










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO  uBio
uBio
Share

 Permalink
PermalinkRevista de Biología Tropical
On-line version ISSN 0034-7744Print version ISSN 0034-7744
Rev. biol. trop vol.62 n.3 San José Jul./Sep. 2014
Knowledge, perceptions, and practices with respect to the prevention of dengue in a mid-Pacific coastal village of Costa Rica
Conocimientos, percepciones y prácticas para prevenir el dengue en un pueblo costero del Pacífico central de Costa Rica
Abstract
Dengue fever is the fastest spreading, most prevalent and deadly arthropod-borne viral disease worldwide, present in over 125 countries. In 2013, Costa Rica is experiencing the highest number of Dengue infections since the virus’s reintroduction to the country in 1993. This study evaluated the Dengue-related knowledge of 320 community members, and polled opinions on how to better educate and mobilize the community on Dengue prevention in Quebrada Ganado, Costa Rica during March-May, 2013. In addition, property inspections were used to find relationships between knowledge or opinions and presence of Aedes breeding sites. Results showed that while citizens knew the virus is transmitted by mosquitoes that reproduce near water, they lacked knowledge on Aedes habits and confused it with other mosquitoes. Eighty-one percent of respondents assumed some responsibility for dengue prevention. Suggestions for improved education included consistent and continual information on the risks and dangers dengue poses to an individual. Characteristics relating to households with more positive breeding sites were: lower education level, higher prevalence of dengue infections in the household, lesser knowledge of dengue symptoms, a lower rating on the dangers of dengue and a lower rating on the importance of preventative actions. While a range of prevention methods are implemented, active community involvement is highly important for successful Dengue prevention. Continual evaluation is necessary to make more immediate, long-term behavioral societal changes, and to maximize the economic resources spent on Dengue prevention. Rev. Biol. Trop. 62 (3): 859-867. Epub 2014 September 01.
Key words: dengue fever, Costa Rica, social communication, Aedes aegypti, arbovirus, KAP.
Resumen
Entre las enfermedades virales transmitidas por artrópodos, el dengue es la más mortal y de difusión más rápida en el mundo. Es transmitida por los mosquitos Aedes, y está presente en más de 125 países. En 2013, Costa Rica tuvo el mayor porcentaje de casos de dengue desde la reintroducción del virus al país en 1993. Este estudio evaluó el conocimiento de 320 miembros de la comunidad costera de Quebrada Ganado, Costa Rica, quienes dieron sus opiniones acerca de cómo mejorar la educación y movilizar la comunidad en la prevención del dengue durante marzo y abril 2013. Además, mediante inspecciones de propiedades se trató de hallar conexiones entre el conocimiento u opiniones y la presencia de criaderos de Aedes. Aunque los habitantes sabían que el virus es transmitido por los mosquitos que se reproducen cerca del agua, no reconocían los hábitos del mosquito y lo confundían con otros mosquitos. El 81% acepta la responsabilidad por la prevención del dengue. Sugerencias para mejorar la educación incluyeron: información continua y frecuente sobre los riesgos, peligros y daños a la salud. Las características relacionadas con las propiedades que tenían más criaderos fueron: menor nivel de educación, mayor frecuencia de infecciones con dengue, menor entendimiento de los síntomas del dengue, menor calificación dada a los peligros del dengue y menor calificación dada a la importancia de las acciones preventivas. Mientras se pone en práctica una gama amplia de métodos de prevención del dengue, la participación activa de la comunidad es sumamente importante para el éxito de estas actividades. La evaluación continua es necesaria para lograr cambios inmediatos y a largo plazo en el comportamiento social y para aprovechar mejor los recursos económicos invertidos en la prevención del dengue.
Palabras clave: dengue, Costa Rica, comunicación social, Aedes aegypti.
Dengue fever is a viral illness caused by any one of the four DENV flavivirus serotypes (DENV1-DENV4). It is the most prevalent and deadly arthropod-borne human illness worldwide (Guzman & Kouri, 2002; Farrar et al., 2007; Ross, 2010) and is transmitted by mosquitoes of the genus Aedes, primarily Aedes aegypti. Infection with one serotype may cause dengue with or without warning signs, or severe dengue. Subsequent acquisition of different serotypes is associated with a weakened immune response and worsens the perspective for recuperation.
Dengue epidemics were reported in 1779, but no persistent infection patterns existed until World War II when a global dengue pandemic began (reviewed in Gubler, 1998). To this day, no dengue vaccine has been approved, and prevention methods rely heavily on diminishing the vector. In 1947 the Pan American Sanitary Bureau initiated a campaign to eradicate Aedes aegypti from the Western Hemisphere, and by 1961 Aedes was completely eradicated from many Latinamercan countries, including Costa Rica (Severo, 1955; Soper, 1963). While dengue continued to be a major health problem in Asia, the Americas remained clear approximately between 1950-1970 (Gubler, 1998). The eradication campaign ended, and during the 1970s the Pacific Islands were re-infected with the virus, leading to the spread of dengue across the Western Hemisphere once again (Gubler, 1998). Today the number of incidences of dengue is 30 times greater than it was 50yrs ago, with an estimated 390 million dengue infections annually (Bhatt et al., 2013) and 2.5 billion people living in areas of risk (WHO, 2009).
Exacerbated by increases in climatic temperatures, frequent intercontinental airline travel, booming, uncontrolled urbanization, inadequate municipal services, and vector adaptability, (Parks & Lloyd, 2004; Farrar et al., 2007; Miller, 2012) dengue is a pressing global health concern. Relatively successful, the country of Costa Rica remained free of dengue until an epidemic outbreak in 1993. Since 1993, infections have persisted and posed an increasing health threat in Costa Rica, and there is a severe gap in published dengue research in the country (Troyo, Porcelain, Calderón-Arguedas, Chadee, & Beier, 2006). In 2013 Costa Rica was declared to have the largest dengue epidemic since 1993, and by the end of August 2013 around 27 000 infections were reported.
