











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Similars in
SciELO
Similars in
SciELO 
 Permalink
Permalink
Introduction
Currently, adolescent idiopathic scoliosis (AIS) is the most common and severe spinal deformity, which affects children and adolescents in the stage of neuromotor development and skeletal maturity of the sagittal curvatures of the spine (1). AIS is defined as a three-dimensional deformity of the spine characterized by lateral inclination and axial rotation of the vertebral bodies, with an angle equal to or greater than 10 degrees, as measured using the Cobb method (2). Worldwide, AIS affects about 2% of the population, but this can change according to the latitude of the country or region (1,4). The prevalence of AIS is higher in females, with 13 and 14 years being the ages most affected (5).
According to scientific evidence, the development of idiopathic scoliosis can occur in childhood and worsen in the adolescence period, with its most significant moment of progression associated with the growth spurt in the adolescence period. Its progression is strongly related to sex, age at onset, and the degree of spine angulation (6). The consequences of the progression of scoliotic curvature can vary from constant pain along the spine to functional impairments, such as reduced motor coordination, body balance, and changes in walking. The aesthetic changes of the spine, together with the physical-functional changes, such as social and psychological implications for the adolescent (7).
The progression of scoliotic curvature can be prevented or better controlled through an accurate and reliable prognosis for adolescents when combined with adolescents' capacity for growth and skeletal maturity(8,9). It is known that AIS progresses in the phases of more accelerated growth, also known as a growth spurt (8), the most vulnerable phase to the progression of scoliotic curvature, reaching 20 to 90% depending on the Cobb angle measurement, reliable radiographic parameters and with great clinical applicability for monitoring the progression of scoliosis (9).
To measure the Cobb angle, the X-ray examination, considered the gold standard, is done using two-dimensional or three-dimensional radiography (X-ray / 2D or 3D) taken for the sagittal and anteroposterior profiles. Cobb's method, the most widespread in clinical and scientific practice (9), measures the angle of the projection of a line tangent at the top of the vertebra, indicating the beginning of the spine's curvature, and another line tangent at the base of the vertebra, which indicates the end of the spine's curvature. Perpendicular lines are added to each line and the acute angle between them, called the Cobb angle, is measured. According to Goldberg et al., (10) Wills et al., (11) and Ricart et al., (12) the Cobb method is accurate and precise for radiographic measurements in traditional or digital printed form as well as for digital only measurements made through computer software. Despite being an effective and highly valid method, X-ray examination remains risky for patients with scoliosis: According to some authors, scoliotic patients monitored from childhood to adolescence underwent an average of 25 X-ray imaging exams to monitor the Cobb angle, corresponding to an average of 10.8 cGy ionizing radiation, increasing the risk of breast cancer and infertility in affected adolescents(13).
Three-dimensional (3D) exams, called EOS, have been included in current clinical and scientific practice to achieve better precision when assessing scoliotic curvatures (thoracic and lumbar), using an innovative ultra-sensitive X-ray imaging system that allows rapid (20 seconds) 3D exams (14,15). This method is advantageous because it reduces radiation dosages by up to 85% compared to traditional or digital radiography, both of which use standard two-dimensional (2D) X-ray technology (15,16). Despite this innovative method's considerable precision when measuring thoracic and lumbar scoliotic curvatures, the EOS system has high financial costs for patients, making it difficult for patients in the a single-payer healthcare system to access this exam, so scoliosis monitoring has largely remained in the form of traditional X-ray examinations (14-16).
Given this context, great efforts have been made by researchers and clinicians to uncover possible resources to indirectly measure the sagittal parameters of the spine as a way of monitoring scoliotic curvatures that would be predisposed to the lowest radioactive exposure of X-rays but maintain the precision and accuracy of scoliotic measurements of thoracic and lumbar curvatures in the prognosis of curvature progression. According to Tabard-Fougère et al., (17) accurate non-radioactive clinical tools for measuring scoliotic curvatures are needed to monitor the progression of this deformity during an adolescent's growth phase.
