











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Endodontic therapy should diminish the possible amount of major microorganisms and debris entering into the root canals, and this is achieved by mechanical instrumentation and suitable chemical irrigation. Another factor that determine the success of therapy is the shape of the root canal system (1,2). The instrumentation in straight canals is relatively simple; however, that in curved canals is challenging and depends on the knowledge and skills of the operator. Apical transportation in curved canals is important because the curvature of the canal affects the access for instrumentation and increases the risk of fracture of an endodontic file inside the canal (3). The apical transportation is defined as the elimination of dental structure in the outer part of the curvature of the apical third of the root canal (4). This is due to the tendency of the endodontic files to recover their original shape during the instrumentation of the root canals and this could lead to the creation of a zip and a possible perforation.
New instruments had been introduced in the endodontic field a few years ago, as substitutes for the conventional manual instruments or for supporting the instrumentation in case of curved canals or canals with complex anatomy. Thereby, there are endodontic files with memory control, which are manufactured with alloys that can return to their original form after plastic deformation. These materials can be deformed up to 10% and recover their initial state when bacterial load is removed from the canals (5). These effects are called thermal or shape memory effects and are observed as elastic shape-memory and/or super-elasticity (6,7). Recently, thermal treatments performed with endodontic files of nickel-titanium (NiTi) alloys have been used to optimize the mechanical properties of files.
Commercially, there are different brands of endodontic files with memory control such as Hyflex CM and Typhoon, which have been introduced in the market a few years ago. These instruments are more resistant to torsion and cycle fatigue and factors that cause fracture of the instruments, and allow a better conservation of the tooth structure during instrumentation because they follow the path with less resistance. These instruments were found to be successful in widening the root canals with complex anatomy (8,9). Hyflex CM design includes a triangular section, a variable helix angle, and an inactive tip, these instruments offers of 300-800% more resistance to fracture caused by fatigue cycle in comparison to the traditional NiTi files (10,11). Instead, Typhoon design includes a triangular transversal section (12,13).
Mtwo rotary system has characteristics that facilitate the instrumentation of the curved and narrow canals such as system files with a variable helix, small diameter, and a big conicity. These characteristics allow endodontist to work at the same length from the beginning of the instrumentation, keeping the original shape of the root canals, and provide a guidance for wider files resulting in a reduction of the apical transportation and fractures rates. This system also consists of an inactive and non-cutting round tip that stabilizes the instrument within the root canal and a reduced central nucleus, which has an “italic S” shape with two edges and a smaller transverse section that results in more flexibility (14,15).
The use of these files with memory control has not been demonstrated previously in vitro in extracted teeth with root canals with pronounced curvatures. Therefore, the aim of this study was to compare the apical transportation and loss of working length by the three rotary systems in root canals with curvatures more than 25 degrees.
Material and methods
Samples
Sixty molars extracted from patients with dental caries and/or periodontal disease, of the Oral Surgery Clinic of Dentistry Faculty were included in this study. All patients underwent an oral review for establishing the clinical diagnosis for the teeth extraction, panoramic and/or periapical radiography, a clinical history taking, and signed the informed consent for the study. All the included teeth had curved canals. Posteriorly, the cavities were made in each tooth by using a carbide round bur No. 4 and high-speed hand piece with cooling water (Pana-Max, NSK Nakanishi INC, Tochigi, Japan). Working length was determined using a 10 K endodontic file (Dentsply Sirona, York, PA) until it was visible at the foramen and pulling the file back by 1mm. Later, a 15 K file (Denstply, Sirona, York, PA) was placed at the working length. This study was approved by the institutional Ethics Committee.
X-RAY examinations
A standard X-ray scan was designed based on a previous study (16), fixing the head of the X-ray cone at two wooden supports, and a rotary platform was added in which the samples were attached inside a transparent plastic container. Radiography was performed while making the rotary platform spin until the file appeared straight and centered inside the root canals. Then, the platform was spun 90 degrees to reveal the maximum curvature of the root canals and obtain the initial X-ray scan. The initial position was recorded so that the final radiographs would be taken at the same position.