Aedes aegypti maintains a lifestyle dependent on humans, and lives exclusively in human-populated areas (Trpis, Hausermann, & Craig, 1995). The female mosquito lays her eggs in clean water, and eggs can lay dormant for over a year in a dry state. While a number of options for diminishing the vector have been considered in the past 20yrs, including predation to kill the mosquitoes, fumigation, and shorter-lived organophosphate insecticides, these methods are not successfully executed and are difficult to manage without community participation. Aedes breeding is often propagated by the failure to remove breeding sites, such as old tires, flower vases, random garbage, and even pop bottle caps that should be properly disposed of. Studies show that in working to eliminate dengue, community education and involvement are crucial (Espinoza-Gómez, Hernández-Suárez, & Coll-Cárdenas, 2002; Parks & Lloyd, 2004; Martín & Prado, 2004; Nam et al., 2005), yet much effort is still needed to optimize community involvement (Toledo-Romaní, Baly-Gil, Ceballos-Ursula, Boelaert, & Van der Stuyft, 2006).
In order to combat dengue and eradicate the vector, the Pan-American Health Organization, national health care system and the Ministry of Health of Costa Rica designed a plan in 2005. The plan, EGI (Spanish for Integrative Management Strategy), has five integrated components, one of which is social communication. A goal of social communication is to mobilize public participation in eliminating the vector; however, attaining and maintaining long-lasting behavioral changes in a community is a difficult task (Parks & Lloyd, 2004). It was reported that public education regarding dengue knowledge is relatively strong in Costa Rica, yet education on attitudes and beneficial practices has not been well provided (Solís, Quesada, & Gutiérrez, 2010).
This study aimed to evaluate and report on the current status of the residents’ knowledge, perceptions and actions in regards to dengue in the small, mid-Pacific coastal village Quebrada Ganado, Puntarenas, Costa Rica.
Materials and Methods
Study site: The study site was Quebrada Ganado, Puntarenas, Costa Rica (hereafter referred to as Quebrada, or QG), (9.72ºN - 84.63ºW), with a population of 1 916 (967 males, 949 females) (INEC, 2011). Before the study began, QG had 40 confirmed and reported cases of dengue in the first 16wks of 2013 (Ministry of Health). The town has 754 residences including 583 occupied and 171 unoccupied (INEC, 2011). Ninety-nine percent of the houses (582/583) have internal running water, and 99% (577/583) have a television (INEC, 2011). In general, houses are very close together and space is concentrated, including a community center, soccer field, kindergarten, pharmacy, primary and secondary schools, and public health clinic. The most commonly-reported resident occupations are personal services, cleaning services, sales and construction (INEC, 2011).
Study design: To correlate resident knowledge and attitudes with their respective property, and to evaluate the behavior of QG citizens, only citizens at residential properties were interviewed. Our 25-item interview was adapted from a similar interview designed to aid the Ministry of Health (MH) in a 2004 study (R. Baxter, unpublished). All interviews took place in March and April, 2013. Interview procedures, including interviewee verbal consent protocol, were approved by the Ethics Review Board of the Associated Colleges of the Midwest, Chicago, Illinois.
Household inspections were carried out during March through May, 2013 by employees of the Vector Control sector of the Garabito Ministry of Health of Costa Rica. As part of the EGI branch of Entomological Surveillance, MH workers inspect properties for possible and positive Aedes breeding sites, and educate owners about dengue prevention.
All answers were directly recorded on an interview sheet. Independent of how many people were present in the house, only one person was asked to respond. All respondents were at least 18 years of age, lived in the house, and as often as possible, managed household decisions. To avoid influence by recent in-house education by MH employees, we interviewed 182 households with no previous recent MH visit. These properties were inspected after the interview. An additional 37 interviews were conducted directly after a MH inspection, and 45 interviews were conducted in households that had an inspection two months prior. Fifty-six interviews were conducted in households with no previous inspection, and no MH inspection data following the interview were available for these houses.
All data were entered in Microsoft Excel and rechecked. Dependency of type of water used for mosquito breeding with prior education by MH was tested with a contingency table. The relationship between Likert scale or other types of responses for various independent and dependent variables of interest were estimated by simple linear regression. Differences in mean Likert scale responses between various groupings of participants were estimated with one-way parametric ANOVA. Assumptions of homogeneity of variance were tested and posterior comparisons between means were carried out with LSD, Tukey or Scheffe tests. Statistical procedures followed Sokal & Rohlf (1995). Analysis of variance and linear regression analyses were conducted using Statgraphics Centurion XVI (Statpoint Technologies, Inc., 2011).
Results
Tables and additional comments appear as Digital Appendices. The rest of the results are detailed below.
Sample demographics: Of the 19 city blocks in the study site, 18 blocks were visited and 320 citizens were interviewed. This included 242 (76%) females and 78 (24%) males. Median age was 40 with a range from 18 to 86. Twenty-three (7%) participants had no education, 167 (52%) had received education at the primary level, 102 (32%) at the secondary level and 28 (9%) up to university level. Fifty-three percent of participants were stay-at-home mothers or not employed, 14% were blue-collar workers (construction, packing, maintenance, fishing, among others), 13% worked in a restaurant, tourism, or as a cashier and the other 20% were employed in 10 other sectors including childcare, independent work and security. Sixty-five percent of those interviewed owned their home or paid mortgage and 35% rented.
Citizen history with dengue and familiarity: Sixty-one percent of participants reported someone in their house had been previously infected with dengue and 21 (11%) of these participants reported it to be “hemorrhagic”. According to the previous WHO guidelines for dengue classification, community members were more familiar with this terminology than with the newer classification of “severe dengue.” Thirty-nine percent had no house-member with previous infection. Of those who reported a previous infection in the house, an average of two people in the house had contracted dengue and on average one time ranging from a reported one to six times.