The literature presents several radiation-free instruments to assess and monitor the progression of scoliotic curvature angles in the AIS. The instruments presented in the literature are the flexicurve (18), the manual inclinometer (19) or inclinometer assisted by smartphone (19), the 3D ultrasound (20), the Zebris column system (21), rastereography (17,22), Scolioscan (23), and the electrogoniometer (24). Of all the instruments described in the literature, the inclinometer stands out in clinical practice, given its applicability-both manual (17) and digital (19)-and because it is a simple, fast system with a low cost which has received wide attention from many authors and doctors for measuring and monitoring the progression of scoliotic curvature in patients with AIS.
The applicability of the inclinometer is based on studies that refer to excellent reliability (ICC > 0.90) when compared to the X-ray image exam (17,19,22). However, the reliability and validity of the inclinometer at different stages of growth were not understood until recently, which underscores the significant clinical relevance of this study, since radiation doses from X-ray exams as part of the monitoring of scoliotic curvature in the growth phase is a major issue and greatly challenges the health and well-being of adolescents affected by idiopathic scoliosis. Thus, the aim of this study was to assess the reliability of the inclinometer and compare it to the gold standard of X-ray examination of the sagittal parameters of the spine in the early and late growth stages of adolescents with idiopathic scoliosis. We hypothesized that in the initial phase of growth, the inclinometer would present excellent reliability and validity in relation to the radiographic examination when compared to the late phase of growth.
Materials and methods
Study Design and Participants
This study had a cross-sectional design. The sample consisted of 39 adolescents with AIS seen at Clinica Escoliose Brasil, in the city of Campinas, São Paulo/SP. Adolescents were divided into two groups according to Risser sign: an initial growth phase (Group 1, 10-13 years, n = 16, Risser 1 or 2) and a late growth phase (Group 2, 14-18 years, n = 23, Risser 3 or 4). All adolescents or their respective legal guardians signed the Free and Informed Consent Term, previously approved by the Research Ethics Committee of the University of Santo Amaro, on the number: 2.729.155.
The following were the inclusion criteria: participants had to be between 10 and 18 years of age, diagnosed with idiopathic scoliosis with a Cobb angle between 20 and 40° according to a two-dimensional X-ray exam, considered the gold standard for scoliosis detection, as measured by a responsible doctor. The exclusion criteria were as follows: a body mass index (BMI) ≥ 29, other neurological, rheumatic, or orthopedic pathologies of the spine or lower limbs, presence of fractures less than six months old, respiratory or cardiac disorders, symptomatic musculoskeletal diseases in lower limbs, symptomatic diseases of the central and peripheral nervous system, diabetes mellitus, corrective surgery of the curvature of the spine, rigid deformities in the feet, infiltrations in the feet and ankles in the last three months, inability to stand and walk more than 100 m, mental disability, and the presence of tattoos or scars on the back (17).
Examination of X-ray Image and Evaluation of Inclinometer
Each adolescent was recruited for two evaluations: first, biplane radiography and second, inclinometer evaluation. It is worth mentioning that the radiographic evaluations were performed on different days, considering the time taken by the patient to schedule the same. When performing a biplane, a two-dimensional radiographic image, all adolescents underwent the X-ray image in the sagittal profile of the spine as part of the medical request to monitor and confirm the diagnosis of idiopathic scoliosis (Figure 1)(17). To undergo the X-ray examination, adolescents remained in an orthostatic posture in a standing position supporting their own body weight. The patients' feet remained in the same alignment in the frontal plane, with 7.5 cm between them. To reduce artifacts due to the projection of the humerus overlapping the spine, side imaging was completed with adolescents crossing their arms, fingers resting on the collarbones. The X-ray images were digitized and analyzed by physical therapist 1. After four weeks, the images were reevaluated by the same physical therapist and by a second physical therapist.

Figure 1 Representation of the performance of the frontal and sagittal profile of the X-ray image exam.
Immediately following the X-ray examination, the adolescent was referred to a physiotherapy clinic to assess sagittal, thoracic, and lumbar curvatures using the inclinometer (Tozz® magnetic base). In this evaluation, the adolescent was positioned in a standing orthostatic posture with body weight support, feet spread 7.5 cm and separated by ethyl acetate vinyl-EVA. The adolescents remained standing, with the physiotherapists measuring the sagittal angles of thoracic kyphosis and lumbar lordosis when positioned tothe side of the spine (sagittal plane). When measuring, both physiotherapists maintained the base of the inclinometer on the two spinous processes directed directly at the surface of the back, and the difference between the two measured values was the calculated angle. The standardization of the base of the two inclinometers was 2.5 cm for all evaluated adolescents.
