










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkOdontología Vital
On-line version ISSN 1659-0775Print version ISSN 1659-0775
Odontología Vital n.38 San Pedro, Lourdes de Montes de Oca Jan./Jun. 2023
Article
Management and Follow-up of Orthodontic Forced Extrusion: A Case Report
1
 http://orcid.org/0000-0002-4034-4583
http://orcid.org/0000-0002-4034-4583
2
http://orcid.org/0000-0001-5494-1816
3
http://orcid.org/0000-0003-4770-8156
4
http://orcid.org/0000-0002-8163-4093
5
http://orcid.org/0000-0003-0912-0466
1 Facultad de Estomatología. Universidad Autónoma de San Luis Potosí. E-mail: fojeda@uaslp.mx. Orcid: 0000-0002-4034-4583
2 Facultad de Estomatología. Universidad Autónoma de San Luis Potosí. E-mail:alanzuma@uaslp.mx. Orcid: 0000-0001-5494-1816
3 Facultad de Estomatología. Universidad Autónoma de San Luis Potosí. E-mail: manzur_nahim@hotmail.com. Orcid: 0000-0003-4770-8156
4 Facultad de Estomatología. Universidad Autónoma de San Luis Potosí. E-mail: rogelio.gonzalez@uaslp.mx. Orcid: 0000-0002-8163-4093
5 Facultad de Estomatología. Universidad Autónoma de San Luis Potosí. E-mail: francisco.ojeda@uaslp.mx. Orcid: 0000-0003-0912-0466
6 Facultad de Estomatología. Universidad Autónoma de San Luis Potosí. E-mail: arturo.garrocho@uaslp.mx. Orcid:0000-0001-9123-0300
7 Facultad de Estomatología. Universidad Autónoma de San Luis Potosí. E-mail:nveroza@fest.uaslp.mx. Orcid: 0000-0001-6014-0994
The case of an adult patient with a complicated Crown fracture of the right upper canine due to trauma is reported, diagnosing a class VII Ellis coronal fracture.
There are several treatment alternatives that range from the extraction, placement of a bone graft and placement of an implant, to a forced root extrusión with bone removal to allow the biological space and subsequently be restored.
In the present case, a multidisciplinary orthodontic forced extrusion treatment is performed, which allows to increase the amount of clinical remnant, preserving the periodontal support and maintaining the biologic thickness, thus achieving to maintain the root remnant with good length so that prosthetic rehabilitation is facilitated.
The clinical and radiographic follow-up was 12 months.
The multidisciplinary treatment involved: Root canal treatment, forced extrusion with orthodontics, fibrotomy with root planing and fixed prosthesis.
Key words: Trauma; Coronary fracture; Endodontics; Forcedextrusion; Prosthetic Restoration
Introduction
Some of the main reasons why patients go to the dentist are: Aesthetic and chewing problems, so patients prioritize this type of treatment (Uribe et al., 2010). Dental trauma represents a real therapeutic dilemma for the professional of stomatology (Koyuturk & Malkoc, 2005).
Most dental injuries occur within the first two decades of life, although they can occur at any age, the most susceptible teeth being the central and lateral incisors (AAPD, 2008-Forsberg & Tedestam, 1993). Fractures of the permanent teeth constitute the most frequent type of dental trauma, with a percentage of 26 to 76%.
These injuries involve the loss of dental tissues hard (Andreasen & Ravn, 1972-Andreasen, 1993), although they can involve enamel, or enamel and dentin, without affecting the pulp (Arapostathis et al., 2006), Good prognosis (De Blanco, 1996); however, when it affects the pulp (Cavalleri & Zerman, 1995-Ojeda et al., 2011), especially in cases of complex injuries of root and complicated crown the prognosis is generally less favorable long-term (Keinan et al., 2013).
Lesions involving enamel, dentin and pulp represent from 4 to 16% of all traumatic dental injuries (Cavalleri & Zerman, 1995- Stockwell, 1988), with the central incisors accounting for 80% and lateral incisors for 16% being the most frequently affected teeth due to their protruded and vulnerable anterior position in the mouth (Andreasen, 1970).
Different criteria have been established to classify the different types of dental fractures. The most recognized and used are those of Black, OMS and Ellis. (Spinas & Altana, 2002- Ellis & Davey, 1970).
