










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkActa Médica Costarricense
On-line version ISSN 0001-6002Print version ISSN 0001-6012
Acta méd. costarric vol.63 n.3 San José Jul./Sep. 2021
http://dx.doi.org/10.51481/amc.v63i3.1138
Original
Trends in admissions to Emergency Services during the COVID-19 pandemic

1Caja Costarricense de Seguro Social, CCSS, Hospital Nacional de Niños “Dr. Carlos Sáenz Herrera”, Servicio de Emergencias. San José, Costa Rica.0000-0002-8251-2434
2Caja Costarricense de Seguro Social CCSS, Hospital San Vicente de Paul, Servicio de Emergencias. Heredia, Costa Rica. 0000-0001-7308-5760
3Caja Costarricense de Seguro Social, CCSS, Hospital Rafael Calderón Guardia, Servicio de Emergencias. San José, Costa Rica. 0000-0002-2646-5020
Emergency Services (SEM) worldwide are a vital resource to ensure the provision of health services to users with the most critical conditions. In December 2019, a new viral disease caused by the SARS-CoV-2 coronavirus was identified, which originates in the city of Wuhan - China,1 giving a rapid spread to the rest of the world and identifying the first case in Europe in France on January 25, 2020,2 In the American continent the first case was identified in the United States on January 21 of the same year, and quickly countries around the world report positive cases of COVID-19, so the World Health Organization declares March 11 as a pandemic, just 5 days after the first case was identified in Costa Rica.3
This disease has taken most of the world’s health systems by surprise, forcing them to make adaptations not only in infrastructure, but also in the flow of care at the first levels of care, as well as in Hospital Services, including Emergency Care, and in the inpatient areas.4 For Emergency Services, the constant adaptations, and transformations carried out in the shortest possible time have been a challenge in order to provide care not only to patients with SARS CoV2 disease, but also to continue the usual care for all other emergencies. The redefinition of spaces and reorganization of human resources, among other aspects, had to be carried out in a fast and organized way, very similar to other countries in the world. 4,5
Published studies have shown declines in the use of health services for elective and emergency conditions in the months following the pandemic declaration. 6,7
Reductions in SEM use could reflect the difficulty of patients with serious illnesses or lifethreatening conditions to seek care, including non- COVID-19 conditions7; another reason could be the avoidance of non-emergency SEM use; or the shift of emergency care to other settings, such as the use of telemedicine.8
In Costa Rica, a decrease in SEM care was observed at the beginning of the pandemic. The nature of this phenomenon, its duration, as well as its implications are not fully known at this time, and no data published for Central America can be found in the international literature. The objective of this study was to describe this phenomenon, its duration, as well as its implications in our country.
Methods
This was a retrospective observational descriptive study of the Emergency Services admissions in the hospitals belonging to the Caja Costarricense del Seguro Social (CCSS) from January 1st to December 31st, 2020. Data from Emergency Services that meet the operational definition described below were included.
The study of the indicators for the Emergency Services was approved as an administrative study by the Medical Manager of the CCSS with official letter GMMDA- 14314-2019 and did not require review by an Ethics Committee or Institutional review Board.
Operational Definitions:
• Emergency Service: 9
An Emergency Services is the area of the hospital center intended for the initial assessment, early diagnosis, and timely treatment of patients with a wide spectrum of diseases or injuries that can be life-threatening or condition their organic functionality. All of these require rapid attention as they are time dependent. They are characterized by their wide availability of schedules (24 hours, 7 days a week and 365 days a year) and a resolution capacity according to their level of functional classification (hospital and non-hospital). Those that do not meet all of the postulates proposed in this definition should be called Emergency Services.
• Triage:10
Triage is defined as a selection process using critical thinking, in which trained personnel perform a rapid classification of patients upon arrival at the Emergency Services. The classification system used at the Institution is the Canadian Triage Acuity Scale System (CTAS), which classifies patients into 5 categories according to the severity of the patients; category 1 being the most serious and category 5 the non-urgent.