Participants were asked to list the symptoms of dengue fever, and 89% of participants could state three or more symptoms. We designated three or more symptoms as an adequate understanding of the symptoms of dengue. The most common symptoms mentioned were fever (285 participants, 89%), headache (209 participants, 65%), body pain (134 participants, 42%), vomiting (122 participants, 38%), and rash (105 participants, 33%). Of those who had an adequate understanding, participants mentioned up to nine symptoms (n=2); with a mean, median and mode of four symptoms. Participants with previous acquisition were more knowledgeable of the symptoms, (F=76.6; df=1, 318; p<0.0001, R2=19.41%).
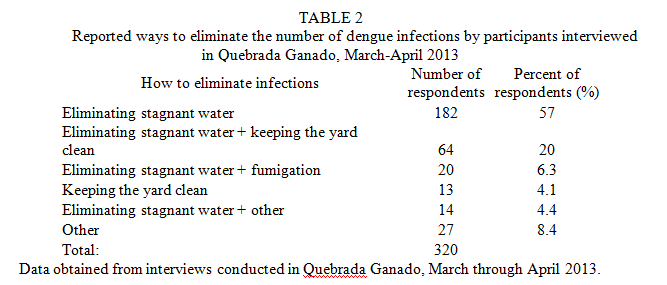
Citizen knowledge: Three hundred fifteen (98%) participants knew that dengue is transmitted by a mosquito and 98% knew that the mosquito reproduces in stagnant water. It became evident that the town has common knowledge that mosquitoes reproduce in water, but they grossly generalize all mosquitoes, specifically those around dirty street water, to carry dengue. When this generalization became evident, we began asking participants (n=253) what kind of water is preferred by the mosquitoes that transmit dengue. As previously noted, participants were interviewed either before or after an inspection by the Ministry of Health workers (Table 1) (Appendix 1). Participants reported clean water more often if their house had been inspected by a Ministry of Health worker 5wks prior, compared with the participants with no previous house inspection (x2=8.88; df=1; p=0.0029). Education from MH inspections had an effect on community knowledge 5 weeks later. When asked how to decrease the number of dengue infections in the community, 280 participants (88%) mentioned eliminating stagnant water (Table 2) (Appendix 1).
Community concerns: When asked for the “most severe problem in the community”, 20 people (6%) reported a lack of available appointments in the clinic, 12 people (4%) reported garbage thrown in the streets and river, nine (3%) reported poor management of water in the streets, five (1.6%) reported inconsideration for the environment, four (1.3%) reported non-efficient political organizations, and dengue or excess of mosquitoes was reported by 13 (5%). The most common answer was illegal drug use (29%, 94 people).
When asked for the “principal health problem in QG”, an overwhelming 160 (50%) participants reported dengue. Six (2%) reported their concern for contaminated, stagnant water in the streets, and four (1.3%) reported a plague of mosquitoes.
Citizen perceptions: When asked: How dangerous it is for a person to get infected with dengue? 157 (52%) respondents said it is very dangerous, 125 (42%) said it is dangerous, and 18 (6%) said it is not dangerous, or they did not know. Mean response for danger level was greater for respondents that had a house member with previous dengue infection (
 =2.52 on scale from 1-3) when compared to the mean response for respondents who had no house member previously infected (=2.32) (F=5.97; df=1, 298; p=0.015).
=2.52 on scale from 1-3) when compared to the mean response for respondents who had no house member previously infected (=2.32) (F=5.97; df=1, 298; p=0.015). Two hundred twelve (71%) respondents reported that “actions on dengue prevention” are very important, 75 (25%) reported the actions are important, three (1%) reported the actions are not important, and 10 (3%) reported they did not know. Mean response for perceived “importance of actions on dengue prevention” were greater for participants with a previously infected house member (
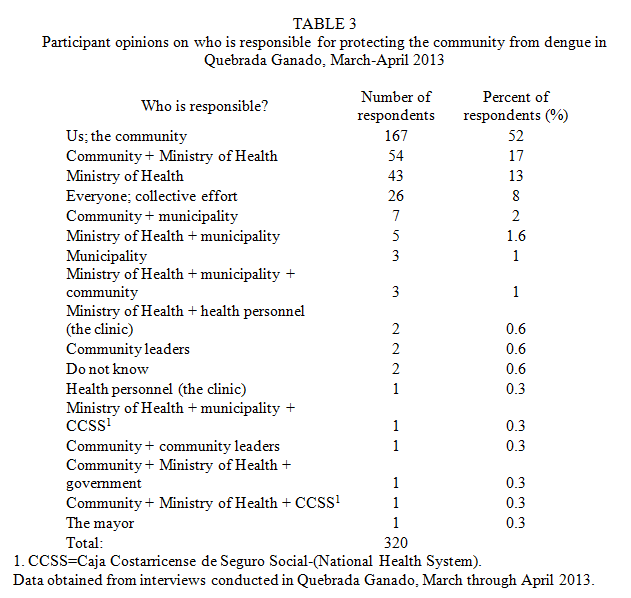
=2.74) than for those with no previous household infection (=2.46) (F=13.23; df=1, 298; p=0.0003). Similarly, respondents’ rating on the “importance of actions on dengue prevention” was greater for respondents who could name “three or more dengue symptoms” (=2.66) compared to those who could not (=2.38) (F=5.25; df=1, 298; p=0.0227). Similarly, those who could name “three or more dengue symptoms” perceived a greater “danger of infection” (=2.46) than those who could not (=2.29) (F=1.77; df=1, 298; p=0.18). Citizen opinions on responsibility and effective dengue education in the community: The last three questions in the interview were used to gather community views, opinions and advice on dengue prevention within their community. In response to the question: Who has the responsibility of protecting the community from dengue? 167 (52%) reported it was their responsibility entirely, 29% responded the community has responsibility along with other organizations, and 19% did not include the community in their response (Table 3) (Appendix 1).