According to these criteria, the treatment to be followed is established, which will depend on the degree of condition caused by the trauma, from control and observation appointments, direct or indirect pulp coating, partial pulpotomy, pulpotomy, pulpectomy, to tooth extraction.
When the fracture involves the entire crown, particularly in the anterior sector, a multidisciplinary dental treatment involving several pulpal, periodontal and restorative procedures is indicated.
In the present case, several procedures were carried out that involved the treatment of ducts and orthodontic forced extrusion with fibrotomy, with the aim of achieving a sufficient dental structure and an adequate biological space for prosthetic rehabilitation.
In 1977, Ingber developed the concept of extrusion force, which is defined as a vertical movement that is done with forces orthodontic controlled and continuous low-intensity, improving the ratio crown-root and eliminating defects intraosseous and bags, to allow the rehabilitation of the crown fractured (Ingber, 1989). Pontoriero (1987) proposes to perform the fibrotomy (resection of the periodontal fibers) together with the forced extrusion, which allowed to reduce the eruption time, resulting in an elongation of the crown without the need for bone resection (Pontoriero et al., 1987).
The objective of this report is to describe the management and follow-up of a case of orthodontic forced extrusión and the multidisciplinary treatment of the coronal fracture of an upper canine in an elderly adult patient.
Case Report
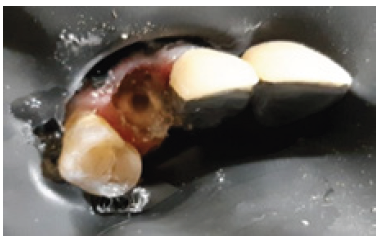
Apparently healthy 78-year-old patient comes to the clinic of the Specialty of Orthodontics and Dentomaxillofacial Orthopedics, referred by a specialist in Endodontics, due to corono-radicular fracture of right upper canine, fixed bridge abutment of three units (Figure 1). The patient reports having received a blow to the mouth about three weeks ago.
On physical examination, he presents good general conditions, with no apparent wounds or edema in the oral region.

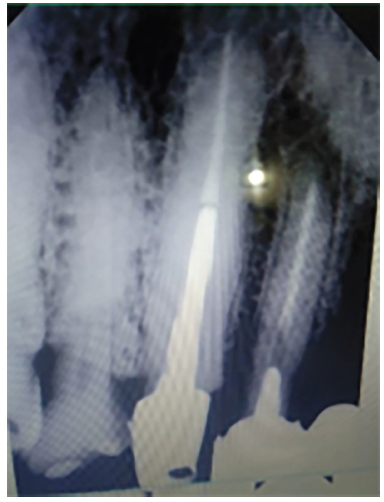
On intraoral examination, he presents with a cervical fracture of the Crown of the right upper canine (Ellis class VII). Periapical radiographs and clinical percussion, palpation and mobility tests are performed (Figure 2).
When evaluating the case, it is determined to carry out dental treatment with a multidisciplinary approach, which involves endodontics, orthodontics (forced extrusion), periodontics with fibrotomy and prosthetic rehabilitation.
As a first step, endodontic treatment was performed on the dental piece and placement of a supporting intracaval attachment (emptied endoposteum) (Figure 3), in order to improve orthodontic traction.
This attachment consisted of a cast post with perforations (Figure 4).
After an exhaustive orthodontic diagnosis, we proceed to place fixed appliances in the upper arch with MBT technique (slot 0.022), from the right molar to the left canine of indirect and passive cementing (with the slots of the brackets aligned).
Immediately after, a 0.019 x 0.025 rectangular arch made of stainless Steel with an extrusion bend was placed at the level of the right upper canine. In the same fold, a helix-type loop was adapted that functioned as a support to place the passive ligature (the cebanda) (Figure 5).


The activations of the apparatus were carried out every week with metal ligation (0.010), expecting an extrusive movement of 0.5 to 1 mm per week with a force between 15 and 20 grams per activation in addition to the realization of the circumferential supracrestal fibrotomy to help the extrusion and avoid its recurrence.
The treatment time to achieve the planned extrusion was 4 weeks, at the rate of one millimeter per week, in addition to 8 weeks of stabilization, for a total period of three months before placing the fixed prosthesis.