Evaluation Parameters of Sagittal Angles: Thoracic Kyphosis and Lumbar Lordosis
To evaluate the digital X-ray image, the thoracic kyphosis (CT) angle was measured between the line tangent to the cranial ends of the fourth thoracic vertebra (T4) and the caudal end of the 12th thoracic vertebra (T12), and the angle of the lumbar lordosis (LL) was measured between the tangent at the cranial end of L1 and sacral (S1), called L1-S1 (Figure 2).
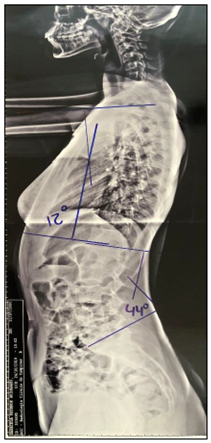
Figure 2 Representation of the sagittal angles of thoracic kyphosis and lumbar lordosis in the X-ray imaging of adolescents with idiopathic scoliosis.
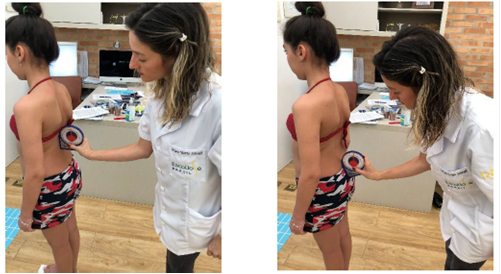
Using the inclinometer, the angle of thoracic kyphosis (CT) was measured by placing the base of the instrument on the spinous processes of T1-T2 and T12-L1, previously located by manual palpation. The angle of lumbar lordosis (LL) was measured by placing the base of the inclinometer over T12-L1 and L5-S1. In total, measurements were repeated three times by the same physiotherapist and the average of these measures was used for data analysis (Figure 3).
Data Reliability Analysis
To verify the degree of reliability of the intra-examiner analysis between the different instruments X-ray and inclinometer, a single examiner (physiotherapist 1) used an inclinometer to measure the sagittal angles with an interval of one week between the first and second X-ray assessments to ensure that there would be no memorization of the angles. To assess the inter-examiner reliability of the sagittal angles, two examiners (physiotherapists 1 and 2) evaluated the sagittal angles using both instruments-X-ray imaging and inclinometer-on the same day but in different environments to ensure that no information regarding data analysis could be exchanged, which would have interfered with the final result of the analysis (17,19).
Statistical Analysis
The normality of the data was verified using the Shapiro-Wilk test, and after confirming the non-normality of the data, nonparametric tests were performed. The Mann-Whitney test was used to compare the anthropometric variables of Groups 1 and 2 (i.e., the early and late growth stage groups). The Wilcoxon test was used to separately compare the sagittal parameters of the angles of thoracic kyphosis and lumbar lordosis according to each physiotherapist's measurements using each instrument (inclinometer and X-ray) and for each group. The same test was applied to compare the percentage differences between X-ray examination and inclinometer evaluation (percentage variation delta) for each evaluator. The Mann-Whitney test was used to compare the measurements by physiotherapists 1 and 2 of the sagittal angles for each instrument and group. These measurements were performed according to the sagittal parameters of the angles of thoracic kyphosis and lumbar lordosis for adolescents with AIS in the early and late growth phases.
To assess the intra- and inter-examiner reliability of inclinometer measurements in adolescents with AIS in the early and late stages of growth, the intraclass correlation coefficient (ICC) was used. To calculate the ICC equation type (1, 1) for the intra-examiner analysis, measurements were made one week apart by the same examiner, and for the ICC type equation (3, 3) for intra-examiner reliability, measurements were performed by physiotherapist 1 and physiotherapist 2 (24). The ICC was considered excellent if greater tan 0.75, moderate between 0.74 and 0.40, and poor if less than 0.39. To calculate the percentage delta differences, the following formula was applied: Δ % = X-ray angle − inclinometer angle × 100
X-ray angle
To assess the construct validity between inclinometer and radiography, Spearman's correlation coefficients were calculated. The percentage differences between inclinometer and radiograph measurements for the thoracic kyphosis and lumbar lordosis angles for Groups 1 and 2 were compared, and participants with differences greater than 5 ° were compared. For all analyses, p < 0.05 was considered significant (24).