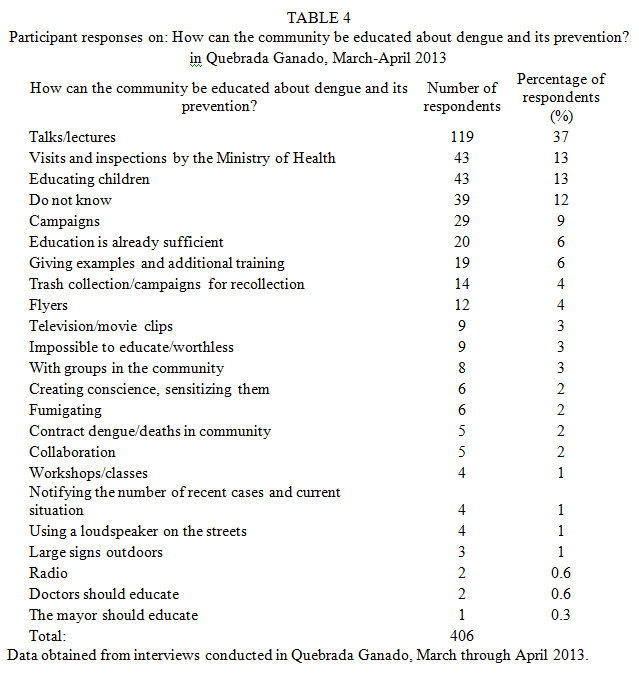
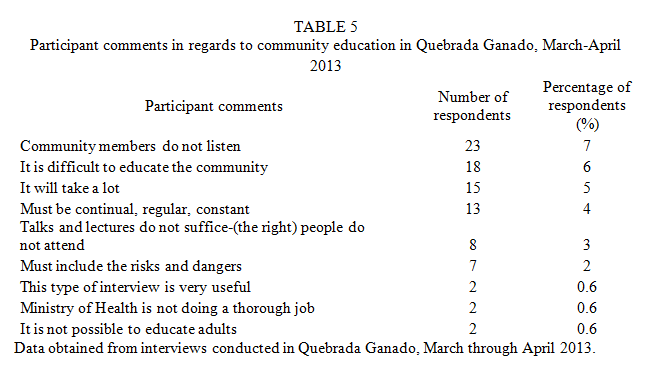
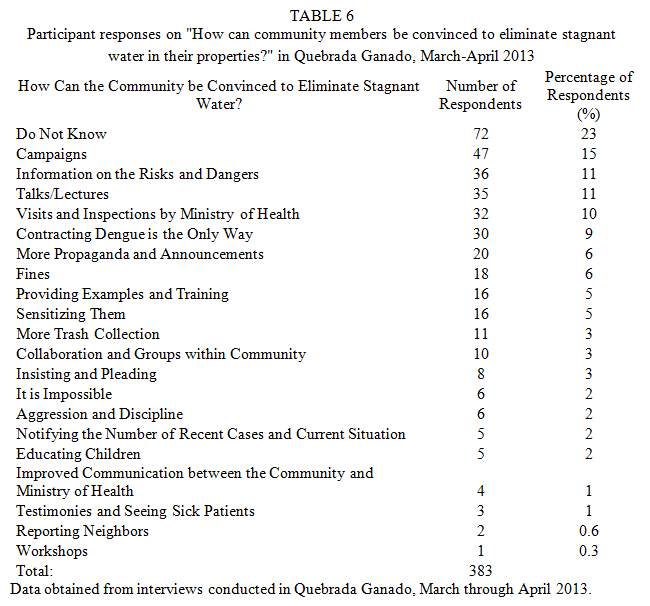
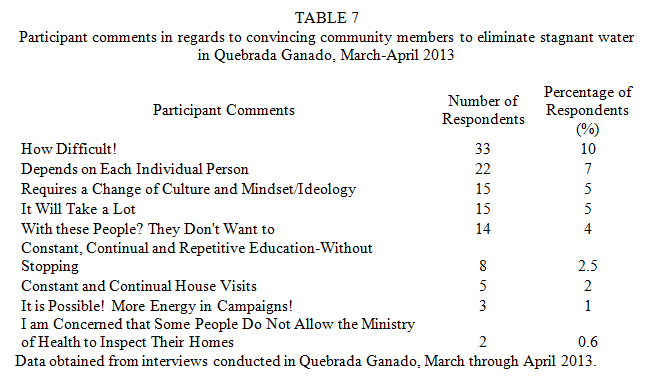
We asked participants: How the community can be educated on dengue and its prevention? and 406 responses were received. Response frequencies from the 320 participant total were calculated as percentages (Table 4) (Appendix 1). Many comments on dengue education were also offered, and some of the most common comments were recorded (Table 5) (Appendix 1). We also asked: How community members can be convinced to eliminate breeding sites on their properties? (Table 6) (Appendix 1), and additional comments were recorded (Table 7) (Appendix 1).
Citizen practices: Based on 264 properties inspected by MH employees, all 264 properties (100%) had possible breeding sites. Mean number of possible breeding sites per house was 8.5 (median=7, mode=5, and ranged from 2-51 per house). Nine percent of the properties inspected had at least one breeding site positive for Aedes aegypti larvae or pupas (n=24). The quantity of positive breeding sites found on each property ranged from 0 to 6, and included a variety of receptacles, including small buckets, flowerpots, and appliances not in use. The maximum number of times a house member had been infected by dengue was positively related to the number of possible breeding sites at that house (F=5.51; df=1, 261; p=0.0196; R2=2.07). Houses with more possible breeding sites had more positive breeding sites for A. aegypti larva/pupa (F=142; df=1, 263; p<0.0001; R2=35.17).
