










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkActa Médica Costarricense
versión On-line ISSN 0001-6002versión impresa ISSN 0001-6012
Acta méd. costarric vol.63 no.3 San José jul./sep. 2021
http://dx.doi.org/10.51481/amc.v63i3.1133
Original
Selection method of rescue treatment in patients with HIV-1: response and survival
1
 http://orcid.org/0000-0002-6231-1643
http://orcid.org/0000-0002-6231-1643
2
http://orcid.org/0000-0002-8877-5155
3
http://orcid.org/0000-0003-1492-8187
4
http://orcid.org/0000-0001-7318-7206
1Instituto de Medicina Tropical “Pedro Kouri”. Departamento de Asistencia Médica. La Habana. Cuba. 0000-0002-6231-1643
2Hospital Freyre Andrea. Departamento de Asistencia Médica. La Habana. Cuba. 0000-0002-8877-5155
3Instituto de Medicina Tropical “Pedro Kouri”. Departamento de Asistencia Médica. La Habana. Cuba. 0000-0003-1492-8187
4Instituto de Medicina Tropical “Pedro Kouri”. Departamento de Microbiología. La Habana. Cuba. 0000-0001-7318-7206
5Instituto de Medicina Tropical “Pedro Kouri”. Departamento de Microbiología. La Habana. Cuba. 0000-0001-7878-7542
6Instituto de Medicina Tropical “Pedro Kouri”. Departamento de Epidemiología y Estadística. La Habana. Cuba. 0000-0001-9231-7109
Sources of support:
No financial contributions were received from outside for the authors; authorized databases were used from the Instituto de Medicina Tropical “Pedro Kouri”.
Conflict of interest: The authors declare that there are no conflicts of interest.
Toxicity, non-adherence, and resistance are factors that can limit the efficacy and safety of TARGA, the latter being the main cause of therapeutic failure and therefore a threat to the sustained impact of ART, contributing to therapeutic failure. Resistance to TARGA is the total or partial loss of susceptibility to antiretrovirals, being an evolutionary viral adaptive mechanism (World Health Organization, HIV drug resistance report 2019. http://apps.who.int/iris/bitstre am/10665/255896/1/9789241512831-eng.pdf).
Resistance studies to drugs used in the treatment of HIV infection are a fundamental tool for the correct monitoring and follow-up of patients. There are two types of resistance studies: genotypic and phenotypic, the former is more commonly used in routine clinical practice as they are cheaper, faster, and less complex to perform (UNAIDS. Geneva, Switzerland: UNAIDS; 2019. http://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_es.pdf).
In the 2019 World Health Organization (WHO) report on antiretroviral resistance, based on information obtained from 18 countries on different continents, 12 of them (Argentina, Eswatini, Cuba, Guatemala, Honduras, Namibia, Nepal, Nicaragua, New Guinea, South Africa, Uganda, and Zimbabwe) it was shown that more than 10% of the patients studied had pre-treatment resistance to non-nucleoside reverse transcriptase inhibitors (NNRTIs) (UNAIDS. Geneva, Switzerland: UNAIDS; 2019. http://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_es.pdf). The prevalence of antiretroviral resistance among individuals receiving TARGA varies, overall, between 3% and 29%, slightly higher among those who have received therapy for more than 48 months. Among populations with virologic failure to firstline ITINAN-based therapies, acquired resistance in the first 12 months (±3 months) ranges from 50% to 97%. Dual resistance to both ITINAN and nucleoside/nucleotide reverse transcriptase inhibitors (ITIAN) occurs in 21% to 91% of these patients in the same time period. Worryingly, an even higher prevalence of acquired resistance is found in patients treated with these regimens for more than 48 months (UNAIDS. Geneva, Switzerland: UNAIDS; 2019. http://www.unaids.org/sites/default/files/media_asset/ UNAIDS_FactSheet_es.pdf).
