










Servicios Personalizados
Revista
Articulo
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista Costarricense de Cardiología
versión impresa ISSN 1409-4142
Rev. costarric. cardiol vol.6 no.3 San José sep. 2004
una Tarea Mundial.
Es bien conocido que más del 80%del problema global de las enfermedades cardiovasculares ocurre en países de bajos o medianos ingresos 1, 2. Los conocimientos actuales sugieren que, en el mejor de los casos, sólo el 50% del riesgo de enfermedad coronaria se debe a factores de riesgo conocidos.3 En este momento, los factores de riesgo tratables incluyen fumado, hipertensión, hiperlipidemia y diabetes. El estudio InterHeart, recientemente publicado, revela que el impacto de los factores de riesgo de enfermedad cardiovascular convencionales (fumado, hipertensión, colesterol elevado, diabetes), y de los factores de riesgo emergentes (trastornos de la glucosa, obesidad abdominal), varían según el origen étnico y geográfico (se inscribieron 15,152 casos y 14,820 controles). La prevalencia de estos factores de riesgo en la población mundial en general fue: fumado 45%, hiperlipidemia 50%, hipertensión 40%, y diabetes 20%. En el estudio InterHeart, cada uno de estos factores de riesgo estuvo relacionado en forma significativa a infartos del miocardio (p<0.0001) 4 .
Hoy en día, los factores de riesgo tratables incluyen fumado, hipertensión, hiperlipidemia, y diabetes en general. Muchos estudios han seleccionado factores de riesgo específicos para tratamientos farmacológicos y han logrado una reducción significativa de problemas cardiovasculares, pero muy pocos han tratado múltiples factores de riesgo al mismo tiempo. El beneficio del tratamiento global de los factores de riesgo sería una reducción más marcada de sucesos cardiovasculares. Esta estrategia ha sido probada en pacientes que se han presentado con infarto agudo del miocardio, y han sido seguidos en el estudio CHAMP 5 . En este estudio, se incluyeron 558 hombres y mujeres consecutivos hospitalizados por infarto agudo del miocardio, y en forma randomizada se dividieron entre tratamiento usual y tratamiento agresivo. Los lípidos se trataron agresivamente teniendo como objetivo un LDL <100mg/dL con medicamentos antihipertensivos adicionales y modificación de los factores de riesgo. El beneficio de la reducción global del riesgo después de un año de seguimiento, fue una reducción significativa en la mortalidad cardiaca, recurrencia de infarto del miocardio, de hospitalizaciones, y de la mortalidad por otras causas (p<0.05).
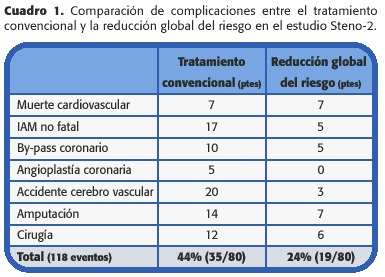
En el estudio Steno-2 6 , se comparó la reducción global del riesgo con el tratamiento convencional de los factores de riesgo modificables de enfermedad cardiovascular en pacientes con diabetes tipo 2 y micro albuminuria. Ochenta pacientes fueron asignados por randomización a recibir tratamiento convencional de acuerdo a los lineamientos actuales, y 80 a recibir tratamiento intensivo, con modificación en el comportamiento y terapia farmacológica dirijida a la hiperglicemia, hipertensión, dislipidemia, y micro albuminuria, así como aspirina para la prevención secundaria de enfermedad cardiovascular. La edad promedio de estos pacientes fue de 55 años y el seguimiento fue de 7.8 años desde la línea de base. En el Cuadro 1 se muestra el beneficio marcado que se observa con la reducción global del riesgo versus el tratamiento convencional (p<0. 01).
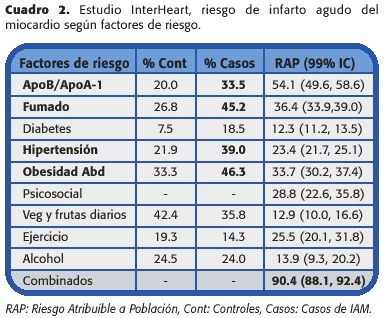
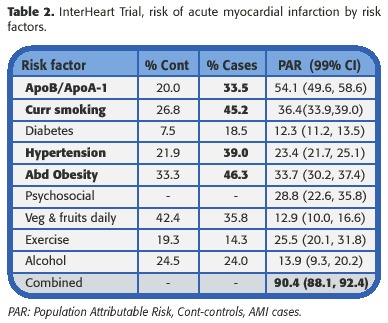
En el estudio InterHeart los cuatro factores de riesgo principales que se asociaron con infarto agudo del miocardio alrededor del mundo fueron hiperlipidemia, fumado, hipertensión y obesidad abdominal, como se muestra en el cuadro 2.