Citizen trends and predictive factors: Having a previous infection or knowledge of dengue symptoms did not have a significant relationship with the number of breeding sites found during inspections. Among the knowledge and demographic factors collected, participant education level had the greatest relationship to number of positive breeding sites found in inspections (negative relationship) (F=5.92; df=1, 262; p=0.0156; R2=2.21). The number of positive breeding sites was also greater in homes where a) the respondent rated a lower importance on the actions of dengue prevention (F=5.08; df=1, 244; p=0.0251; R2=2.05) and b) the rating for dengue danger was lower (F=5.08; df=1, 244; p=0.0223; R2=2.13).
Discussion
As with other studies, most often women of the house were available for interviewing (de María Cáceres-Manrique, Vesga-Gómez, Perea-Florez, Ruitort, & Talbot, 2009; Zuleta et al., 2011). Based on our total sample size of 42.4% of the residences in QG, the majority of townspeople reported having had a dengue infection in their household (61%). Nine in ten citizens (90%) have an adequate understanding of the fever’s symptoms, indicating they understand dengue fever well, which is comparatively high (Panagos, Lacy, Gubler, & Macpherson, 2005). An overwhelming 98% understand that dengue is transmitted by a mosquito, but think erroneously that the mosquito proliferates in stagnant water. However, a portion of participants reported false positive dengue cases. They reported up to six distinct dengue infections, which is not possible with four serotypes. Citizens also had a defined confusion on the characteristics of the dengue vector. Previous studies have shown a similar trend where communities are familiar with dengue and mosquitoes, but have a poorer understanding of the relationship between the mosquito, human behavior and transmission (Panagos et al., 2005).
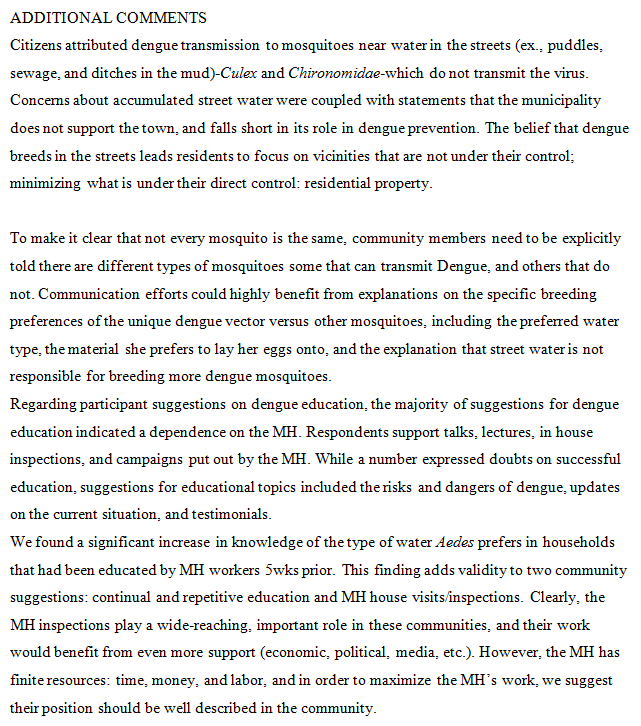
Citizens were not well educated on the differences in mosquito niches, leaving them to perceive “a mosquito is a mosquito,” hence, all mosquitoes transmit dengue. For example, citizens were preoccupied that dengue was spread by mosquitoes that are often found in areas where Aedes does not reproduce. They failed to focus on the primary breeding sites the dengue vector prefers: receptacles or other items with solid, flat surfaces that hold clean water in residential areas. Previous studies similarly reported participants failed to recognize mosquitos in their house as the dengue vector (Pérez-Guerra, Seda, García-Rivera, & Clark, 2005; Torres-López, Guerrero-Cordero, & Salazar-Estrada, 2012). Reported social barriers include a lack of responsibility and a muted concern of the disease (Pérez, Zielinski, Vargas, & Clark, 2009), especially due to hazy information (Torres-López et al., 2012). We believe the inability to differentiate and identify practices between mosquitoes may lead to this lack of responsibility and a muted concern, as well as the failure to mobilize in QG.
The primary role communities play in reducing the risk for dengue is to remove receptacles on their property (San Martin & Prado, 2004), and the role of community participation needs to be unified within a community (Toledo-Romaní et al., 2006). A blurry understanding of Aedes habits mutes the relevancy and urgency for community members to play their part. By comprehending the distinctions of the dengue vector, community members will understand the reason they must review their lawns diligently, and unify on their participatory role.
Regarding community views on dengue responsibility, eight in ten (81%) respondents said the community is at least partially responsible for dengue prevention; however, about 20 percent do not claim any responsibility. This is a concern because a mindset of responsibility and ownership leads citizens to act. Citizens reported the best ways to convince community members to eliminate stagnant water were through: campaigns, information on risks and dangers, talks and lectures and the work by the MH. That is, the number one way to convince members to act is through more information and education.
The next most popular response was that contracting dengue is the only way to convince members to act; indicating personal experience is the best teacher. About one in three respondents expressed doubts in convincing other community members to take preventative actions. This stems from a long-standing culture that community members expect their neighbor will not take action and remove breeding sites on their property. For example, in the town it is “normal” to litter, therefore watching a neighbor throw trash on the street is acceptable. In order to change this norm, each member has to not only take individual ownership, but collaborate with others. This attitude of pointing the finger at one’s neighbors is not unique to this community (Pérez-Guerra et al., 2005, Torres-López et al., 2012). But members need to take ownership, challenge norms, and even expand their personal responsibilities. Some community members are physically unable to independently review their lawns adequately, such as the elderly. These people need family members or neighbors to step in for them.