In Cuba, resistance reports from 2009 to 2013, indicated a high rate of resistance to TARV, both in treated and untreated patients; mainly to drugs used in Cuban first-line therapy; as well as the emergence of cross-resistance to the latest generation TARV1,2 (Ministry of Public Health. Cuba. Directorate of Medical Records and Health Statistics. Anuario Estadístico de Salud 2018 (Internet). http://files.sld. cu/dne/files/2018/05/Anuario_Estad%C3%ADstico_de_Salud_e_2018_edici%C3%B3n_2018.pdf).
Despite the great advances achieved in antiretroviral therapy against HIV, the emergence of resistance is one of the main threats to the sustained impact of antiretroviral therapy (ARVs) in Cuba.3
This imposes new challenges to the scientific community in the management of the disease. The correct use of Genotypic Resistance Tests (PGR) can play a fundamental role in the fight against this scourge. Therefore, it is of great importance to know the impact that the routine performance of this study has had on the response to treatment and the evolution of Cuban patients with TARV failure. It is also important to identify the subgroup of patients who can benefit most from PGR in the Cuban context, so it is vital for medical personnel to know the virological and immunological response, the occurrence of opportunistic diseases, and survival to salvage therapy of those patients infected with HIV-1 who had a previous therapeutic failure, depending on the form of a selection of salvage therapy: resistance tests or expert criteria.
Given the above, this study aimed to determine the influence of the way of selection of salvage therapy on the therapeutic response and long-term survival of HIV-1 infected patients who presented failure to antiretroviral therapy in IPK between the years 2012 and 2016.
Methods
Type of study: Cohort, analytical and retrospective, in patients infected with HIV-1, with therapeutic failure to ART who were treated at the Institute of Tropical Medicine “Pedro Kourí” during the years 2012 to 2016.
Study universe: all patients with HIV-1 infection and antiretroviral treatment maintained for at least 6 months, who were discussed at the National Commission for antiretroviral treatment based at the IPK, between the years 2012 and 2016.
Inclusion criteria: patients in virologic failure who were prescribed rescue TARGA and with viral load (VL) >1,000 copies per mL on two or more consecutive occasions.
Exclusion criteria: 1. patients with TARGA discontinuation two weeks prior to treatment change, 2. patients with previous PGR-based TARGA change, 3. patients who did not attend the followup visit 4. patients not adherent to treatment.
A total of 212 patients were selected and divided into two groups, according to the selection of salvage treatment: Group A: 107 patients with salvage treatment selected based on the PGR result, and Group B: 105 patients with salvage treatment selected on the basis of expert criteria. The expert criterion considered was the criterion of the National Antiretroviral Treatment Commission: any salvage treatment that is chosen without prior genotypic resistance testing and includes at least two new, potentially active drugs.
Outcome variables were taken into account as (a) virologic response at 6, 12, 12, 18, and 24 months after initiation of salvage therapy (complete virologic suppression CV ˂ 50 copies per mL and virologic failure CV ˃ 200 copies per mL); b) CD4+ cell response at 6, 12, 12, 18 and 24 months after initiation of salvage therapy (mean increase in CD4+ T cells/mm3; c) percentage of patients who achieved CD4+ T cells>200 cells/mm3 ; d) incidence of opportunistic diseases during the study period; and e) survival at 48 months.
Independent variables were considered as: a) genotypic test for resistance; b) demographic (age, sex, skin color); and c) clinical and laboratory variables at the time of initiation of salvage therapy (time of HIV diagnosis, time on ART, number of previous treatment regimens, previous exposure to three different ARV families, and baseline CD4+ T-cell count and CV).
Variables were studied before the change in rescue therapy and at 6, 12, 12, 18, and 24 months after the change in rescue therapy.
Information was obtained from the minutes of the National Antiretroviral Therapy Commission (TARV), the Sidatrat database (IPK Hospital database where all patients with a diagnosis of HIV infection are included) and the clinical records of the patients studied.
Data were entered directly into an Excel 2010 database (Microsoft Corporation, Redmond, Washington, USA) and exported to the SPSS 21 statistical package (IBM Corp., Chicago, Illinois, USA) for analysis.