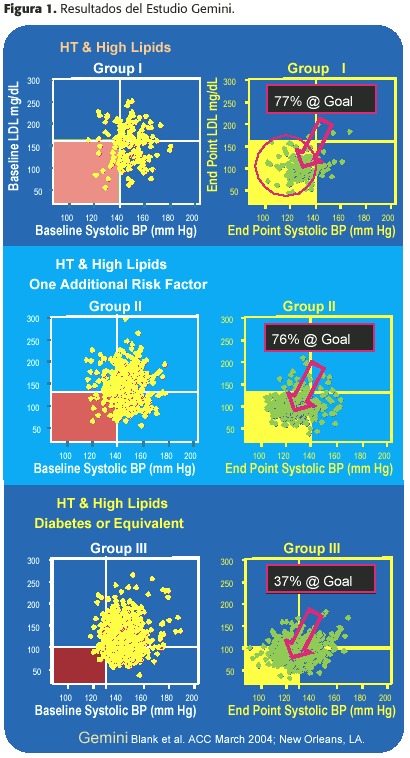
El beneficio de combinar dos medicaciones en una pastilla para mejorar el cumplimiento tiene muchas ventajas para los pacientes con hipertensión e hiperlipidemia. Actualmente, hay muchos compuestos que ayudan al tratamiento de estos pacientes de alto riesgo. Gemini, recientemente presentado en el congreso del 2004 del Colegio Americano de Cardiología, fue un estudio no controlado ni a doble ciego, de 14 semanas, en consultorios, prospectivo, de 1.220 pacientes con hipertensión y islipidemia. Gemini evaluó la utilidad de la pastilla Caduet ® (besilato de amlodipina/atorvastatina). El diseño del estudio no incluyó un período de lavado. Los pacientes reclutados en este estudio, tenían un rango de severidad de su hipertensión y su dislipidemia. La Figura 1 muestra tres puntos diferentes en este estudio usando la terapia combinada. El primer grupo de pacientes en esta figura representa un grupo de prevención primaria y el último grupo representando prevención secundaria. Nótese que los objetivos iniciales para LDL y presión arterial cambian en cada grupo. Los beneficios observados por el uso de sólo una pastilla dirigida a tratar dos de los factores de riesgo más poderosos, apuntan hacia un mayor beneficio en la reducción de eventos cardiovasculares en estos pacientes.
Global Risk Reduction: A World CV Burden
It is well known that over 80%of the global burden of cardiovascular disease occurs in low-income and middle-income countries. At best, the current thinking suggests that "only 50%" of the risk of CHD is accounted by known risk factors. Currently, treatable risk factors include smoking, hypertension, hyperlipidemia, and diabetes in general. The recently published InterHeart Trial revealed that the relative impact of conventional risk factors (smoking, hypertension, elevated cholesterol, diabetes)and emerging risk factors (glucose abnormalities, abdominal obesity)for cardiovascular disease does vary by ethnic and geographic origin (15 152 cases and 14 820 controls were enrolled). The prevalence of these risk factors in the world population in general was smoking 45%, hyperlipidemia 50%, hypertension 40%, and diabetes 20%. Each of these risk factors were found to be significantly related to myocardial infarctions (p<0.0001)in the InterHeart Trial.
Currently, treatable risk factors include smoking, hypertension, hyperlipidemia, and diabetes in general. Many trials have selected specific risk factors for pharmacological treatment with a significant reduction in CV events, but few have treated multiple risk factors at once. The benefit of global risk factor treatment would be a more marked reduction in CV events. This strategy has been test in patients who have presented with acute myocardial infarctions and then followed in the CHAMP trial.558 consecutive men and women were hospitalized for acute myocardial infarction randomly divided into usual care and aggressive treatment arm. Lipids were treated aggressively to a target LDL <100mg/dL with additional hypertensive agents and risk factor modification. The benefit of global risk reduction at one 1 year follow up was a significant reduction in cardiac ortality, recurrent myocardial infarction, re hospitalizations, and all cause mortality (p<0.05).