Respondents also suggested dengue education needs to be frequent, continual and non-stop, because community members are human and therefore tend to “forget” if information is not brought up often. This report reflects one of the tenets of Communication for Behavior Impact (COMBI) put out by the WHO: sustained appropriate advertising which is massive, repetitive, intense and persistent (Parks & Lloyd, 2004), which has been supported in other studies as well (Khun & Manderson, 2007).
Regarding MH vector control inspections, MH workers inspect properties to remove and prevent Aedes breeding sites, and to educate citizens on dengue and its prevention. The MH visits and inspections were of the most common suggestions on how to educate and even to convince community members on dengue and its prevention. Other communities have similarly requested house visits (Zuleta et al., 2011) to explain specific control measures (Pérez-Guerra et al., 2005). The use of dialogue has been stressed in the transition from critical understanding to critical action (Freire, 1973), and a house visit provides a great opportunity for one-on-one dialogue with MH educators and residents.
House visits and family education require many trained vector control workers, and a lot of time. Additionally, some citizens report that the MH has abandoned their position in dengue control because they fumigate much less than before. The request for fumigation has been reported in other communities as well (Pérez-Guerra et al., 2005). However, an over-dependence on fumigation or repeated house visits diminishes the community’s ownership and perceived responsibility to review their own properties for breeding sites. There is a misunderstanding that fumigation equals support in fighting dengue. This aim should be openly communicated with community members so they do not get the incorrect impression that the MH is retracting its position or support in dengue control by decreasing the frequency of fumigation.
Regarding target audience characteristics to consider, dengue perceptions have been shown to vary based on previous acquisition (Pérez et al., 2009). We similarly found that respondents who have had a dengue infection in the household perceive dengue to be more dangerous, and they consider the actions of prevention to be more important. Respondents who were familiar with dengue symptoms were also stronger supporters of preventative actions. This indicates if people are more aware of dengue symptoms, they may be more inclined to prevent the disease. This supports the educational goal to highlight the symptoms of dengue and risks it poses to an individual (Pérez et al., 2009).
To avoid “preaching to the choir,” dengue education needs to target the right audience. According to our findings, we compiled the following characteristics which suggest the target audience should include people who: do not live with anyone previously infected by dengue, do not understand the symptoms of dengue, have more frequent infections in the household (relates to more possible breeding sites), have a low education level (Rosenbaum et al., 1995, Syed et al., 2010), rate the importance of actions on dengue prevention lower (which relates to more positive breeding sites), rate dengue to be less dangerous (which relates to more positive breeding sites), and have more possible breeding sites on their property (which relates to more positive breeding sites).
Acknowledgments
A special thank you goes to Chris Vaughan, Michael McCoy, Mario Morera, Judith Magnan, Jaime Rodríguez Arguedas, José Valerín Cordero, Maynor Peraza Solas, Zulema Conejo Mora, Luis Guillermo Chaverri, Nick Bohrer, and above all, the community members of QG.
References
Bhatt, S., Gething, P. W., Brady, O. J., Messina, J. P., Farlow, A. W., Moyes & Hay, S. I. (2013). The global distribution and burden of dengue. Nature, 496(7446), 504-507. [ Links ]
de María Cáceres-Manrique, F., Vesga-Gómez, C., Perea-Florez, X., Ruitort, M., & Talbot, Y. (2009). Conocimientos, actitudes y prácticas sobre dengue en dos barrios de Bucaramanga, Colombia. Revista de Salud Pública, 11(1), 27-38. [ Links ]
Espinoza-Gómez, F., Hernandez-Suarez, C. M., & Coll-Cárdenas, R. (2002). Educational campaign versus malathion spraying for the control of Aedes aegypti in Colima, Mexico. Journal of Epidemiology and Community Health, 56(2), 148-152. [ Links ]
Farrar, J., Focks, D., Gubler, D., Barrera, R., Guzman, M. G., Simmons, C., & Kroeger, A. (2007). Editorial: Towards a global dengue research agenda. Tropical Medicine & International Health, 12(6), 695-699. [ Links ]
Freire, P. (1973). Education for critical consciousness. New York, NY, USA: Seabury. [ Links ]
Gubler, D. J. (1998). Dengue and dengue hemorrhagic fever. Clinical Microbiology Review, 11(3), 480-496. [ Links ]
Guzman, M. & Kouri, G. (2002). Dengue: An update. The Lancet Infectious Diseases 2(1), 33-42. [ Links ]
INEC (Instituto Nacional de Estadística y Censos) (2011). Estadística Censo 2011. Retrieved from Área de Servicios de Información y Divulgación. San José, Costa Rica. [ Links ]
Khun, S. & Manderson, L. (2007). Community and school-based health education for dengue control in rural Cambodia: A process evaluation. PLoS Neglected Tropical Diseases, 1(3), e143. [ Links ]
Martín, J. L. & Prado, M. (2004). Risk perception and strategies for mass communication on dengue in the Americas. Revista Panameña de Salud Pública, 15(2), 135-139. [ Links ]