Absolute numbers and some measures of central tendency were used, such as mean and median, with their respective standard deviations (SD). The Chi statistic was used2, the Relative Risk (RR) and Mann-Whitney U test, also called “Wilcoxon rank-sum test”, “Wilcoxon W test” or “Wilcoxon rank sum test”.
The probability of survival was analyzed using the Kaplan-Meier method. Survival curves were compared using the Mantel-Haenszel test (log rank), Wilcoxon exact test (Gehan) and Tarone-Ware.
Results
A total of 212 HIV-infected patients with TARGA treatment failure were studied. The two study groups were defined according to the way of selection of the salvage therapy used. Group A (n=107) received salvage antiretroviral therapy guided by PGR and group B (n=105) by expert judgment.
Table 1 shows the distribution of the patients studied according to general characteristics and how rescue therapy was selected prior to initiation of rescue therapy.
There were no significant differences between the general characteristics of the two groups of patients studied, which demonstrates the homogeneity between groups A and B when deciding how to select rescue therapy.
The evolutionary virological response obtained after salvage therapy for the two groups was analyzed by virological failure and suppression.
As illustrated in Figure 1, the percentage of patients in virologic failure at 6, 12, 12, 18, and 24 months after initiating treatment was significantly higher in Group B patients (63.6%, 61.10%; 53.30%, and 60.80%) compared to Group A patients (36.4%, 38.90%; 41.70%, and 39.20%), respectively.
When stratifying the results based on the number of previous treatment regimens received by patients at the time of the study (Figure 2), it was observed that the percentages of complete virologic suppression 6 months after initiating treatment decreased in patients in both groups to the extent that they had greater prior exposure to ART and, which, in turn, were better in patients in group A regardless of the number of previous treatment regimens, but the most significant difference with respect to those in group B was observed in patients who had received 2 previous treatment regimens 38% vs. 18% (p<0,005).
Table 1 General characteristics of patients in both study groups at the start of salvage therapy. IPK 2012-2016
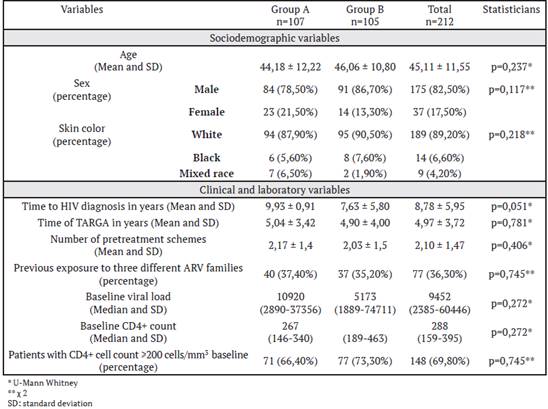
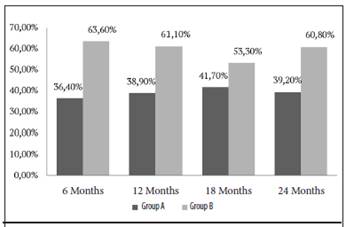
Figure 1 Percentage of patients with virologic failure according to the method used to choose treatment and time from initiation of salvage. IPK 2012-2016. Note that, in the group of patients to whom antiretroviral therapy was assigned based on genotypic resistance testing (Group A), the percentage of virologic failure was significantly lower for each of the cut-off times, compared to the group where selection was made under expert criteria (Group B).
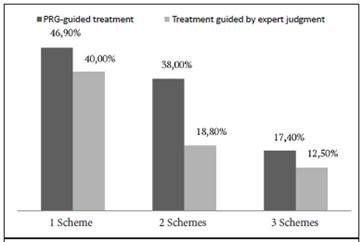
Figure 2 Percentage of patients with complete virologic suppression according to method used to choose treatment and number of previous treatment regimens. IPK 2012-2016. Three subgroups of patients were formed within each group, in relation to the number of antiretroviral therapy schemes previously used. Note that, regardless of the form used to select antiretroviral therapy, the greater the number of previous treatment schemes, the lower the percentage of patients who achieved complete virological suppression. In the subgroup where the form of treatment selection had the greatest impact was in which patients used two previous regimens.
