SNA (°) | 81.1±5.4° | 81.8±2.4° | 82.5±3.3° | 0.657a |
| SNB (°) | 79.7±4.0° | 79.2±3.0° | 79.7±2.9° | 0.922a |
| ANB (°) | 1.3±2.8° | 2.6±1.4° | 2.7±2.1° | 0.187b |
| SNGoGn (°) | 33.9±3.6c | 30.8±2.8° | 29.6±4.7c° | 0.036a |
| SN-PP (°) | 10.4±6.3° | 6.4±3.5° | 7.7±3.2° | 0.201b |
| PP-MP (°) | 27.2±7.4° | 29.2±4.1° | 26.7±5.9° | 0.592a |
| C/PP (°) | 67.6±9.9° | 66.0±8.6° | 62.9±9.1° | 0.348b |
| Alveolar Arch width (mm) | 34.4±2.5 mm | 34.8±1.6 mm | 34.3±4.5 mm | 0.756b |
| Molar arch width (mm) | 39.9±2.1 mm | 40.6±2.3 mm | 39.5±4.7 mm | 0.702b |
| Crowding (mm) | 6.6±6.0 mm | 5.7±4.9 mm | 5.4±4.9 mm | 0.849a |
| Treatment duration (month) | 8.4±3.2d | 8.3±4.2e | 12.7±5.3d.e | 0.010b |
a: One-Way ANOVA, b: Kruskal Wallis test, c: There is a difference significantly between the group “I-II” and group “IV-V” (p=0,028) for SNGOGN angle, d: Treatment duration was longer in group “IV-V” than group “I-II” significantly. (p<0,001), e: Treatment duration was also longer in group “IV-V” than group “III” significantly (p<0,001).
Table 4 Correlations between α angle, d distance, Canine/PP angle and cephalometric, dental cast measurements.
| - | α Angle | - | d distance | - | Canine/PP° | ||
|---|---|---|---|---|---|---|---|
| Parameters | Correlation coefficient | p | Correlation coefficient | p | Correlation coefficient | p | |
| SNA (°) | 0.177 | 0.310 | 0.117 | 0.504 | 0.149 | 0.417 | |
| SNB (°) | 0.130 | 0.457 | 0.097 | 0.578 | 0.323 | 0.071 | |
| ANB (°) | 0.177 | 0.309 | 0.061 | 0.728 | -0.417 | 0.018 | |
| SNGOGN (°) | -0.493 | 0.003 | -0.163 | 0.351 | 0.243 | 0.181 | |
| SN-PP (°) | -0.229 | 0.187 | -0.121 | 0.490 | -0.321 | 0.074 | |
| PP-MP (°) | -0.166 | 0.340 | -0.029 | 0.869 | 0.568 | <0.001 | |
| Alveolar Arch width (mm) | 0.208 | 0.231 | 0.063 | 0.717 | -0.227 | 0.212 | |
| Molar arch width (mm) | 0.183 | 0.293 | 0.016 | 0.929 | -0.388 | 0.028 | |
| Crowding (mm) | 0.273 | 0.131 | -0.061 | 0.738 | -0.145 | 0.443 | |
| Treatment duration (month) | 0.528 | <0.001 | 0.693 | <0.001 | 0.011 | 0.954 | |
Discussion
Predicting the possible successful alignment of the PDCs in the oral cavity and treatment duration for these patients has generally been based on subjective clinical experience. Patients with PDCs typically require longer treatment duration than other conventional fixed orthodontic treatment patients. Assessment of the risks and determination of the factors influencing the success rates are of great importance for the clinicians, as well as for the patients, to discuss the treatment outcomes and the treatment duration. Previous studies have identified certain parameters on the panoramic radiographs, such as the angle between the PDC and the midline, distance from the crown of the PDC to the occlusal plane, and the amount of overlapping of the incisor region by the PDC for the diagnosis and description of the degree of impaction of maxillary canines (9,14). However, sagittal inclination of the impacted canine that measured in the cephalometric radiographs has not been evaluated as a predictor for the treatment duration. In this prospective study, all these parameters were analyzed on the panoramic and cephalometric radiographs which were already taken routinely for orthodontic patients to determine the initial positions of PDCs’ in detail without requirement of an additional imaging technique.