Miller, A. (2012). UN atlas links climate change to disease spread. Canadian Medical Association Journal, 185(1), E38. [ Links ]
Nam, V. S., Yen, N. T., Phong, T. V., Ninh, T. U., Mai, L. Q., Lo, L.V., & Kay, B. (2005). Elimination of dengue by community programs using mesocyclops (copepod) against Aedes aegypti in central Vietnam. The American Journal of Tropical Medicine and Hygiene, 72(1), 67-73. [ Links ]
Panagos, A., Lacy, E. R., Gubler, D. J., & Macpherson, C. N. (2005). Dengue in Grenada. Revista Panamericana de Salud Pública,17(4), 225-229. [ Links ]
Parks, W. & Lloyd, L. (2004). Planning social mobilization and communication for dengue fever prevention and control: A step-by-step guide. Geneva, Switzerland: World Health Organization. [ Links ]
Pérez, C. L., Zielinski, E., Vargas, D., & Clark, G. G. (2009). Community beliefs and practices about dengue in Puerto Rico. Revista Panameña de Salud Publica, 25, 218-226. [ Links ]
Pérez-Guerra, C. L., Seda, H., García-Rivera, E. J., & Clark, G. G. (2005). Knowledge and attitudes in Puerto Rico concerning dengue prevention. Revista Panameña de Salud Pública, 17(4), 243-253. [ Links ]
Rosenbaum, J., Natahan, M. B., Ragoonanansingh, R., Rawlins, S., Gayle, C., Chadee, D. D., & Lloyd, L. S. (1995). Community participation in dengue prevention and control: A survey of knowledge, attitude and practice in Trinidad and Tobago. American Journal of Tropical Medicine and Hygiene, 53(2), 111-117. [ Links ]
Ross, T. M. (2010). Dengue virus. Clinics in Laboratory Medicine, 30(1), 149-160. [ Links ]
San Martín, J. L. & Prado, M. (2004). Percepción del riesgo y estrategias de comunicación social sobre el dengue en las Américas. Revista Panameña de Salud Pública, 15(2), 135-139. [ Links ]
Severo, O. P. (1955, September), Eradication of the Aedes aegypti mosquito from the Americas. Paper presented at “Yellow fever, a symposium in commemoration of Carlos Juan Finlay” Paper 6 of Jefferson Medical College, Philadelphia. Retrieved from http://jdc.jefferson.edu/yellow_fever_symposium/6 [ Links ]
Sokal, R. R. & Rohlf, F. J. (1995). Biometry: The principles and practice of statistics in biological research. New York, NY, USA: W. H. Freeman & Co. [ Links ]
Solís, M. I., Quesada, M., & Gutiérrez, I. (2010). Knowledge, attitudes and practices against the dengue fever promoted by Costa Rican media. Revista Costarricense de Salud Pública, 19, 88-92. [ Links ]
Soper, F. L. (1963). The elimination of urban yellow fever in the Americas through the eradication of Aedes aegypti. American Journal of Public Health and the Nation’s Health, 53(1), 7-16. [ Links ]
Statpoint Technologies, Inc. (2011). Statgraphics Centurion [computer software]. Retrieved from http://www.statgraphics.com. [ Links ]
Syed, M., Saleem, T., Syeda, U., Habib, M., Zahid, R., Bashir, A., & Saleem, S. (2010). Knowledge, attitudes and practices regarding dengue fever among adults of high and low socioeconomic groups. Journal of Pakistan Medical Association, 60(3), 243-247. [ Links ]
Toledo-Romaní, M. E., Baly-Gil, A., Ceballos-Ursula, E., Boelaert, M., & Van der Stuyft, P. (2006). Participación comunitaria en la prevención del dengue: Un abordaje desde la perspectiva de los diferentes actores sociales. Salud Pública de México, 48(1), 39-44. [ Links ]
Torres-López, T. M., Guerrero-Cordero, J. L., & Salazar-Estrada, J. G. (2012). Dimensiones culturales del dengue que favorecen o dificultan su prevención en México. Revista Panameña de Salud Pública, 31(3), 197-203. [ Links ]
Troyo, A., Porcelain, S. L., Calderón-Arguedas, O., Chadee, D. D., & Beier, J. C. (2006). Dengue in Costa Rica: The gap in local scientific research. Revista Panameña de Salud Public, 20(5), 350-360. [ Links ]
Trpis, M., Hausermann, W., & Craig, G. B. (1995). Estimates of population size, dispersal, and longevity of domestic Aedes aegypti aegypti (Diptera:Culicidae) by mark-release-recapture in the village of Shauri Moyo in eastern Kenya. Journal of Medical Entomology, 32(1), 27-33. [ Links ]
WHO (World Health Organization). (2009). Dengue: Guidelines for diagnosis, treatment, prevention and control-new edition. Geneva, Switzerland: WHO. [ Links ]
Zuleta, L. P., Garzón, A., Pérez, R., Rodríguez, E., Fonseca, J., & Cano, F. (2011). Caracterización de conductas relacionadas con dengue, Yopal, Casanare, Colombia, 2010. Informe Quincenal Epidemiológico Nacional, 16(17), 203-215. [ Links ]
de María Cáceres-Manrique, F., Vesga-Gómez, C., Perea-Florez, X., Ruitort, M., & Talbot, Y. (2009). Conocimientos, actitudes y prácticas sobre dengue en dos barrios de Bucaramanga, Colombia. Revista de Salud Pública, 11(1), 27-38. [ Links ]
Espinoza-Gómez, F., Hernandez-Suarez, C. M., & Coll-Cárdenas, R. (2002). Educational campaign versus malathion spraying for the control of Aedes aegypti in Colima, Mexico. Journal of Epidemiology and Community Health, 56(2), 148-152. [ Links ]
Farrar, J., Focks, D., Gubler, D., Barrera, R., Guzman, M. G., Simmons, C., & Kroeger, A. (2007). Editorial: Towards a global dengue research agenda. Tropical Medicine & International Health, 12(6), 695-699. [ Links ]
Freire, P. (1973). Education for critical consciousness. New York, NY, USA: Seabury. [ Links ]
Gubler, D. J. (1998). Dengue and dengue hemorrhagic fever. Clinical Microbiology Review, 11(3), 480-496. [ Links ]
Guzman, M. & Kouri, G. (2002). Dengue: An update. The Lancet Infectious Diseases 2(1), 33-42. [ Links ]