A low percentage of patients in both groups with 3 or more previous treatment schemes achieved complete viral load suppression 17.40% and 12.50% for patients in groups A and B, respectively. Although the results were slightly better in patients who underwent PGR, the difference was not statistically significant (p<0.05).
Table 2 shows the CD4+ cell response to rescue therapy in patients in both study groups.
Group A patients had a more vigorous immune response than group B patients. The mean increase in CD4+ T lymphocytes was significantly higher in group A patients in all slices performed.
Although patients in Group B had slightly higher CD4+ numbers at baseline, higher percentages of patients achieving CD4+ counts ˃ 200 cells/mm3 were found in Group A, during case follow-up (Table 2). However, the differences were not significant.
Overall, opportunistic diseases were present in 15.56% of the patients studied. Table 3 shows that opportunistic diseases were diagnosed in 6 (5.60%) of the patients in Group A and in 27 (25.20%) of the patients in Group B (RR 5.827; CI 2.293-14.807; p<0.001), demonstrating a higher risk of incidence of opportunistic diseases in those treated under expert criteria.
Table 2 CD4+ cell response according to study group and time from initiation of salvage therapy. HIV patients in therapeutic failure. IPK 2012-2016
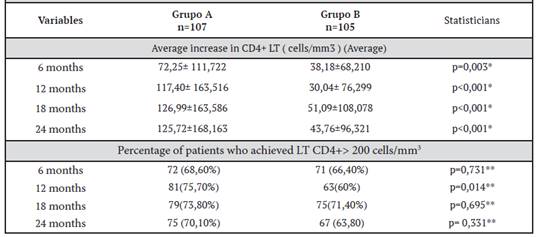
Table 3 Incidence of opportunistic diseases for each study group from the start of salvage therapy. Patients with therapeutic failure. IPK 2012-2016

Twenty-four patients died during the study period, which represents 11.3% of the total number of cases. The highest percentage was concentrated in group B, with 22 patients (21.0%) out of 105, compared to group A, where only 2 patients died (1.9%).
Kaplan-Meier curves demonstrate the impact of the introduction of salvage antiretroviral therapy, according to the form of choice, on the survival of HIV-1 infected patients in therapeutic failure during the 48 months of the investigation.
The highest percentage of cumulative survival was observed in group A patients with 98.1% at the end of the study, compared to group B patients with 79% in the same time (Figure 3 ).
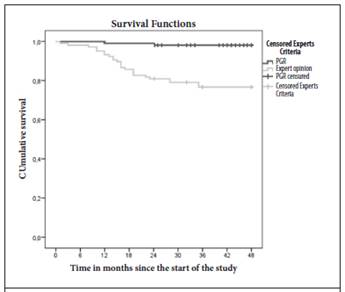
Figure 3 Kaplan-Meier Survival curves for patients in both study groups at 48 months. IPK 2012-2016. The highest percentage of cumulative survival was observed in the group that received the PGR-based treatment change with 98.1% at the end of the study, compared to the group treated based on expert judgment with 79% during the 48-month duration of the investigation.
When Log Rank was applied to determine the equality of distribution of survival, it was shown that there were statistically significant differences between the two groups: Log Rank = 20.26 (p<0.001); Generalized Wilcoxon = 19.21 (p<0.001) and Tarone-Ware = 19.73 (p<0.001).
Discussion
The sociodemographic characteristics of the patients included in the present study were like those described in the Cuban epidemic.4-7 Beyond making comparisons with studies carried out in other countries, it is important to focus the present investigation in the context of Cuba, with its sociocultural particularities and those of its health system.8
Some of the initial clinical studies failed to demonstrate the beneficial effect of resistance testing on virological response.9,10 In interpreting these results, it is important to bear in mind that knowledge of the genotypes predictive of response to treatment and the availability of drugs with activity against resistant virus were very limited at that time.