The circumferential supracrestal fibrotomy and root planing were performed before, during and after each orthodontic activation, in order to be able to decrease the stabilization time.
During the control appointments, at three, six, nine and twelve months, the stability of the extruded tooth was evaluated, through palpation of the mucosa, in addition to percussion tests and X-ray taking, mainly verifying the absence of clinical and radiographic signs and symptoms (Figure 6).

Discussion
The difficulty of treatment in the dental organs with transverse or intraalveolar fracture, which involves enamel, dentin, pulp and cement, represents a challenge for the dentist, who must take the necessary measures to maintain their vitality and their subsequent restoration in an aesthetic, pedagogical and functional way.
The accurate diagnosis of each individual case is carried out through the evaluation of the mobility of the coronary segment, the demonstration x-ray of the fracture line, and, on special occasions, through computed tomography, cone beam, which allows more accurate assessment of the extent and direction of the fracture line (May et al., 2013).
Different treatment modalities have been adopted for this type of injury, ranging from control and observation appointments to osteotomy, gingivectomy, orthodontic extrusión (Bondemark et al., 1997- Sönmez et al., 2008- Saito et al., 2009) or surgical, extraction or intentional reimplantation (Grossman, 1966).
An alternative treatment is forced extrusion by orthodontic means (Kumar et al., 2019), which is a conservative and predictable method to achieve a supragingival margin that allows the survival of the restoration in a longer term.
In the present case, along with the forced extrusion, the supracrestal circumferential fibrotomy was performed, described by Campbell (Campbell et al., 1975). This procedure consists of the resection of the periradicular fibers to the bottom of the gingival sulcus and root planing to minimize possible recurrence (Carvalho et al., 2006) and improve the stability of the affected tooth (Bach et al., 2004).
These actions allow the alveolar bone and the gingival extension to move together with the root (Edwards, 1988- Brain, 1969). It is recommended that the orthodontic extrusion speed be one millimeter of root movement (Bach et al., 2004- Durham et al., 2004- Jorgensen & Nowzari, 2001) per month and subsequently a stabilization period of eight weeks (Carvalho et al., 2006).
In 2000, Jorgensen (Jorgensen & Nowzari, 2001) recommended fibrotomy before, during and after forced orthodontic eruption, to decrease the necessary stabilization time.
The advantages of the procedure are the absence of bone loss or periodontal support, which usually occurs when an extraction is performed; the recurrence of the extruded teeth is avoided and the aesthetic appearance left by the extrusion is improved (Yoshinuma et al., 2009- Gonçalves et al., 2015). Its disadvantages are the use of orthodontic devices with consequent aesthetic problems and the impediment to proper oral hygiene.
The treatment time is 2 to 3 months, plus the stabilization period; according to Bach (Bach et al., 2004), it is contraindicated in ankylosed teeth, in the presence of vertical fracture, teeth with short roots, insufficient space in the arch and exposures of the furca.
Keinan (Keinan et al., 2013) and Simon (Simon et al., 1978) propose in some cases, where the exposed dental structure allows it, the placement of a supporting intra-ductal attachment, but this technique is not always possible.
In the present case, a hollowed post was cemented with perforations, which helped to pull the tooth in a progressive and controlled way, with an extrusión speed of one millimeter per week (Ingber, 1989- Carvalho et al., 2006), for 4 weeks, in addition to a retention period of eight weeks.
This procedure differed from that proposed by Durman, who suggests one month of stabilization for every millimeter of orthodontic extrusion.
In independent reports, Keinan (Keinan et al., 2013) and Farmakis (Farmakis, 2018) concluded that the prognosis of treatment is much more favorable in young patients. However, in this case, adequate extrusion was achieved in an elderly patient, along with the immediate placement of the prosthesis, so it represents a comprehensive and multidisciplinary treatment that offers good functional and aesthetic results. During the follow-up period, every three months until one year was completed, no pain was reported in the area, no signs or symptoms of apical or periapical pathology, nor radiographic periodontal defects were presented as expected in an elderlypatient. Finally, the restorations placed were functionally and aesthetically acceptable.
Conclusion
Through an interdisciplinary approach (endodontics, periodontics, orthodontics and prosthetics) the dentist can offer quality joint treatments, such as those described in the case reported here.