• Assessment: this is the first time a patient is seen by a doctor.9
• Reassessments: are the number of subsequent times a patient is seen after the initial assessment.9
The variables analyzed were number of assessments, revaluations, SEM discharge diagnoses, disposition of patients, as well as number of admissions in the different functional areas of the SEM during the pandemic. In addition to the number of admissions during 2019 and 2020, the “category according to the severity of the patient” was a variable analyzed, as well as another variable is the “status” of the patient admitted.
The data were extracted from the Emergency Health Cube of the Health Statistics Area of the CCSS and the data analysis was performed with Excel Microsoft 365. In order to allow analysis and trends in SEM care during 2020 data from 2019 were obtained in order to demonstrate the differences between periods prior to the declaration of the pandemic. A descriptive statistics analysis was performed with frequency and proportion calculations.
Results
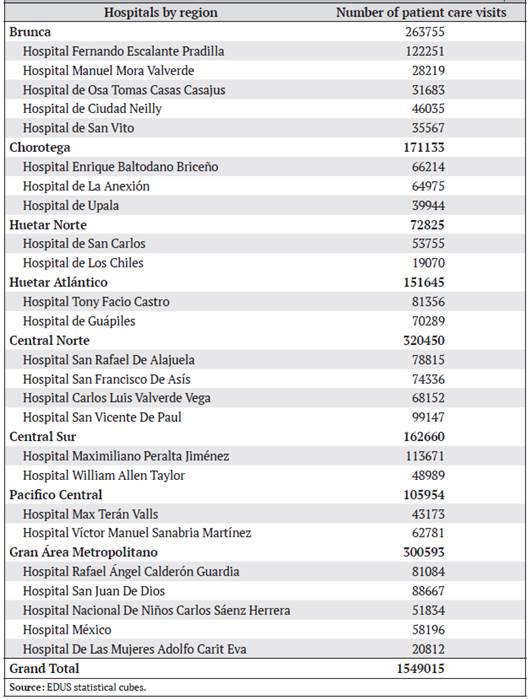
Twenty-five SEM that met the technical definition were included in the analysis. Admissions during the study period were 1,549,024 million visits. The range of cases ranged from 19,070,000 to 122,251,000 during the study period. The lowest number of visits corresponds to a peripheral hospital and the highest number to a regional hospital. Regarding the gender of the patients who consulted the SEM during 2020, it was observed that 850,707 (54.9%) were female.
As can be seen in Figure 1, when comparing the number of care visits in 2019 with the year 2020, a reduction of approximately 50% is observed, being more marked during the month of March when the pandemic is declared.
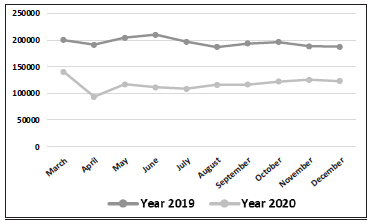
Figure 1 Emergency Services Admissions at the CCSS from March 1 to December 31, 2019, and 2020. Source: Statistical cubes of EDUS (Digital Health Record).
The greatest number of patients admitted in the SEM were between the ages of 20 and 44 years with 693,379 (44.7%), followed by the group between 45 and 64 years with 328,979 (21.2%) and finally those over 65 years with 205,485 (13.2%).
Patients under 18 years of age accounted for 20.7% (321,135) of the total number of visits. The number of assessments during 2020 corresponded to 1,549,024 and the number of revaluations to 4,038,029.
Regarding the classification of the acuity of the patients by means of the CTAS system, 40% (620,449) were classified as category 3, 39.8% (616,855) category 4, 14% (218,124), 5.3% (82,360) category 2 and finally 0.6% (9206) patients as category 1. The hospitals with the highest severity (category 1) according to the findings were those in the Huetar Atlantico Region (3,433) and those in the Greater Metropolitan Area (1,704).