Results
Adolescents with AIS in various stages of growth showed similar anthropometric characteristics. The differences between groups related to age and Risser sign, which demonstrate differences in the maturity of musculoskeletal systems, as observed in Table 1.
Table 1: Adolescents with idiopathic scoliosis in early and late growth stages according to body mass, height, body mass index, Cobb angle, and Risser sign.
| Variables | Initial growth phase (Group 1) mean (SD) | Late growth stage (Group 2) mean (SD) | p |
| Age (years) | 12.3 (1.0) | 15.0 (1.7) | 0.001* |
| Body Mass (kg) | 49.4 (8.0) | 50.6 (11.0) | 0.463 |
| Height (m) | 1.60 (0.1) | 1.5 (0.2) | 0.674 |
| Body Mass Index-BMI (kg /m2) | 20.3 (3.3) | 24.1 (4.9) | 0.124 |
| Thoracic Cobb Angle (degrees) | 31.8 (13.3) | 33.0 (8.4) | 0.369 |
| Lumbar Cobb Angle (degrees) | 32.4 (8.8) | 32.7 (7.8) | 0.412 |
| Risser sign (score) | and 2 (1.6) | 3 and 4 (3.1) | 0.019* |
* Mann-Whitney test, considering significant differences p < 0.05.
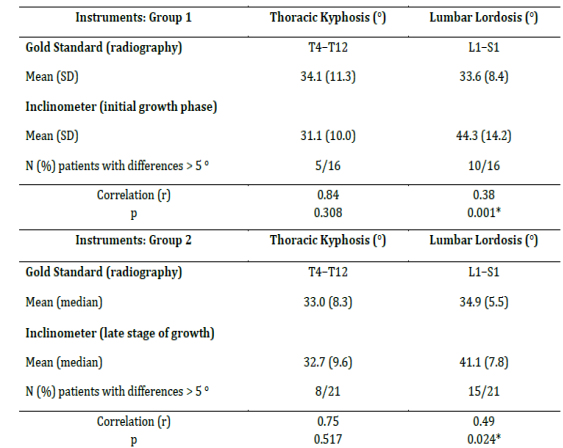
Table 2 shows that the sagittal angle of lumbar lordosis was found to be significant between the X-ray and inclinometer measurements, considering the same evaluator, both for the early and late growth stages. The angle of thoracic kyphosis showed no significant difference between the inclinometer and X-ray measurements when considering evaluations by a single examiner. Based on these findings, it can be inferred that the sagittal parameter of the spine of the lumbar lordosis angle is not effective; therefore, caution should be exercised when using the inclinometer to measure the lumbar lordosis angle given the significant differences between its measurements and the measurements of X-ray imaging for both the early and late growth phases.
Table 2: Sagittal parameters of thoracic kyphosis and lumbar lordosis measured by X-ray and inclinometer for each evaluator in adolescents with idiopathic scoliosis in early and late stages of growth.
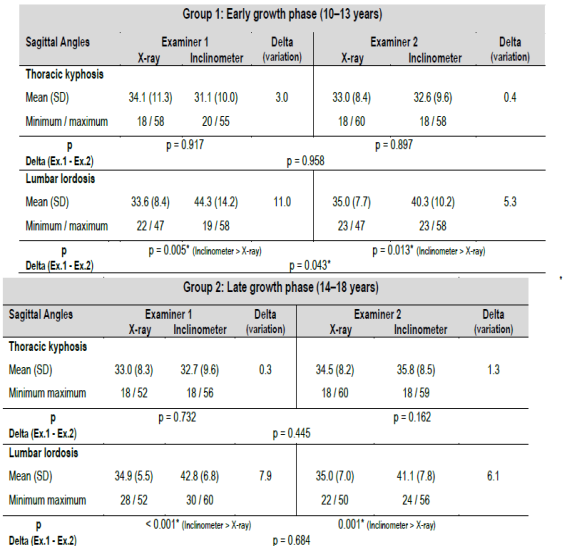
Wilcoxon test, considering significant differences p < 0.05.