PGRs are currently an important part of the management of patients with HIV infection. Current national and international guidelines recommend performing such studies to optimize salvage treatment in patients with antiretroviral therapy failure (Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. Department of Health and Human Services. Available at www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL. pdf). However, the evidence supporting this recommendation is scarce or contradictory. The clinical studies consulted studied the short-term effect of PGRs on the virological and immunological response to salvage therapy,11,12 and very few studies evaluated the impact of PGRs on survival in HIV patients with extensive exposure to ART.13
The usefulness of resistance testing to guide antiretroviral drug selection in patients with virologic failure has been demonstrated. In general, changes in therapy based on resistance test results lead to better early virologic response than regimen changes guided by clinical judgment alone14,15 (Boillat-Blanco N, Darling KE, Schoni-Affolter F, et al. Virological outcome, and management of persistent low-level viraemia in HIV-1-infected patients: 11 years of the Swiss HIV Cohort Study. Virological outcome and management of persistent low-level viraemia in HIV-1-infected patients: 11 years of the Swiss HIV Cohort Study. Antivir Ther), as was also observed in this study.
After a first treatment failure, most patients have a large number of options for salvage antiretroviral drugs, which facilitates the choice of regimens with 2 or more potentially active drugs based solely on treatment history and knowledge of the resistance barrier of the drugs used,10 not so in those with failure to several ART regimens, who present complex drug resistance patterns and have few or no treatment options. In these patients the usefulness of resistance studies seems more limited.16
Another primary goal of ART is to achieveimmune reconstitution. The number of CD4+ T lymphocytes is the main indicator of the immune status of the person living with HIV (National Strategic Plan for the Prevention and Control of STIs and HIV/AIDS. MINSAP. Cuba 2014-2018 (PEN)).
Its measurement is particularly useful for monitoring treatment-naïve patients, defining the timing of ART initiation and the need to administer prophylaxis against opportunistic infections (OIs). Currently, ART is recommended for all patients regardless of viral load and CD4 + cell count (Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. Department of Health and Human Services. www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf ; Plan Estratégico Nacional para la Prevención y el Control de las ITS y el VIH/SIDA. MINSAP. Cuba 2014-2018 (PEN)).
It is recorded in the literature that the mean increase in CD4+ T-lymphocyte count in patients with therapeutic failure and rescue treatment based on PGRs is higher than in those in whom therapy is based on clinical judgment alone,9 as visualized in the present study.
However, some studies that evaluated the effectiveness of PGR in the therapeutic management of HIV-1-infected patients failed to demonstrate a beneficial effect on CD4+ cell response.4,14 One aspect that may have influenced the disparity of those results with those of the present investigation is the difference in terms of patient observation periods. In most of the studies consulted, the re-evaluation of CD4+ counts was performed 3 months after the change in antiretroviral treatment and in some it was extended to 6 months.4,11,14
Considering that immune restoration is a slow process that requires a relatively long time in virological suppression to be established, especially if one starts from very low CD4+ levels, longer evolutions in time are needed to be able to visualize it, (Grupo de estudio del SIDA-SIMC (GeSIDA). Consensus document of GeSIDA/National AIDS Plan regarding antiretroviral treatment in adults infected by the human immunodeficiency virus. Spanish Ministry of Health, Social Services, and Equality.
Government of Spain (Updated January 2019). In the current study, the follow-up time was extended to 24 months after the initiation of rescue treatment, so that the immunological restoration of the patients enrolled in the study could be better evidenced.
The ultimate goal of ART is to reduce the risk of OE and prevent death. At present, the development of opportunistic diseases or death from AIDS AIDSassociated diseases 6 months after initiation of an ART regimen is considered a clinical failure (Pérez J, Pérez D, Gonzalez I, Diaz Jidy M, Orta M, et al. Perspectives and practice in antiretroviral treatment. Approaches to the management of HIVAIDS in Cuba: a case study. Geneva: WHO. http://www.who.int/hiv/pub/prev_care/en/cuba.pdf. Accessed 27 May 2014).