Of all the patients seen in SEM during 2020, most of them were discharged directly from the Emergency Services (1,357,953; 87.67%) and a total of 161,075 (10.4%) required hospitalization. There were 4702 patients reported to have died in SEM,
with a mortality rate of 2.8% per 1000 admissions.
Two hundred and forty-nine thousand two hundred and eighty patients required a stay in the emergency observation area. When compared to 2019 as seen in Table 2, there was an increase in the percentage of patients requiring SEM observation and hospitalization.
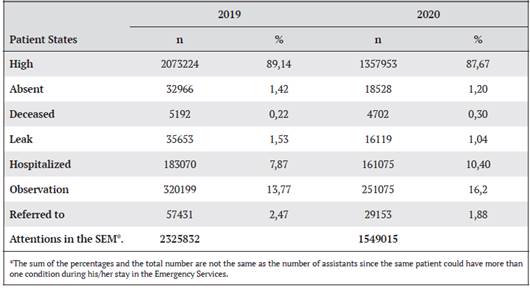
Figure 2 shows how the decrease in emergency care began earlier in relation to the increase in COVID-19 cases, and despite the sustained increase in positive cases, no major drop in consultations was observed in the second half of the year.
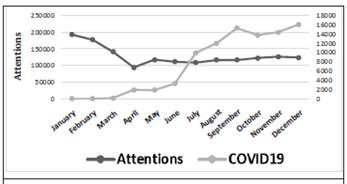
Figure 2 Total Emergency Services admissions versus COVID-19- related admissions reported in the Emergency Services of the Caja Costarricense del Seguro Social during the year 2020.
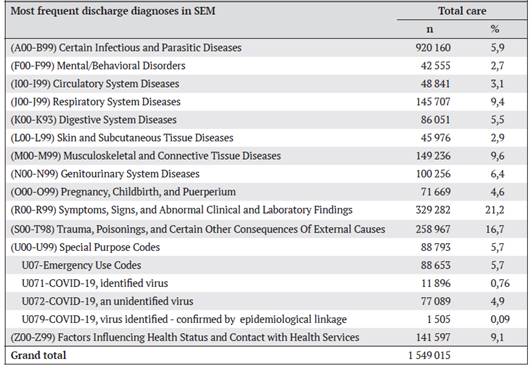
The most frequent diagnoses of patients discharged from SEM according to the ICD-10 list are shown in Table 3. The three most frequent diagnoses were pathologies associated with abnormal and laboratory symptoms and signs (n=xx, xx%), trauma-poisoning (n=xx, xx%), and musculoskeletal and connective tissue diseases (n=xx, xx%). With respect to patients with the diagnosis associated with SARS CoV-2, it was observed that 88 793 patients in the emergency services had such diagnoses during the study period.
Discussion
Emergency Services are a vital resource to ensure the delivery of health services to users with the most critical conditions. During the pandemic, SEM care worldwide decreased for a variety of reasons, including public fear of contagion in health care facilities. This study documented a decrease of almost 50% in SEM visits when compared to the same period in 2019.
One of the most interesting studies concerning care in Emergency Services was that carried out in the United States, in which a comparison was made of the health systems in 5 states, including emergency admission, before and during the pandemic due to COVID-19. In this study, it was found that the amount of care in this group of health systems before the pandemic ranged annually between 13,000 in Maryland, which had the lowest number, and 115,000 thousand in Springfield. In the month of March, there was a significant decrease in the number of visits by the population to Emergency Services, contrasting with an increase in suspected or positive cases of COVID-19, this decrease could be explained, according to the authors, by fear of the population to go to these services and risk of contagion, or being aware that other people required these services as a priority. 11
A similar study, conducted at Hamad Medical Corporation (the public health system that provides approximately 90% of emergency care in the State of Qatar), documented that the number of requests for Hospital Emergency Services has also been affected in those latitudes, with a decrease in requests during the initial months of the pandemic. 12
The first COVID-19 patient in Qatar was diagnosed on February 29, 2020. This study determined the number of individuals presenting to an Emergency Services during March-April 2020 and compared it to March-April 2019, and a decrease in admissions was observed between 20-43% compared to 2019; like what was found in our country.12
Latin America does not escape this phenomenon, as described by Dr. Luis Toro Cabrera, from the Hospital Clínico Universidad de Chile; an analysis was made of the care provided in all public Emergency Services from January 1, 2015, to May 3, 2020, mainly due to causes derived from respiratory and cardiovascular diseases (myocardial infarction, stroke, and hypertensive crisis). The drop-in care coincides with the beginning of the pandemic. 13
These findings are very significant for Emergency Services, in that there is a risk of not treating these entities in a timely manner, and therefore producing permanent complications, death, or a subsequent rebound effect in the number of consultations to health services in a post-pandemic scenario that exceeds the capacity of the Services.