Erupting and aligning labially-positioned impacted canines have been found to be easily managed, whereas PDCs have been considered as having more complexity in terms of requiring surgical intervention, auxiliary appliances and more adjustments of the archwires (6). In the present study, all patients were treated by using the same closed-eruption technique, which included an elastic usage between a removable appliance in the mandible and the button attached to the PDC. All PDCs were erupted into the oral cavity successfully. When we evaluated the initial angulations of PDC’s, it was found that the mean α angle of the PDCs was 33.8° (range: 5.5-79.0°). Based on this study result, PDCs exhibiting even large α angle were able to be erupted. Therefore, it is suggested that the decision to extract a PDC should not be based merely on this angle. Although Stewart et al. (14) found no correlation between the angulation of the PDC and treatment duration, the present study identified that an increase in this angulation significantly increased treatment duration. This difference between the studies might have been resulted from the differences in calculated treatment durations. In the present study, the treatment duration was calculated as from clinical A point to the clinical B point. The A point was the rising of the flap and also first orthodontic force application. The point B was the alignment of the PDC in the dental arch. This point was defined as the application of 0,014 NiTi archwire to the maxiller dentition including the PDCs. We did not calculate the total orthodontic treatment duration to be able to eliminate the time spent for the other teeth disarrangements, occlusion and finishing procedures. The calculated treatment duration was the time spent for purely to the surgical eruption and alignment of the PDCs.
Fernandez et al (22), reported the eruption characteristics of the permanent canines and considered an overlapping of the lateral incisor by the canine on the panoramic radiograph as a sign of a possible eruptive anomaly of the canine. It has been further shown that sector location was a significantly better predictor of impaction than tooth angulation (23,24). In the present study, most of the PDCs (30%) were located in sector IV (overlapped by the central incisors), in agreement with previous studies (15,23). Jung et al. noted that 80% of PDCs in patients aged over 15 years were located in sectors III, IV, and V (11). The success rate was reported to be 64%, even if the canine crown was mesial to the midline of the lateral incisor (10). However, according to Bishara (8) the extraction of the canine might be a better option if the canine was located between the roots of the central and lateral incisors and orthodontic movement could jeopardize these teeth. In the present study, one PDC located in sector V was extracted before the orthodontic treatment while the other teeth were repositioned by the surgical-orthodontic methods. As an early attempt, Ericson and Kurol (10) showed that early extraction of the deciduous maxillary canines could result in a normal eruption of the displaced permanent maxillary canines. However, if the permanent canine was positioned well beyond the mesial surface of the lateral incisor root, self-correction did not occur (8). Therefore, the sector and the angulation of the PDC have been critical in making decisions regarding interceptive treatment. In a previous study, immediate surgical exposure to a PDC located in sector IV with a large angle (α angle>30°) was recommended while it was suggested that canines angulated less than 20° and located in sector II could bemobserved without interceptive deciduous canine extraction (25). In addition, treatment duration was shown to be affected by the sector of the PDC (26). In a study conducted by Bazargani et al (26), the treatment duration averaged 17 months for canines displaced in sector I or II, 2.6 months longer for those in sector III, and 7.6 months longer for canines displaced in sector IV or V. Similarly, in the present study, treatment duration averaged 4.3 months longer for canines displaced in sector IV or V than sectors I-III, and this was statistically significant (Table 4). This finding may help in providing more precise information to the patients about the treatment duration.
It was stated that the “vertical distance” from the cusp tip of the unerupted canine to the occlusal plane was a more important and earlier predictor of eventual impaction than all other measurements made on a panoramic radiograph (9). A longitudinal study showed the maxillary canine could eventually remain impacted, as it loses potential movement in the vertical plane as early as 5 years of age. Unaffected canines continued to move downward in the vertical plane, reaching a distance of approximately 18 mm between 5 to 12 years of age. By 8 years of age, there was a mean difference of 4 mm between the impaction and control groups, and it became remarkable by the age of 9 years (9). In the present study, the mean vertical distance of the PDC group was 13 mm (range: 4.5-20.0 mm), and, in agreement with previous studies (14,15,16), this distance was positively correlated with the treatment duration, which ranged from 10 to 23 months. Hence, it was suggested that the greater the distance from the occlusal plane, the longer the treatment duration. Zuccati et al (17) evaluated the treatment durations for impacted canines and concluded that one additional visit was required for every 0.6- mm increase in this distance on the panoramic radiograph. Similarly, Stewart et al (14) found that PDCs located less and greater than 14 mm from the occlusal plane required average treatment times of 23.8 and 31.1 months, respectively. Although linear measurements on panoramic radiographs have not been suggested; all of the panoramic radiographs were taken with the same device in the same standard conditions in the present study.