The greater increase in CD4+ T lymphocytes in patients who underwent PGR appears to explain, at least in part, the differences between the study groups in the incidence of OE. Several prospective studies have shown that for patients living with the virus, CD4+ T lymphocyte counts < 200 cells/ mm3 represent a critical level below which the risk of opportunistic disease increases considerably (Perez J, Perez D, Gonzalez I, Diaz Jidy M, Orta M, et al. Perspectives and practice in antiretroviral treatment. Approaches to the management of HIVAIDS in Cuba: case study. Geneva: WHO. http://www.who.int/hiv/pub/prev_care/en/cuba.pdf. Accessed 27 May 2014).
The greater virologic suppression achieved by patients treated on the basis of PGR may also have contributed to the lower incidence of OEs in patients in this group during the study. It is known that some OEs, such as Pneumosystis jirovesi pneumonia (PCP), occur less frequently in patients with complete virologic suppression due to ART, even when they have not reached CD4 levels above 200 cells/mm3 (Panel on Opportunistic Infections in HIV-Infected Adults and Adolescents. Guidelines for the prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: recommendations from the Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. http://aidsinfo.nih.gov/contentfiles/lvguidelines/adult_oi.pdf).
Some OE such as opportunistic neoplasms, herpetic infections, and tuberculosis can appear even with CD4+ T lymphocyte counts above 200 cells/mm3, particularly in patients without treatment or with persistent viremia due to ART failure (Grupo de estudio del SIDA-SIMC (GeSIDA).
GeSIDA/National AIDS Plan consensus document on antiretroviral treatment in adults infected with human immunodeficiency virus. Spanish Ministry of Health, Social Services and Equality. Government of Spain (Updated January 2019)).
The use of PGRs in ART selection had a statistically significant impact on long-term patient survival, consistent with evidence from previous studies and other authors.17,18 This may have been mediated, at least in part, by the greater percentage increase in CD4+ counts, greater virologic suppression, and lower incidence of opportunistic disease in Group A of the study.
Patients in whom salvage therapy was chosen based on a genotypic test for resistance had a better virologic response, a greater increase in CD4+ T lymphocytes, and longer survival than those in whom treatment was chosen based on expert judgment.
Abbreviations: CD4+: CD4 T lymphocytes CV: viral load SD: Standard Deviation OE: opportunistic disease IPK: “Pedro Kourí” Institute of Tropical Medicine ITINAN: non-nucleoside reverse transcriptase inhibitor. RR: Relative Risk ART: antiretroviral therapy. HIV-1: Human Immunodeficiency Virus Type 1
tatianapd0201@gmail.com
Referencias
1 Kourí V, Alemán Y, Pérez L, Pérez J, Fonseca C, Correa C. High frequency of antiviral drug resistance and non-B subtypes in HIV-1 patients failing antiviral therapy in Cuba. J. Clin. Virol 2012; 55:348-55. [ Links ]
2 Perez L, Kouri V, Aleman Y, Abrahantes Y, Correa C, Arag ones C, et al. Antiretroviral drug resistance in HIV-1 therapy-naive patients in Cuba. Infection, genetics and evolution. Journal of molecular epidemiology and evolutionary genetics in infectious diseases. 2013; 16:144- 50. DOI: 10.1016/j.meegid.2013.02.002 [ Links ]
3 Perez L, Alvarez L, Carmona R, Aragones C, Delgado E, Thomson M, et al. Genotypic resistance to antiretroviral drugs in patients infected with several HIV type 1 genetic forms in Cuba. AIDS Res Hum Retroviruses 2007; 23: 407-14. [ Links ]