Here all the advantages offered by forced orthodontic extrusion were taken advantage of, even in an elderly adult patient, achieving a traction of four millimeters. This objective was achieved thanks to the use of light and controlled extrusive forces on the affected dental organ. With the described treatment modality, a crown lengthening can be achieved without the need to perform a bone resection, which allows a correct prosthetic rehabilitation, returning the function and aesthetics to the injured tooth and providing an integral Benefit to the patient.
We consider as a limitation of this report that the observation time of the case was not long enough. The authors declare that there is no conflicto of interest with respect to the case presented
Bibliografía
1. - Uribe et al., (2010). Ortodoncia Teoría y Clínica. Medellín, Colombia. Corporación para investigaciones biológicas. [ Links ]
2. - Koyuturk & Malkoc, (2005). Orthodontic extrusion of subgingivally fractured incisor before restoration. A case report: 3‐years follow‐up. Dental traumatology, 21(3), 174-178. [ Links ]
3. - American Academy on Pediatric Dentistry Clinical Affairs Committee-Pulp Therapy subcommittee (AAPD), (2008). [ Links ]
American Academy on Pediatric Dentistry Council on Clinical Affairs: Guideline on pulp therapy for primary and young permanent teeth. Pediatr Dent, 30, 175-183. [ Links ]
4. - Forsberg & Tedestam, (1993). Etiological and predisposing factors related to traumatic injuries to permanent teeth. Swedish dental journal, 17(5), 183-190. [ Links ]
5. - Andreasen & Ravn, (1972). Epidemiology of traumatic dental injuries to primary and permanent teeth in a Danish population sample. International journal of oral surgery, 1(5), 235-239. [ Links ]
6. - Andreasen, (1993).Textbook and color atlas of traumatic injuries to the teeth, 3rd ed. Copenhagen: Munksgaard; 216-256. [ Links ]
7. - Arapostathis et al., (2006). A modified technique on the reattachment of permanent tooth fragments following dental trauma. Case report. Journal of Clinical Pediatric Dentistry, 30(1), 29-34. [ Links ]
8. - De Blanco, (1996). Treatment of crown fractures with pulp exposure. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, 82(5), 564-568. [ Links ]
9. - Cavalleri & Zerman, (1995). Traumatic crown fractures in permanent incisors with immature roots: a follow‐up study. Dental Traumatology, 11(6), 294-296. [ Links ]
10. -Ojeda et al., (2011). Reattachment of anterior teeth fragments using a modified Simonsen's technique after dental trauma: report of a case. Dental Traumatology, 27(1), 81-85. [ Links ]
11. - Keinan et al., (2013). Applying extrusive orthodontic force without compromising the obturated canal space. The Journal of the American Dental Association, 144(8), 910-913. [ Links ]
12. -Stockwell, (1988). Incidence of dental trauma in the Western Australian school dental service. Community dentistry and oral epidemiology, 16(5), 294-298. [ Links ]
13. - Andreasen, (1970). Etiology and pathogenesis of traumatic dental injuries A clinical study of 1,298 cases. European Journal of Oral Sciences, 78(1‐4), 329-342. [ Links ]
14. - Spinas & Altana, (2002). A new classification for crown fractures of teeth. The Journal of Clinical Pediatric Dentistry, 26(3), 225-231 [ Links ]
15. - Ellis & Davey, (1970). The classification and treatment of injuries to the teeth of children: a reference manual for the dental student and the general practitioner. Year Book Medical Publishers. [ Links ]
16. - Ingber, (1989). Forced eruption: alteration of soft tissue cosmetic deformities. The International journal of periodontics & restorative dentistry, 9(6), 416-425. [ Links ]
17. - Pontoriero et al., (1987). Rapid extrusion with fiber resection: a combined orthodontic-periodontic treatment modality. The International journal of periodontics & restorative dentistry, 7(5), 30-43. [ Links ]
18. - May et al., (2013). Contemporary management of horizontal root fractures to the permanent dentition: diagnosis-radiologic assessment to include cone-beam computed tomography. Pediatric dentistry, 35(2), 120-124. [ Links ]