In previous studies that investigated the correlations between PDCs and craniofacial characteristics in the sagittal and vertical planes, the PDC was found to be most frequent in patients with Angle Class II Division 2 malocclusions (18,19,20,27,28,29). However, in the present study PDC group presented a normal facial pattern and maxillomandibular sagittal relationships in agreement with Mercuri et al’s study (30) which reported that PDC was not associated with skeletal abnormalities. In a previous study, patients with PDC exhibited a significantly more prognathic maxilla and a more frequent occurrence of Skeletal Class I relationship than patients with buccally displaced canines (20). Although the present data showed statistically differences in the SNA° and SNB° angles between the PDC and Class I control groups, this can be clinically ignored since the mean values of these angles were within the normal range in both groups. According to Amini et al.’s study (31), PDC was not associated with maxillary or mandibular skeletal widths or lengths, whereas vertical dimensions were smaller in patients with PDC than patients with buccally displaced canines (20). Similarly, Chernochova et al. stated that the vertical plane angle (SN-GoGn°), which was correlated with the α angle and d distance, was significantly lower in the PDC group, demonstrating that the greater the α angleand d distance, the lower the SN-GoGn° angle as well (20). These all studies reported similar results on vertical plane characteristics of patients with PDC. In the present data, although the mean SN- GoGn° value was normal, 6 patients exhibited a hypodivergent pattern (SN-GoGn<27°) in the PDC group while the control group had only one hypodivergent case.
Although mesial angulation and the amount of overlapping of PDC by incisors have been evaluated by many investigators, labio lingual inclination of the PDC (measured between the vertical axis of the canine and the palatal plane) on cephalometric radiographs as a diagnostic factor has not been investigated before except Novak et al.’s study (32). Novak et al. pointed out that the angle less than 102° suggested the presence of PDC (32). In the current study, this sagittal angulation of the PDC was assessed cephalometrically combined with the other measurements. The possible relationship between the severity of this angulation and the other cephalometric and panoramic characteristics and also treatment duration were investigated. The mean of this angle was found to be 65°, indicating the severe labiolingual angulation of the PDCs. However, there was no relationship between this angulation and treatment duration for aligning the canine tooth.
The palatal position of the ectopic canine has been associated with excess space in the maxillary apical base in the literature (6,28,29,33). Interestingly, in the present study, arch length discrepancies (crowding) were significantly different between the groups in favor of the PDC group, even though the PDC group had wider arch length than the control group. Furthermore, there was no correlation between crowding and the PDCs’ positions (α angle and d distance). The presence of either crowding or space in the maxillary arch was not related to the canine impactions, within the limitations of the present study.
Another aetiological factor for PDCs discussed in the literature was the transverse maxillary arch width (27,31,34,35). While some authors noticed the transverse arch dimensions were significantly wider in the patients with PDC, some others observed no significant difference in the maxillary arch widths between patients with PDC and control sample (27,31,34,35). The present data showed both the intermolar arch and alveolar widths were similar between the groups, and the PDC group had adequate transverse arch dimensions. No correlation was evident between the arch parameters and the PDC’s location.
One of the limitations of the present study was the assessment of the PDCs without cone- beam computed tomography (CBCT). The recent studies suggest that panoromic radiographs are good enough for rendering PDC position and the use of routuine additional CBCT scans for PDCs can be minimized (16). Although the PDCs’ angulation was assessed on the lateral cephalograms, in some cases, a CBCT evaluation was required to ensure the absence of any contact or root resorption between the PDC and the adjacent tooth. Panoramic and lateral cephalometric radiographs were sufficient in most of the cases. Another limitation of this study was the sample size. Further studies involving a relatively larger sample size may be more useful for characterizing the predictors for successfully erupting and aligning the PDCs.
Conclusions
It is suggested that the greater the angulation of the PDC to the midline and the greater the distance of the PDC from the occlusal plane, the longer treatment duration expected. The treatment duration of the patients with PDCs in the sector IV/V (more mesially) was significantly longer than that of the other groups. Panoromic radiographs are sufficient for evaluating the positions of PDCs for most of the cases and intraoral elastic traction with a removable appliance in the opposite arch is a preferable method for impacted canines.