Some studies point out as a possible explanation for the decrease in Emergency Services consultations concomitant with the increase in cases of COVID-19, the fear of the population to go to these services due to the risk of exposure to COVID-19, fear of long waiting times, or being aware that other people required these services as a priority.11 Administrative decisions that tend to divert patients with less urgent conditions to other areas of care in the health system have also been suggested as a contributing factor in the decrease in emergency consultations. In our case to the first level of care.12 Other factors that may add to this decrease in the number of cases in the Emergency Services are the changes in the activity patterns of the population during the pandemic. For example, the decrease in mobility during periods of closure, and this in turn has an impact on the decrease in occupational accidents, traffic accidents, and other types of trauma, as well as less risk of acquiring other types of infectious diseases.14
During the pandemic, all Emergency Services had to sectorize areas for the management of patients with COVID-19, and worldwide it was also necessary. In health systems such as the General Hospital in Singapore with 1758 beds and 130,000 annual Emergency Services admissions, there was a need to divide both triage and observation areas for patients suspected and non-suspected for COVID-19 disease, as well as observation areas. 15
The level of “hospital systems” that involve several Emergency Services under single management is described in the study of “Emory University Healthcare System”, which has seven hospitals (seven Emergency Services) with a total of 500 thousand admissions per year; in this system, the classification area was also sectorized, the workflows were changed as well as the strengthening of human resources involving physicians from other specialties in the care of the pandemic. 5
Limitations of the Study
The main limitations of this study were its retrospective nature and the fact that the information was extracted from the cube system, which does not allow us to detail more information on the patients who consulted in the SEM during the year 2020. Although the year of the beginning of the pandemic was analyzed, the pandemic is still ongoing, so this phenomenon and its impact on SEM continues during 2021, which means that at the end of the pandemic this same analysis should be repeated.
Based on statistical information from our Institution, there is evidence of a reduction in the number of emergency room visits in all the country’s Emergency Services. This reduction is concomitant with the increase in COVID-19 cases in Costa Rica and the continuous plateau (no decrease in cases). However, the number of reevaluations per center comparing 2019 to 2020 remains similar. The downward trend in SEM consultations in Costa Rica reproduces the trends reported in the literature worldwide. The explanation for this phenomenon is multifactorial; however, to our knowledge, there are no published studies in our country that explain this phenomenon.
Many changes have had to be made to SEM for Pandemic care. Differentiated care in Emergencies is a widely endorsed, implemented, and successful strategy that has been developed worldwide. The strategies implemented in Emergency Services worldwide for the care of COVID 19 have invariably required the re-adaptation and/or increase of Human Resources. Through staff redeployment, new hires, training strategies, flexible schedules, and use of trainees, among others.
There are many “structural” changes in the Emergency Services, hospitalization, and the Health System in general, which will most likely have to be changed definitively and as a priority. Not only for the attention of this Pandemic, but also so that these systems are better prepared for future infectious events of any kind. Future studies are needed to analyze in greater detail the effects of the pandemic on the country’s emergency services, including 2021.