19. - Bondemark et al., (1997). Attractive magnets for orthodontic extrusion of crown-root fractured teeth. American journal of orthodontics and dentofacial orthopedics, 112(2), 187-193. [ Links ]
20. - Sönmez et al., (2008). Orthodontic extrusion of a traumatically intruded permanent incisor: a case report with a 5‐year follow up. Dental Traumatology, 24(6), 691-694. [ Links ]
21. - Saito et al., (2009). Management of a complicated crown‐root fracture using adhesive fragment reattachment and orthodontic extrusion. Dental Traumatology, 25(5), 541-544. [ Links ]
22. - Grossman, (1966). Intentional replantation of teeth reimplantation. Asociación J Am Dent, 72 (5): 1111-8. doi: 10.14219 / jada. archive.1966.0125. [ Links ]
23. - Kumar et al., (2019). Management of subgingival root fracture with decoronation and orthodontic extrusion in mandibular dentition: A report of two cases. Contemporary Clinical Dentistry, 10(3), 554. [ Links ]
24. - Campbell et al., (1975). Orthodontically corrected midline diastemas: A histologic study and surgical procedure. American journal of orthodontics, 67(2), 139-158. [ Links ]
25. - Carvalho et al., (2006). Orthodontic extrusion with or without circumferential supracrestal fiberotomy and root planing. International Journal of Periodontics & Restorative Dentistry, 26(1), 87-93. [ Links ]
26. - Bach et al., (2004). Orthodontic extrusion: periodontal considerations and applications. Journal (Canadian Dental Association), 70(11), 775-780. [ Links ]
27. - Edwards, (1988). A long-term prospective evaluation of the circumferential supracrestal fiberotomy in alleviating orthodontic relapse. American Journal of Orthodontics and Dentofacial Orthopedics, 93(5), 380-387. [ Links ]
28. - Brain, (1969). The effect of surgical transsection of free gingival fibers on the regression of orthodontically rotated teeth in the dog. American journal of orthodontics, 55(1), 50-70. [ Links ]
29. - Durham et al., (2004). Rapid forced eruption: a case report and review of forced eruption techniques. General dentistry, 52(2), 167-75. [ Links ]
30. - Suprabha et al., (2006). Reattachment and Orthodontic Extrusion in the management 9f an incisor crown-root fracture: A case report. Journal of Clinical Pediatric Dentistry, 30(3), 211-214. [ Links ]
31. - Jorgensen & Nowzari, (2001). Aesthetic crown lengthening. Periodontology 2000, 27(1), 45-58. [ Links ]
32. - Yoshinuma et al., (2009). Orthodontic extrusion with palatal circumferential supracrestal fiberotomy improves facial gingival symmetry: a report of two cases. Journal of Oral Science, 51(4), 651-654. [ Links ]
33. - Gonçalves et al., (2015). A mixed-model study assessing orthodontic tooth extrusion for the reestablishment of biologic width. A systematic review and exploratory randomized trial. International Journal of Periodontics & Restorative Dentistry, 35. [ Links ]
34. - Simon et al., (1978). Extrusion of endodontically treated teeth. The Journal of the American Dental Association, 97(1), 17-23. [ Links ]
35. - Farmakis, (2018). Orthodontic extrusion of an incisor with a complicated crown root fracture, utilising a custom-made intra-canal wire loop and endodontic treatment: a case report with 7-years follow-up. European Archives of Paediatric Dentistry, 19(5), 379-385. [ Links ]
36. - Newman (1992). Ortodoncias limitada para la población mayor: modalidades multidisciplinarias. Revista estadounidense de ortodoncia y ortopedia dentofacial , 101 (3), 281-285. [ Links ]
37. - Marianne et al., (2002) Tratamiento de periodoncia y ortodoncia en adultos. Am J Orthod Dentofacial Orthop, 122:420-428. [ Links ]
38. - Heithersay (1973). Tratamiento combinado endodóntico-ortodóncico de las fracturas radiculares transversales en la región de la cresta alveolar. Cirugía Oral, Medicina Oral, Patología Oral , 36 (3), 404-415. [ Links ]
39. -Girón, F. H., & Fernández, S. T. (2014). Ortodoncia en un paciente adulto mayor. Revista Mexicana de Ortodoncia, 2(3), 196-203 [ Links ]
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