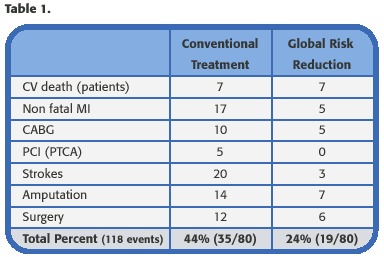
In the Steno-2 Study, compared global risk reduction with that of conventional treatment on modifiable risk factors for cardiovascular disease in patients with type 2 diabetes and microalbuminuria. 80 patients were randomly assigned to receive conventional treatment in accordance with current guidelines and 80 to receive intensive treatment, with behavior modification and pharmacologic therapy that targeted hyperglycemia, hypertension, dyslipidemia, and microalbuminuria, along with secondary prevention of cardiovascular disease with aspirin. The mean age of these patients was 55 years old with and 7.8 year follow up from baseline. Table 1 reveals with marked benefit seen with global risk reduction vs conventional treatment (p<0.01).
In the InterHeart Trial the most powerful top 4 risk factors associated with acute myocardial infarction around the world was hyperlipidemia, smoking, hypertension and abdominal obesity as seen in Table 2.
The benefits of combining 2 agents into one pill for improved compliance have tremendous advantages for the patients with hypertension and hyperlipidemia. Currently many agents will aid in the treatment of these high risk patients. In a recent trial, Gemini (American College of Cardiology Meeting 2004)was an uncontrolled, 14-week, office-based, prospective, open-label study of 1220 patients with concomitant hypertension and dyslipidemia. Gemini evaluated the utility of single-pill Caduet ® (amlodipine besylate/atorvastatin calcium). The study design did not include a washout period.
Patients enrolled in the study had a range of severity of both HT and hyperlipidemia. Gemini was an open-label uncontrolled clinical trial. Figure 1 shows 3 different treatment points using combined therapy. The first group of patients in the figure represents a primary prevention group and the last group representing secondary prevention group. Note that the baseline targets for LDL and BP change in each group. The benefits seen by the use of only one pill that targets two of the most powerful risk factors, points toward a greater benefit in reducing cardiovascular events in these patients.
Bibliografía:
1. Murray CJL, Lopez AD, eds. The global burden of disease: a comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020. Boston: Harvard School of Public Health, 1996. [ Links ]
2. Yusuf S, Reddy S, Ôunpuu S, Anand S. Global burden of cardiovascular diseases, part I: general considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation 2001; 104 : 2746 –53. [ Links ]
3. Charles H. Hennekens, MD, DrPH. Increasing Burden of Cardiovascular Disease. Current Knowledge and Future Directions for Research on Risk Factors. Circulation 1998; 97: 1095-1102. [ Links ]
4. Salim Yusuf, Steven Hawken, Stephanie Ôunpuu, Tony Dans, Alvaro Avezum, Fernando Lanas, Matthew McQueen, Andrzej Budaj, Prem Pais, John Varigos, Liu Lisheng, on behalf of the INTERHEART Study Investigators Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet 2004; 364: 937-952. [ Links ]
5. Gregg C. Fonarow, MD, Anna Gawlinski, DNSc, Samira Moughrabi, MN, and Jan H. Tillisch, MD. Improved Treatment of Coronary Heart Disease by Implementation of a Cardiac Hospitalization Atherosclerosis Management Program (CHAMP). Am J Cardiol 2001; 87: 819 –822. [ Links ]
6. Peter Gæde, M.D., Pernille Vedel, M.D., Ph.D. , Nicolai Larsen, M.D., Ph.D., Gunnar V.H. Jensen, M.D., Ph.D., Hans-Henrik Parving, M.D., D.M.Sc., and Oluf Pedersen, M.D., .M.Sc. Multifactorial Intervention and Cardiovascular Disease in Patients with Type 2 Diabetes. N Engl J Med 2003; 348: 383- 93. [ Links ]
* Profesor asociado de medicina y Director del Laboratorio de Cateterismo Cardíaco del Centro de Ciencias Médicas Audie Murphy VA de la Universidad de Texas en San Antonio. Fellow del Colegio Americano de Cardiología, del Colegio de Médicos Americanos, del Colegio Americano de Internistas Osteopáticos y de la Asociación Americana de Corazón. e-mail: chilton@uthscsa.edu