Table 3 shows that for X-ray examinations, there was no significant difference between the physiotherapists' measurements of the sagittal angles of thoracic kyphosis and lumbar lordosis for the early and late phases of growth. It was also observed that the inclinometer effectively compared physiotherapists 1 and 2 when measuring the angle of thoracic kyphosis for early and late phases of growth. The sagittal parameter of the lumbar lordosis angle for physiotherapists 1 and 2 was significantly different for each phase of growth, which indicates that it has little clinical applicability for evaluating adolescents with AIS.
Table 3: Inter-evaluator sagittal parameters of thoracic kyphosis and lumbar lordosis according to X-ray image examination of adolescents with idiopathic scoliosis in different stages of growth.
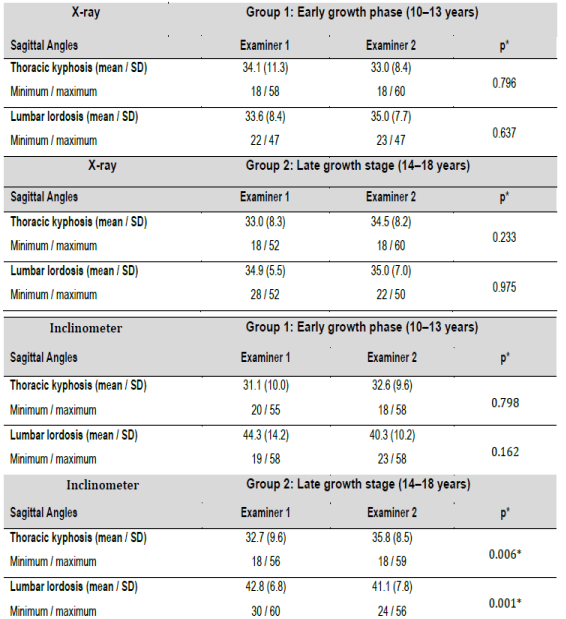
Mann-Whitney test, considering significant differences p < 0.05.
Tables 4 and 5 display the early and late growth phases with moderate intra-examiner reliability (ICC = 0.62; ICC = 65, respectively) and inter-examiner reliability (ICC = 0.64; ICC = 0.48, respectively) for the sagittal angle of lumbar lordosis when measured using an inclinometer. Only the sagittal parameter of the thoracic kyphosis angle showed excellent intra-examiner reliability (ICC = 0.88 for Group 1 and ICC = 0.90 for Group 2) and inter-examiner reliability (ICC = 0.86 for Group 1 and ICC = 0.85 for Group 2) when measured using an inclinometer. This indicates a moderate agreement of the sagittal angle of lumbar lordosis when measured using an inclinometer for the early and late growth phases when monitoring the scoliotic curvature of adolescents, considering the excellent reliability of the sagittal parameters of thoracic kyphosis and lumbar lordosis by X-ray.
Table 4: Intra- and inter-examiner reliability according to the intraclass correlation coefficient (ICC) of the sagittal angles of thoracic kyphosis and lumbar lordosis measured using both an inclinometer and radiography in adolescents with idiopathic scoliosis in the early phase of growth. * Intra-Class Correlation Coefficient (ICC), considering significant differences p < 0.05.
| Sagittal Parameters | Examiner 1 Mean (SD) | Examiner 2 Mean (SD) | ICC | p | Examiner 1 Mean (SD) | ICC | p |
| Thoracic Kyphosis | |||||||
| Inclinometer (°) | 31.1 (10.0) | 32.6 (9.6) | 0.86 | 0.557 | 32.2 (9.3) | 0.88 | 0.563 |
| Radiograph (°) | 34.1 (11.3) | 33.0 (8.4) | 0.93 | 0.721 | 33.6 (8.5) | 0.92 | 0.681 |
| Lumbar Lordosis | |||||||
| Inclinometer (°) | 44.3 (14.2) | 40.3 (10.2) | 0.64 | 0.045* | 48.6 (8.5) | 0.62 | 0.038* |
| Radiograph (°) | 33.6 (8.4) | 35.0 (7.7) | 0.91 | 0.492 | 34.5 (8.2) | 0.96 | 0.675 |
Table 5: Intra- and inter-examiner reliability according to the intraclass correlation coefficient (ICC) of the sagittal angles of thoracic kyphosis and lumbar lordosis measured using both an inclinometer and radiography in adolescents with idiopathic scoliosis in the late phase of growth. * Intra-Class Correlation Coefficient (ICC), considering significant differences p < 0.05.