Abbreviations: CCSS (Caja Costarricense del Seguro Social), CTAS (Canadian triage acuity scale system), SEM (Emergency Services). Sources of support: None. Own financing.
Conflict of interest: No conflicts of interest. ayock@ccss.sa.cr
Referencias
1. Zhou P, Yang XL, Wang XG, Hu B, Zhang L, Zhang W, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020;579:270-3. [ Links ]
2. By the C-A-U-I-IG. Early indicators of intensive care unit bed requirement during the COVID-19 epidemic: A retrospective study in Ile-de-France region, France. PLoS One. 2020;15:e0241406. [ Links ]
3. Wee LE, Fua TP, Chua YY, Ho AFW, Sim XYJ, Conceicao EP, et al. Containing COVID-19 in the Emergency Department: The Role of Improved Case Detection and Segregation of Suspect Cases. Acad Emerg Med. 2020;27:379-87. [ Links ]
4. Whitwell K, Maynard R, Barry N, Cowling V, Sood T. Strategic planning and response to COVID-19 in a London emergency department. Emerg Med J. 2020;37:567-70. [ Links ]
5. Yaffee AQ, Peacock E, Seitz R, Hughes G, Haun P, Ross M, et al. Preparedness, Adaptation, and Innovation: Approach to the COVID-19 Pandemic at a Decentralized, Quaternary Care Department of Emergency Medicine. West J Emerg Med. 2020;21(6):63-70. [ Links ]
6. Rosenbaum L. The Untold Toll - The Pandemic’s Effects on Patients without Covid-19. N Engl J Med. 2020;382:2368-71. [ Links ]
7. De Filippo O, D’Ascenzo F, Angelini F, Bocchino PP, Conrotto F, Saglietto A, et al. Reduced Rate of Hospital Admissions for ACS during Covid-19 Outbreak in Northern Italy. N Engl J Med. 2020;383:88-9. [ Links ]
8. Hollander JE, Carr BG. Virtually Perfect? Telemedicine for Covid-19. N Engl J Med. 2020;382:1679-81. [ Links ]
9. (CASEM) CpeAdlSdE. INFORME TECNICO PARA EL FORTALECIMIENTO DE LA ATENCIÓN DE EMERGENCIAS EN LA CCSS - 2017. In: Social CCdS, editor. San José, Costa Rica2017. p. 19-36. [ Links ]
10. Beveridge R. CAEP issues. The Canadian Triage and Acuity Scale: a new and critical element in health care reform. Canadian Association of Emergency Physicians. J Emerg Med. 1998;16:507-11. [ Links ]
11. Jeffery MM, D’Onofrio G, Paek H, Platts-Mills TF, Soares WE, 3rd, Hoppe JA, et al. Trends in Emergency Department Visits and Hospital Admissions in Health Care Systems in 5 States in the First Months of the COVID-19 Pandemic in the US. JAMA Intern Med. 2020;180:1328-33. [ Links ]
12. Butt AA, Azad AM, Kartha AB, Masoodi NA, Bertollini R, Abou-Samra AB. Volume and Acuity of Emergency Department Visits Prior To and After COVID-19. J Emerg Med. 2020;59:730-4. [ Links ]
13. Luis Toro AP, Miriam Alvo. Epidemia de COVID-19 en Chile: impacto en atenciones de Servicios de Urgencia y Patologías Específicas. Rev Med chile. 2020;148:557-64. [ Links ]
14. Hartnett KP, Kite-Powell A, DeVies J, Coletta MA, Boehmer TK, Adjemian J, et al. Impact of the COVID-19 Pandemic on Emergency Department Visits - United States, January 1, 2019-May 30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:699-704. [ Links ]
15. Quah LJJ, Tan BKK, Fua TP, Wee CPJ, Lim CS, Nadarajan G, et al. Reorganising the emergency department to manage the COVID-19 outbreak. Int J Emerg Med. 2020;13:32 [ Links ]
Received: June 02, 2021; Accepted: September 13, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