Measurements of the teeth
Curved canals with 25 to 52 degrees were included in the study. The degrees of curvature of each tooth were measured employing the Schneider method (17) using the software Sherlock (Teledyne Dalsa Inc, ON, Canada) and a 15 K file within the root canals. The radius of the curve of each tooth was determined using the software AutoCAD (Autodesk Inc, San Rafael, CA) and samples with radius from 3 to 9 mm were included (Figure 1. A and C).
Instrumentation and chemincal irrigation
The final apical preparation was set to number 30 in all groups. All root canals were preinstrumented manually using K files with stainless steel number 10 and 15 (Denstply, Sirona, York, PA) and later using endodontic motor SILVER (VDW, Munich, Germany). The 60 teeth were randomly divided in to three groups of 20 teeth in each one. One group of teeth (n=20) were instrumented with Mtwo rotary system (VDW, Munich, Germany) following the instructions of the manufacturer, using the sequence of files: #10/0.04 with a torque of 1.2 N/cm2, #15/0.05 with a torque of 1.3 N/cm2, #20/0.06 with a torque of 2.1 N/cm2, #25/0.06 with a torque of 2.3 N/cm2, and #30/0.05 with a torque of 1.2 N/cm2, at 280 revolutions per minute (rpm) of velocity. Another group (n=20) was instrumented with Hyflex CM rotary system (Coltene-Whaledent, Allstetten, Switzerland) following the instructions of the manufacturer, with the sequence of files: #25/0.08, #20/0.04, #25/0.04, #20/0.06, and #30/0.04, at 500 rpm with a torque of 25 N/cm2. The last group (n=20) was instrumented with Typhoon Infinite Flex NiTi rotary system (Typhoon TM, London, UK) with the sequence of files: #30/0.04, #25/0.06, and #20/0.04 at 400 rpm with a torque of 2-2.75 N/cm2. The chemical irrigation was performed using sodium hypochlorite at 2.25% concentration. Once the instrumentation and irrigation were finished, the final radiographs were obtained of all teeth to compare the central axes of the file before and after the endodontic procedure, and the distance between the axes was measured at 0,1,2, and 4mm from the working length. The loss of working length between the initial and final file was measured. The apical transportation was evaluated using two different views, the mesial-distal and buccal-lingual views by Maggiore´s technique (18).
Statistical analysis
All data were expressed as mean and standard deviation or as median and interquartile range, according to their normal or not normal distribution, respectively. The type of graphs used to express the results were scatter plots where each point represented an individual sample. Comparisons between the groups were performed using one- way analysis of variance (ANOVA) or Kruskal- Wallis tests, and the post hoc analyses employed were Dunn´s or Tukey´s multiple comparison tests. Association was analyzed by using Spearman or Pearson correlation test, according to the normality of the variables. The data were analyzed using GraphPad Prism software version 5.0 (GraphPad, San Diego, CA). A p value less than 0.05 was considered statistically significant.
Results
Loss of working length
All teeth were evaluated for the degrees of the curvatures and radius and were randomized in to the three groups (Mtwo system, HyFlex system, and Typhoon system groups) later. There were no significant differences in the degrees (mean ± standard deviation: 34.47±7.593, 35.96 ±6.800, and 35.73±7.287, respectively), and radius (mean±standard deviation: 6.22±1.45, 5.60±1.37, and 6.07±1.80, respectively) in each group (p>0.05, Figure 1. B and D). Therefore, we assumed that all groups worked in a similar way. Further, the Pearson´s correlation tests performed between the degrees of curvatures and radius in millimeters for each group showed no correlation between the data (data not shown). The loss of working length was measured for each tooth (Figure 2. A-C), and no significant difference was observed between the three systems (mean±standard deviation: 0.032±0.019, 0.36±0.020, and 0.039±0.018, respectively; p>0.05; Figure 2. D).