| Group 2 (14-18 years) | Inter-Examiner (same day) | Intra-Examiner (a week later) | |||||
| Sagittal Parameters | Examiner 1 Mean (SD) | Examiner 2 Mean (SD) | ICC | p | Examiner 1 Mean (SD) | ICC | P |
| Thoracic Kyphosis | |||||||
| Inclinometer (°) | 32.7 (9.6) | 35.8 (8.5) | 0.85 | 0.130 | 32.9 (9.1) | 0.90 | 0.652 |
| Radiograph (°) | 33.0 (8.3) | 34.5 (8.2) | 0.95 | 0.579 | 33.2 (8.1) | 0.96 | 0.846 |
| Lumbar Lordosis | |||||||
| Inclinometer (°) | 42.8 (6.8) | 41.1 (7.8) | 0.48 | 0.009* | 38.7 (8.5) | 0.65 | 0.040* |
| Radiograph (°) | 34.9 (5.5) | 35.0 (7.0) | 0.88 | 0.744 | 34.2 (5.3) | 0.92 | 0.942 |
Table 6 shows the weak correlation between the measurements of the sagittal angle of lumbar lordosis using an inclinometer and using X-ray imaging for both the early and late growth phases, demonstrating inefficient validity to use thoracic kyphosis and lumbar lordosis to monitor the sagittal parameter of the spine in adolescents with AIS.
Discussion
This study evaluates the inter- and intra-examiner agreement (reliability) of the inclinometer, a radiation-free instrument, and its relationship with the gold standard of the X-ray exam on the sagittal parameters of the spine in the early and late growth phase of AIS. The main results showed that the sagittal angle of lumbar lordosis was different between the X-ray and inclinometer measurements taken by the same physiotherapist for both the early and late growth stages. When used by different physiotherapists, the inclinometer yielded differing measurements for the lumbar lordosis angle for early and late phases of growth; this demonstrates that the inclinometer has little clinical applicability for monitoring the scoliotic curvature of the lumbar in AIS. Another important point was the inclinometer's moderate intra-examiner and inter-examiner reliability when measuring the sagittal angle of lumbar lordosis; the thoracic kyphosis angle demonstrated excellent intra-examiner and inter-examiner reliability for the different stages of growth. In addition, the sagittal angle of lumbar lordosis measured using an inclinometer was weakly correlated to the gold standard of X-ray examination in the early and late stages of growth. This demonstrates that it is an inefficient method for monitoring the sagittal parameter of the spine in adolescents with AIS. The angle of thoracic kyphosis was shown to be highly correlated with the X-ray examination. The sagittal parameter of thoracic kyphosis for adolescents with AIS who were in different growth phases did not vary when measured using X-ray imaging and using an inclinometer, but measurements of the sagittal parameter of lumbar lordosis were affected by the different stages of growth. One study has considered variations in measurements of the angle of thoracic kyphosis (T4-T12 and T5-T12), and the sagittal parameter has been revealed as crucial for the clinical practice of monitoring the progression of scoliotic curvatures by means of X-ray examination (24). Other studies have revealed that the sagittal parameters of the spine (thoracic kyphosis and lumbar lordosis) of an adolescent with scoliosis should be monitored using radiation-free instruments, including the manual inclinometer (17) and the digital inclinometer (19), that demonstrate good reproducibility for sagittal angles measurements. The differential of this study was to consider the early and late phases of growth and to show that measurements of the sagittal parameter of lumbar lordosis using an inclinometer would differ significantly between examiners. Thus, it can be inferred that health professionals should be very cautious when assessing the clinical applicability of the inclinometer to monitor the scoliotic curvature of the lumbar of adolescents with AIS. It is important to consider the different growth phases when using a radiation-free instrument, such as the inclinometer, because an instrument is needed that can identify scoliotic curvature while the bone tissue is maturing while also maintaining the precision and accuracy of sagittal measurements of the spine (22,27). This study has shown that the inclinometer has moderate intra-examiner and inter-examiner reliability for the sagittal angle of lumbar lordosis; furthermore, the thoracic kyphosis angle showed excellent intra-examiner and inter-examiner reliability in the early and late stages of growth. These results corroborate the study by Tabard‑Fougère et al., (17) who observed that the angles of thoracic kyphosis and lumbar lordosis measured using an inclinometer are reliable for adolescents with AIS but have a weak correlation with the angle of lumbar lordosis when compared with X-ray imaging. The literature has emphasized the good correlation of the angle of thoracic kyphosis using various radiation-free instruments-namely, the flexicurve(18), the 3D ultrasound (20), the ZEBRIS system(21), rastereography (17,22), Scolioscan (23), and the electrogoniometer (28) - to evaluate adolescents with scoliosis. Among all these instruments, the inclinometer has stood out both clinically and scientifically, given its easy applicability and low cost, which has proven to be reliable and valid when measuring the angle of thoracic kyphosis but which has a weak correlation with the angle of lumbar lordosis (17,19,22), as observed in the present study. However, other studies that used surface topography have shown a good correlation between the angle of lumbar lordosis and the X-ray measurement in adolescents with idiopathic scoliosis (30,31). Differences in the angle of lumbar lordosis and its weak correlation when compared to the gold standard of X-ray examination might be due to variations in the anatomical positioning of the inclinometer for the repeated intra-examiner evaluations and between the evaluators (inter-examiner); this supports the low validity of this instrument when used for adolescents with idiopathic scoliosis. These discrepancies might also be due to the various factors that can affect the curvature of lumbar lordosis, including tension in the ligaments, tension between the paravertebral, hip, and abdominal muscles, and the inclination of the pelvis both in the orthostatic position and during the pubertal growth spurt, which contribute to the misalignment of the lumbosacral vertebrae in the sagittal plane, especially in relation to spinal deformities such as scoliosis (32). The inclinometer has had great applicability in clinical practice and has received wide scientific and clinical attention from health professionals for measuring and monitoring the progression of scoliotic curvature in adolescents with idiopathic scoliosis. Its applicability has been guided by studies that refer to excellent reliability (ICC>0.90) when compared against the X-ray image exam (17,19,22,23). This study is clinically relevant because it demonstrates the reliability and validity of the inclinometer at different stages of growth for the angle of thoracic kyphosis although not for the angle of lumbar lordosis compared to the gold standard of the X-ray. Reducing radiation exposure when monitoring scoliotic curvature in adolescents is a major issue, as radiation challenges the health and well-being of adolescents with scoliosis. This study is limited because the inclinometer's performance was not compared against X-ray exams using the EOS system, which reproduces micro-doses of radiation two to three times smaller than the traditional X-ray. According to the literature, the EOS system has a lower radioactive dosage but is very expensive and is generally not available to the public health system; thus, it is difficult for affected adolescents to benefit from this system.26,34 Therefore, future studies concerning these measurement tools should better understand the sagittal parameters of the spine at different stages of growth in adolescents with idiopathic scoliosis.
Conclusion
The early and late phases of growth showed excellent inter- and intra-examiner agreement (reliability) regarding measurements by the inclinometer, a radiation-free instrument, of the sagittal parameter of thoracic kyphosis as well as moderate reliability regarding the angle of lumbar lordosis. Another important finding was the weak correlation of the inclinometer in comparison to with the X-ray's measurements of the angle of lumbar lordosis for both the early and late growth stages, showing the inclinometer to be an inefficient instrument for monitoring the scoliotic curvature of the lumbar spine of adolescents with idiopathic scoliosis.
Acknowledgements
The authors acknowledge for help and support of the all the participants and Spine Group of the Institute of Medical Assistance to the State Public Hospital Servant and clinical center of the spine, in the state of Sao Paulo/SP, Brazil, during study.
Competing interests
The author(s) declared no potential conflicts of interest with respect to the research and/or publication.
Funding
This study has received funding from the National Council for Scientific and Technological Development (CNPq), Ministry of Science, Technology, Innovations and Communications of the Brazil under grant number: 458700/2014, São Paulo/SP. The funding bodies had no role in the design of the study, the data collection, data analysis, interpretation of the data or writing the manuscript.
ORCID Ana Paula Ribeiro https://orcid.org/0000-0002-1061-3789
Consent for publication
Not Applicable
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author (apribeiro@alumni.usp.br) on reasonable request.
Authors' contributions
All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors approved the final version to be published. Study conception, writing and design: AVS and APR. Acquisition of data and Statistics: AVS, RMA, NFN and APR. Analysis and interpretation of data: AVS, NFN and APR.