4 Gamero A, Martínez C, Margusino L, Martín I. Influencia de las pruebas de resistencias a antirretrovirales sobre la efectividad del tratamiento en pacientes con infección por VIH y fracaso virológico. Farm Hosp 2007; 31:23-29. [ Links ]
5 Franzetti M, Violin M, Antinori A, De Luca A. Trends and correlates of HIV-1 resistance among subjects failing an antiretroviral treatment over the 2003-2012 decade in Italy. BMC Infectious Diseases 2014, 14:398. http:// www.biomedcentral.com/1471-2334/14/398 [ Links ]
6 Lambert-Niclot S, George E, Pozniak A, White E, Schwimmer C, Jessen H, et al. Antiretroviral resistance at virological failure in the NEAT 001/ ANRS143 trial: raltegravir plus darunavir/ritonavir or tenofovir/emtricitabine plus darunavir/ ritonavir as first-line ART. Journal of Antimicrobial Chemotherapy. DOI: 10.1093/jac/dkv427 [ Links ]
7 Knyphausen F, Scheufele R, Ku ¨cherer C. First Line Treatment Response in Patients with Transmitted HIV Drug Resistance and Well Defined Time Point of HIV Infection: Updated Results from the German HIV-1 Seroconverter Study. 2014. 9. 5: e95956. [ Links ]
8 Reyes A, Mosquera M A, Bouza Y, Pérez J, y cols. Impacto de la terapia antirretroviral de alta eficacia en la respuesta clínica e inmunovirológica en enfermos SIDA. Revista Cubana de Medicina Tropical. 2007; 59:139-48. [ Links ]
9 Panidou ET, Trikalinos TA, Ioannidis JP. Limited benefit of antiretroviral resistance testing in treatment-experienced patients: a meta-analysis. AIDS 2004; 18:2153. [ Links ]
10 White KL, Raffi F, Miller MD. Análisis de resistencia de inhibidores de transferencia de cadena de integrasa en ensayos clínicos de fase 3 de pacientes sin tratamiento previo. Viruses Virus. Jul 2014; 6 (7): 2858-2879. http://www. ncbi.nlm.nih.gov/pubmed/25054884. [ Links ]
11 Durant J, Clevenbergh P, Halfon P, Delgiudice P, Porsin S, Simonet P, Montagne N, et al. Drug- resistance genotyping in HIV-1 therapy: the VIRADAPT randomised controlled trial. Lancet 1999; 353: 2195-9. [ Links ]
12 Grant P, Zolopa A. The use of resistance testing in the management of HIV-1-infected patients. Curr Opin HIV AIDS. 2009; 4: 474-80. [ Links ]
13 Lohse N. The road to success. Long-term prognosis for persons living with HIV in Denmark - time trends and risk factors. Dan Med J. 2016; 63: B5210. [ Links ]
14 Tural C, Ruiz L, Holtzer C, Schapiro J, Viciana P, González J, Domingo P, Boucher C, Rey-Joly C, Clotet B; Havana Study Group. Clinical utility of HIV-1 genotyping and expert advice: the Havana trial. AIDS 2002 Jan 25; 16:209-18. [ Links ]
15 Siliciano JD, Siliciano RF. Recent trends in HIV- 1 drug resistance. Curr Opin Virol. 2013; 3:487- 94. [ Links ]
16 De Luca A, Dunn D, Zazzi M, y col. Declining prevalence of HIV-1 drug resistance in antiretroviral treatment-exposed individuals in Western Europe. Disminución de la prevalencia de resistencia al fármaco VIH-1 en individuos expuestos al tratamiento antirretroviral en Europa occidental. J Infect Dis. J Infect Dis. Apr 15 2013; 207:1216-1220. DOI: 10.1093/infdis/ jit017 [ Links ]
17 Palella F; Armon Cl; Buchacz K, Cole S, Chmiel, J S, Novak R, et al. The Association of HIV Susceptibility Testing With Survival Among HIV-Infected Patients Receiving Antiretroviral Therapy: A Cohort Study. Annals of Internal Medicine.2009; 151:73-84. DOI: 10.7326/0003- 4819-151-2-200907210-00003 [ Links ]
18 Pou C, Noguera M J , Pérez S, García F, Delgado R, Dalmau D, y cols. Improved Prediction of Salvage Antiretroviral Therapy Outcomes Using Ultrasensitive HIV-1 Drug Resistance Testing. Clinical Infectious Diseases 2014; 59: 578-88. DOI: 10.1093/cid/ciu287 [ Links ]
Received: June 01, 2021; Accepted: October 20, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