Aaplica transportation
The three groups of rotary systems were evaluated for the apical transportation by using a radiographic platform taking the preinstrumentation and postinstrumentation radiographs. For the Mtwo rotary system, we found similar values for each measurement at 0,1,2, and 4mm (mean±standard deviation: 0.028±0.015, 0.028±0.015, 0.0279±0.014, and 0.036±0.017, respectively) and thus, there was no significance difference between the values (p>0.05, Fig 3A). We observed similar results in the other two systems at 0,1,2, and 4mm: Hyflex CM (mean±standard deviation: 0.024 ± 0.012, 0.030 ± 0.019, 0.0303± 0.013, and 0.0247±0.0179, respectively) and Typhoon (mean±standard deviation: 0.0251±0.013, 0.031±0.017, 0.031±0.016, and 0.0294 ±0.013, respectively) (Table 1). There was no significance difference between the measured values in each group (p>0.05, Fig 3B and 3C).
Comparison of the apical transportations in the rotary systems
The apical transportation was evaluated at 0,1,2, and 4 mm in each rotary system (Figure 4. A). Comparisons among the groups performed using one way ANOVA could not find a significant difference in the apical transportation at 0 mm in Mtwo system in comparison with Hyflex CM and Typhoon systems (mean±standard deviation: 0.028 ± 0.015, 0.024 ± 0.012, and 0.025± 0.013, respectively) (p>0.05, Figure 4. B). Similar results were observed in the apical transportation at 1mm (mean ± standard deviation: 0.028±0.015, 0.030±0.019, and 0.031±0.017, respectively) and 2 mm (mean±standard deviation: 0.027±0.014, 0.030±0.013, and 0.031±0.016, respectively) in the three different rotary systems (p>0.05, Figure 4. C and D). We observed a significant trend of apical transportation at 4 mm for Mtwo system in comparison with Hyflex CM and Typhoon systems (mean±standard deviation: 0.036±0.017, 0.024±0.017, and 0.029±0.013, respectively) (p=0.08, Figure 4. E).
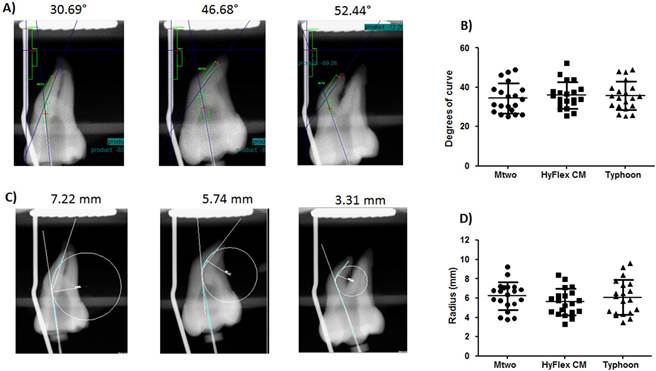
Figure 1 Degrees of curve and radius of each tooth in the three rotary systems. The degrees of curve and radius of each tooth was measured as described in the methodology. A) X-rays of some teeth showing the measurements of the degrees of curve. B) Degrees of curve of the samples employed for Mtwo, Hyflex CM, and Typhoon rotary systems. C) X-rays of some teeth showing the measurements of radius of the root canal. D) Radius in millimeters of the samples employed for Mtwo, Hyflex CM, and Typhoon rotary systems. In B and D, the horizontal lines show mean±standard deviation.
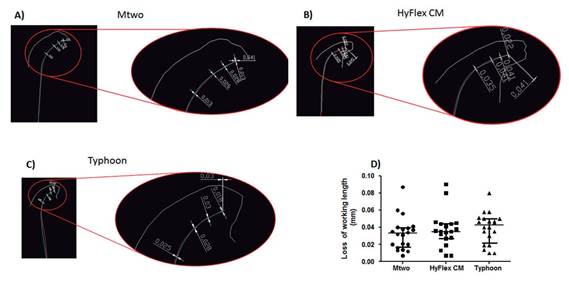
Figure 2 Loss of working length in the three rotary systems. Loss of working length was evaluated as described in the methodology. A) A representative image of measure of loss of working length in the Mtwo system. B) A representative image of measure of loss of working length in the Hyflex CM system. C) A representative image of measure of loss of working length in the Typhoon system. D) Comparison of loss of working length in millimeters in Mtwo, Hyflex CM, and Typhoon systems; the horizontal lines show mean±standard deviation.