INEC (Instituto Nacional de Estadística y Censos) (2011). Estadística Censo 2011. Retrieved from Área de Servicios de Información y Divulgación. San José, Costa Rica. [ Links ]
Khun, S. & Manderson, L. (2007). Community and school-based health education for dengue control in rural Cambodia: A process evaluation. PLoS Neglected Tropical Diseases, 1(3), e143. [ Links ]
Martín, J. L. & Prado, M. (2004). Risk perception and strategies for mass communication on dengue in the Americas. Revista Panameña de Salud Pública, 15(2), 135-139. [ Links ]
Miller, A. (2012). UN atlas links climate change to disease spread. Canadian Medical Association Journal, 185(1), E38. [ Links ]
Nam, V. S., Yen, N. T., Phong, T. V., Ninh, T. U., Mai, L. Q., Lo, L.V., & Kay, B. (2005). Elimination of dengue by community programs using mesocyclops (copepod) against Aedes aegypti in central Vietnam. The American Journal of Tropical Medicine and Hygiene, 72(1), 67-73. [ Links ]
Panagos, A., Lacy, E. R., Gubler, D. J., & Macpherson, C. N. (2005). Dengue in Grenada. Revista Panamericana de Salud Pública,17(4), 225-229. [ Links ]
Parks, W. & Lloyd, L. (2004). Planning social mobilization and communication for dengue fever prevention and control: A step-by-step guide. Geneva, Switzerland: World Health Organization. [ Links ]
Pérez, C. L., Zielinski, E., Vargas, D., & Clark, G. G. (2009). Community beliefs and practices about dengue in Puerto Rico. Revista Panameña de Salud Publica, 25, 218-226. [ Links ]
Pérez-Guerra, C. L., Seda, H., García-Rivera, E. J., & Clark, G. G. (2005). Knowledge and attitudes in Puerto Rico concerning dengue prevention. Revista Panameña de Salud Pública, 17(4), 243-253. [ Links ]
Rosenbaum, J., Natahan, M. B., Ragoonanansingh, R., Rawlins, S., Gayle, C., Chadee, D. D., & Lloyd, L. S. (1995). Community participation in dengue prevention and control: A survey of knowledge, attitude and practice in Trinidad and Tobago. American Journal of Tropical Medicine and Hygiene, 53(2), 111-117. [ Links ]
Ross, T. M. (2010). Dengue virus. Clinics in Laboratory Medicine, 30(1), 149-160. [ Links ]
San Martín, J. L. & Prado, M. (2004). Percepción del riesgo y estrategias de comunicación social sobre el dengue en las Américas. Revista Panameña de Salud Pública, 15(2), 135-139. [ Links ]
Severo, O. P. (1955, September), Eradication of the Aedes aegypti mosquito from the Americas. Paper presented at “Yellow fever, a symposium in commemoration of Carlos Juan Finlay” Paper 6 of Jefferson Medical College, Philadelphia. Retrieved from http://jdc.jefferson.edu/yellow_fever_symposium/6 [ Links ]
Sokal, R. R. & Rohlf, F. J. (1995). Biometry: The principles and practice of statistics in biological research. New York, NY, USA: W. H. Freeman & Co. [ Links ]
Solís, M. I., Quesada, M., & Gutiérrez, I. (2010). Knowledge, attitudes and practices against the dengue fever promoted by Costa Rican media. Revista Costarricense de Salud Pública, 19, 88-92. [ Links ]
Soper, F. L. (1963). The elimination of urban yellow fever in the Americas through the eradication of Aedes aegypti. American Journal of Public Health and the Nation’s Health, 53(1), 7-16. [ Links ]
Statpoint Technologies, Inc. (2011). Statgraphics Centurion [computer software]. Retrieved from http://www.statgraphics.com. [ Links ]
Syed, M., Saleem, T., Syeda, U., Habib, M., Zahid, R., Bashir, A., & Saleem, S. (2010). Knowledge, attitudes and practices regarding dengue fever among adults of high and low socioeconomic groups. Journal of Pakistan Medical Association, 60(3), 243-247. [ Links ]
Toledo-Romaní, M. E., Baly-Gil, A., Ceballos-Ursula, E., Boelaert, M., & Van der Stuyft, P. (2006). Participación comunitaria en la prevención del dengue: Un abordaje desde la perspectiva de los diferentes actores sociales. Salud Pública de México, 48(1), 39-44. [ Links ]
Torres-López, T. M., Guerrero-Cordero, J. L., & Salazar-Estrada, J. G. (2012). Dimensiones culturales del dengue que favorecen o dificultan su prevención en México. Revista Panameña de Salud Pública, 31(3), 197-203. [ Links ]
Troyo, A., Porcelain, S. L., Calderón-Arguedas, O., Chadee, D. D., & Beier, J. C. (2006). Dengue in Costa Rica: The gap in local scientific research. Revista Panameña de Salud Public, 20(5), 350-360. [ Links ]
Trpis, M., Hausermann, W., & Craig, G. B. (1995). Estimates of population size, dispersal, and longevity of domestic Aedes aegypti aegypti (Diptera:Culicidae) by mark-release-recapture in the village of Shauri Moyo in eastern Kenya. Journal of Medical Entomology, 32(1), 27-33. [ Links ]
WHO (World Health Organization). (2009). Dengue: Guidelines for diagnosis, treatment, prevention and control-new edition. Geneva, Switzerland: WHO. [ Links ]
Zuleta, L. P., Garzón, A., Pérez, R., Rodríguez, E., Fonseca, J., & Cano, F. (2011). Caracterización de conductas relacionadas con dengue, Yopal, Casanare, Colombia, 2010. Informe Quincenal Epidemiológico Nacional, 16(17), 203-215. [ Links ]
1. Associated Colleges of the Midwest, San Pedro, Costa Rica.
Lake Forest College, Lake Forest, IL 60045 USA; egeduvl@mx.lakeforest.edu
2. Ministerio de Salud, Área Rectora Garabito Jacó, Puntarenas, Costa Rica; rpc_garabito@ministeriodesalud.go.cr
3. Universidad Nacional, Costa Rica; anabellealfaro@gmail.com
Received 20-iii-2014. Corrected 12-iv-2014. Accepted 13-v-2014.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}