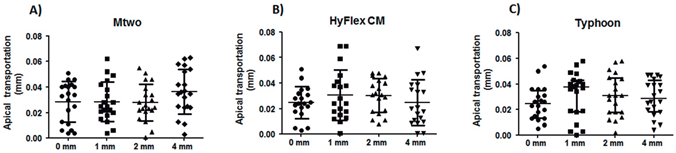
Figure 3 Apical transportation in the three rotary systems. The apical transportation in the three systems were evaluated as described in the methodology. A) Apical transportation in millimeters in the Mtwo system evaluated at 0,1,2, and 4 mm. B) Apical transportation in millimeters in the Hyflex CM system evaluated at 0,1,2, and 4 mm. C) Apical transportation in millimeters in the Typhoon system evaluated at 0,1,2, and 4 mm. In A-C, the horizontal lines show mean±standard deviation.
Table 1 Loss of working length and apical transportation values of the three rotary systems.
| Rotary system | Curve (degrees) | Radius (mm) | Loss of working length (mm) | Apical transportation | |||
|---|---|---|---|---|---|---|---|
| 0 mm | 1 mm | 2 mm | 4 mm | ||||
| Mtwo | 34.47±7.59 | 6.22±1.45 | 0.032±0.019 | 0.028±0.015 | 0.028±0.015 | 0.027±0.014 | 0.036±0.017 |
| Hyflex | 35.96±6.80 | 5.60±1.37 | 0.036±0.020 | 0.024±0.012 | 0.030±0.019 | 0.030±0.013 | 0.024±0.017 |
| Typhoon | 35.73±7.28 | 6.07±1.80 | 0.039±0.018 | 0.025±0.013 | 0.031±0.017 | 0.031±0.016 | 0.029±0.013 |
The values are provided as mean ± standard deviation and expressed in millimeters.
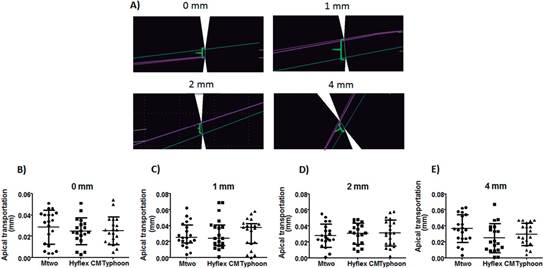
Figure 4 Comparison of apical transportation among Mtwo, Hyflex CM, and Typhoon systems. The apical transportation was evaluated based on the initial and final scans. A) Images of the measurements of apical transportation at 0,1,2, and 4 mm. B) Apical transportation measurements in millimeters evaluated at 0 mm for Mtwo, Hyflex CM, and Typhoon systems. C) Apical transportation measurements in millimeters evaluated at 1 mm for Mtwo, Hyflex CM, and Typhoon systems. D) Apical transportation measurements in millimeters evaluated at 2 mm for Mtwo, Hyflex CM, and Typhoon systems. E) Apical transportation measurements in millimeters evaluated at 4 mm for Mtwo, HyFlex CM, and Typhoon systems. In B-E, the horizontal lines show mean±standard deviation.
Discussion
Rotary systems are increasingly used in Endodontics due their specific characteristics that allow an easy root canal treatment by reducing the operator fatigue, the time required to finish the preparation, and the procedural errors associated with the root canal instrumentation (19). Among these NiTi rotary systems, the Typhoon and Hyflex CM designs include a triangular transverse section and a variable helix angle, and their wires suffer deformations before fracture and show lower critical tension values to stress than that of conventional wires, indicating more flexibility for CM wires (20,21).
The NiTi files show several useful aspects required for the instrumentation of root canals such as less root canals transportation and instrument separations; however, there are not enough evidence in the literature that compare the effect on canal curve during the shaping procedure using Typhoon, Hyflex CM, and Mtwo systems.
No significant differences were observed among the groups with respect to the apical transportation. These results can be explained by the fact that these rotary instruments are more flexible and therefore cause less transportation, and the flexibility of these rotary files depends on the relation between the parameters such as design, diameter, metal properties, and surface treatment. Other important aspect that was evaluated in this study was the loss of working length and no significant differences in the loss of working length were observed between the three groups. The loss of working length is influenced by the straightening of the root canal, after the instrumentation and/or by the accumulation of detritus in the apical third, and this accumulation of detritus can favor the failure of the endodontic treatment (22).
Studies have demonstrated the comparison between different endodontic files for evaluating the apical transportation and other characteristics. Zhao et al (11) reported that Hyflex CM files preserved the original shape of the root canals without causing apical transportation. Typhoon and Vortex files caused more apical transportation than that by self-adjusting file; however, the differences found by them could be due to the use of resin blocks instead of extracted teeth (8). Similar results have been reported in other studies evaluating different rotary files with different techniques of measurement of canal transportation (23,24,25,26). However, it is important to highlight that the differences found in some studies are due to the type of study design employed; in our study, we employed an in vitro design with extracted teeth.
A more sophisticated and novel technique for evaluating the canal transportation of rotary files in curved root canals is cone-beam computed tomography (CBCT) and this method allows to scan the root canals in a more accurate way. Recently, Jainaen et al (27) evaluated the preparation of curved root canals in extracted teeth using different rotary files (reciprocal vs rotational) using CBCT and they found less transportation and working time in reciprocal files (WaveOne and Reciproc) than in rotational files (ProTaper and Mtwo). In the present study, differences in apical transportation were not found with the different rotary files, probably due to the type of file used, the technique employed, and the degrees of curves of the teeth. We employed radiographs for the evaluation of apical transportation, which is a technique that allow to obtain a bi-dimensional image whereas CBCT provides images in three dimensions, which makes it a more accurate evaluation technique. However, one disadvantage of using CBCT is its high price compared to the conventional radiography.
Similar in vitro studies had been performed using CBCT for evaluating the apical transportation of rotary systems. Mesgarani et al (28) performed a study comparing the apical transportation of Mtwo and Recriproc rotary files using this technique and they found no differences in the amount of apical transportation in curved canals (>40°) with these files. Thus, they concluded that these rotary systems could be used clinically with the low risk of apical transportation.
The contradictory results found in different studies are due at the heterogeneity of data, degrees of curves of the teeth, files systems employed, technique of measurement of apical transportation, design of study, etc. This work has an in vitro design, and under the conditions of this study, Mtwo, Typhoon, and Hyflex CM files had shown no differences in the apical transportation and loss of working length, and the obtained results could be reproduced in clinical settings. The results of our study and other related studies were consistent with respect to the safe use of these rotary systems on patients under clinical settings.
The use of rotary instruments is essential for an endodontist during a root canal treatment, since these instruments are employed in most of the cases to optimize the time of work and to preserve the anatomy of the teeth, further research on these instruments should focus on improving the confidence of the operator and providing a secure, safe, and fast treatment to the patient.
Conclusions
In endodontic treatment, chemical-mechanical instrumentation is a key factor for achieving success and the use of rotary files is essential to achieve this objective. In addition, during the process of instrumentation, preservation of the conformation of root canals is a challenge. In this in vitro study, we demonstrated that the three rotary systems evaluated are safe and useful for instrumentation in curved canals, and their specific characteristics preserved the original shape of the root canals, which was essential to avoid the apical transportation or the perforation. Further in vivo studies are essential to compare the effectiveness and safety of these instrumentation systems.

